Download as pdf or txt
You might also like
- SBST3203 Elementary Data AnalysisDocument8 pagesSBST3203 Elementary Data AnalysisSimon RajNo ratings yet
- OPT Plus Form 1Document2 pagesOPT Plus Form 1Crash Zerocool60% (10)
- DOLE Accredited OSH Training CentersDocument6 pagesDOLE Accredited OSH Training CentersAnonymous Xa8cEVV67% (3)
- OPT Plus Form 1Document1 pageOPT Plus Form 1ApOlle Defiesta - DOminguezNo ratings yet
- Executive Functions by Thomas Brown 1Document6 pagesExecutive Functions by Thomas Brown 1api-247044545No ratings yet
- OPT+ Form 1A List of Preschoolers W/ WT HT MeasurementDocument4 pagesOPT+ Form 1A List of Preschoolers W/ WT HT MeasurementSimoneides Macahis100% (1)
- OPT Full Weighing FormsDocument10 pagesOPT Full Weighing FormsDaphne Joyce EmbradoraNo ratings yet
- 12 OPT Plus Form 1B List of Affected at Risk Preschoolers 0 59 Months Old 5 CopiesDocument1 page12 OPT Plus Form 1B List of Affected at Risk Preschoolers 0 59 Months Old 5 CopiesExzur Chavez100% (2)
- Use WEIGHT-FOR-LENGTH or WEIGHT-FOR-HEIGHT To Correctly Determine Overweight and ObesityDocument3 pagesUse WEIGHT-FOR-LENGTH or WEIGHT-FOR-HEIGHT To Correctly Determine Overweight and ObesityExzur Chavez100% (1)
- OPT Plus Masterlist Form - Updated - Feb 2021Document2 pagesOPT Plus Masterlist Form - Updated - Feb 2021Jolland Palomares Sumalinog100% (4)
- BNS Form No. 7Document31 pagesBNS Form No. 7jimmy jardinez100% (2)
- 9 BNS Form No. 7 Full Weighing Report 5 CopiesDocument1 page9 BNS Form No. 7 Full Weighing Report 5 CopiesExzur ChavezNo ratings yet
- eOPT Tool For Barangay or Purok - 500children-11Document313 pageseOPT Tool For Barangay or Purok - 500children-11Ivy EveByang0% (2)
- HAPAG-ASA FILL UP FORM MANA PACK REPORT CabiraoanDocument2 pagesHAPAG-ASA FILL UP FORM MANA PACK REPORT CabiraoanJeferson SardengNo ratings yet
- BLANK BPOC Monitoring Form No. 2Document1 pageBLANK BPOC Monitoring Form No. 2junayrah galmanNo ratings yet
- DTR JO CasualDocument1 pageDTR JO CasualPoblacion 04 San LuisNo ratings yet
- Template BHW Registry Form 2023Document6 pagesTemplate BHW Registry Form 2023daisy1279.dds165No ratings yet
- Harmonized Household Profiling Tool Ver2021Document4 pagesHarmonized Household Profiling Tool Ver2021Marissa Comingking Recaña100% (2)
- Master List of Households On Environmental Health and SanitationDocument6 pagesMaster List of Households On Environmental Health and SanitationFanelyn Lambus Gravamen0% (1)
- Roster of Beneficiaries/Availees (Ra 11261 - First Time Jobseekers Act) Barangay Lussoc, Santo Domingo, Ilocos SurDocument2 pagesRoster of Beneficiaries/Availees (Ra 11261 - First Time Jobseekers Act) Barangay Lussoc, Santo Domingo, Ilocos SurJorge DanielleNo ratings yet
- VAW Desk Form 1Document3 pagesVAW Desk Form 1desiree joy corpuzNo ratings yet
- Office of The Mayor: Barangay ProfileDocument4 pagesOffice of The Mayor: Barangay Profilemichael ricafortNo ratings yet
- DTR Tupad 390Document1 pageDTR Tupad 390Arman Bentain100% (1)
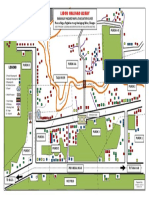
- Libod Malinao Albay: Barangay Hazard Map & Evacuation GuideDocument1 pageLibod Malinao Albay: Barangay Hazard Map & Evacuation Guideiricamae ciervoNo ratings yet
- LUPONDocument1 pageLUPONDