Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5835)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (350)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Clinical Procedures in Primary Eye Care-David Elliott - 158Document3 pagesClinical Procedures in Primary Eye Care-David Elliott - 158Danielle SangalangNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- An Introduction To Optometry: This Chapter Includes A Review ofDocument11 pagesAn Introduction To Optometry: This Chapter Includes A Review ofMwanja Moses100% (1)
- 9893 Alcon Grading Scales 4pp - 0 PDFDocument4 pages9893 Alcon Grading Scales 4pp - 0 PDFDanielle SangalangNo ratings yet
- Clinical Orthoptics - Fiona Rowe - 146Document6 pagesClinical Orthoptics - Fiona Rowe - 146Danielle SangalangNo ratings yet
- Grading Scales Web PDFDocument2 pagesGrading Scales Web PDFDanielle SangalangNo ratings yet
- Optical Math Handout RJohnson PDFDocument5 pagesOptical Math Handout RJohnson PDFRitesh Upadhyay100% (1)
- Corneal Injury Leads To Discovery: A Case Study On Asymptomatic AmblyopiaDocument1 pageCorneal Injury Leads To Discovery: A Case Study On Asymptomatic AmblyopiaDanielle SangalangNo ratings yet
- Volume 6, Issue 1 - 1Document10 pagesVolume 6, Issue 1 - 1Danielle SangalangNo ratings yet
- Acquired Infantile Horner Syndrome and Spontaneous Internal Carotid Artery Dissection: A Case Report and Review of LiteratureDocument10 pagesAcquired Infantile Horner Syndrome and Spontaneous Internal Carotid Artery Dissection: A Case Report and Review of LiteratureDanielle SangalangNo ratings yet
- Myopic Changes in A Climber After Taking Acetazolamide and The Use of Corrective Lenses To Temporize Symptoms: A Case Report From Mount KilimanjaroDocument4 pagesMyopic Changes in A Climber After Taking Acetazolamide and The Use of Corrective Lenses To Temporize Symptoms: A Case Report From Mount KilimanjaroDanielle SangalangNo ratings yet
- Advanced Slit Lamp Skills: How To Adjust The Lighting To See Stuff!Document45 pagesAdvanced Slit Lamp Skills: How To Adjust The Lighting To See Stuff!Danielle SangalangNo ratings yet
- A Course in Low Vision Practice: P 5 - Magnification and MagnifiersDocument6 pagesA Course in Low Vision Practice: P 5 - Magnification and MagnifiersDanielle SangalangNo ratings yet
- Alternating Horner Syndrome: Case Report and Review of The LiteratureDocument4 pagesAlternating Horner Syndrome: Case Report and Review of The LiteratureDanielle SangalangNo ratings yet
- Horner's Syndrome As A Complication of Thyroidectomy: Report of A CaseDocument3 pagesHorner's Syndrome As A Complication of Thyroidectomy: Report of A CaseDanielle SangalangNo ratings yet
- Horners Syndrome Resulting From Agenesis of The Internal Carotid Artery: Report of A Third CaseDocument2 pagesHorners Syndrome Resulting From Agenesis of The Internal Carotid Artery: Report of A Third CaseDanielle SangalangNo ratings yet
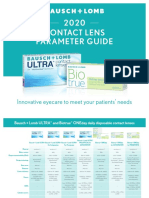
- 2020 Contact Lens Parameter Guide: Innovative Eyecare To Meet Your Patients' NeedsDocument4 pages2020 Contact Lens Parameter Guide: Innovative Eyecare To Meet Your Patients' NeedsDanielle SangalangNo ratings yet
- Clinical Optometry Primary Eye CareDocument3 pagesClinical Optometry Primary Eye CareDanielle SangalangNo ratings yet
- The Other Amsler ChartsFINALDocument20 pagesThe Other Amsler ChartsFINALDanielle SangalangNo ratings yet
- RPG Series Ophthalmology Buster PDFDocument299 pagesRPG Series Ophthalmology Buster PDFDanielle SangalangNo ratings yet
- Bino - Lec - Midterm Exam - Yellow - PadDocument11 pagesBino - Lec - Midterm Exam - Yellow - PadDanielle SangalangNo ratings yet
- Binocular Vision & Orthoptics - Bruce Evans - 17Document3 pagesBinocular Vision & Orthoptics - Bruce Evans - 17Danielle Sangalang0% (1)
- Institute For Career Research - Career As An Optometrist Doctor of Optomet PDFDocument33 pagesInstitute For Career Research - Career As An Optometrist Doctor of Optomet PDFDanielle SangalangNo ratings yet
- Best Aid To Ophthalmology - Pramod TK - 318Document3 pagesBest Aid To Ophthalmology - Pramod TK - 318Danielle SangalangNo ratings yet
- Manual of Squint-Leela Ahuja - 48Document19 pagesManual of Squint-Leela Ahuja - 48Danielle Sangalang100% (1)
- Handbook of Ophthalmology - Amar Agarwal - 159Document5 pagesHandbook of Ophthalmology - Amar Agarwal - 159Danielle SangalangNo ratings yet
- Flyer Symposium INOIIS X PERDAMI JabarDocument7 pagesFlyer Symposium INOIIS X PERDAMI JabarBonita AsyigahNo ratings yet
- Visual Impairment ScriptDocument3 pagesVisual Impairment Scriptapi-285548719No ratings yet
- DARE's Eye PDFDocument33 pagesDARE's Eye PDFvirag.patilNo ratings yet
- RIZALDocument3 pagesRIZALJed Daet0% (1)
- Peripheral Ulcerative KeratitisDocument145 pagesPeripheral Ulcerative KeratitisCarlos OrtegaNo ratings yet
- Thyroid OphthalmopathyDocument59 pagesThyroid OphthalmopathyLavanya MadabushiNo ratings yet
- Ipd B: Finals - Heent: Techniques of Examination For Head (From Bates')Document13 pagesIpd B: Finals - Heent: Techniques of Examination For Head (From Bates')Janica Marie Ragsac100% (2)
- Visual and Auditory DisturbancesDocument53 pagesVisual and Auditory DisturbancesJASTINE JOY PEREZNo ratings yet
- Management of GlaucomaDocument22 pagesManagement of GlaucomaRold Brio Sos100% (1)
- The Spotty RetinaDocument5 pagesThe Spotty RetinaJose Luis Mato AhcanNo ratings yet
- Cycloplegic Effect of 0.5%tropicamide and 0.5%phenylephrine Mixed Eye Drops - Objective Assessment in Japanese Schoolchildren With MyopiaDocument5 pagesCycloplegic Effect of 0.5%tropicamide and 0.5%phenylephrine Mixed Eye Drops - Objective Assessment in Japanese Schoolchildren With Myopiaal_dhi_01No ratings yet
- Laporan Kasus Tatalaksana Pembedahan Pada Pasien Dengan Eksotropia Sensoris - Novaqua YandiDocument13 pagesLaporan Kasus Tatalaksana Pembedahan Pada Pasien Dengan Eksotropia Sensoris - Novaqua YandiMeliNo ratings yet
- Retinal DetachmentDocument14 pagesRetinal DetachmentPui_Yee_Siow_6303No ratings yet
- Spec 1252557782Document6 pagesSpec 1252557782Mukarram AbdulnabeeNo ratings yet
- Pterygium After Surgery JDocument6 pagesPterygium After Surgery JRayhan AlatasNo ratings yet
- 2 - BPE - Eye ExaminationDocument50 pages2 - BPE - Eye ExaminationZauhar NurdildayevaNo ratings yet
- Photostress TestDocument2 pagesPhotostress TestAnumeha JindalNo ratings yet
- Fill-InDocument1 pageFill-InAnirudh SureshNo ratings yet
- A Clinical Study To Correlate Visual Field Defects With Optic Disc Changes in 100 Patients With Primary Open Angle Glaucoma in A Tertiary Eye Care HospitalDocument3 pagesA Clinical Study To Correlate Visual Field Defects With Optic Disc Changes in 100 Patients With Primary Open Angle Glaucoma in A Tertiary Eye Care HospitalIOSRjournalNo ratings yet
- Opmi Lumera IDocument19 pagesOpmi Lumera IUsman RahimNo ratings yet
- Eye Dissection Report Write Up 2014Document8 pagesEye Dissection Report Write Up 2014api-351895935No ratings yet
- Know The New Glaucoma Staging Codes PDFDocument2 pagesKnow The New Glaucoma Staging Codes PDFDinda Ayu YunitasariNo ratings yet
- WOC2010 FinalProgramDocument422 pagesWOC2010 FinalProgramgenrypolNo ratings yet
- IGCSE 0610 - EYES Sense Organs NOTES (2023-2025)Document4 pagesIGCSE 0610 - EYES Sense Organs NOTES (2023-2025)ckqx1234No ratings yet
- Brochure AladdinDocument20 pagesBrochure AladdinAchmad ShiddiqNo ratings yet
- Hyperopia: AuthorsDocument13 pagesHyperopia: AuthorsHana SetianingsihNo ratings yet
- At 030Document88 pagesAt 030Tuchilo ViorelNo ratings yet
- Karl Kaps Som62 Ophthal BrochureDocument8 pagesKarl Kaps Som62 Ophthal BrochureSaamyNo ratings yet
- 001 - SPECTRALIS Brochure OCT2 Insert - USDocument2 pages001 - SPECTRALIS Brochure OCT2 Insert - USMariano FioreNo ratings yet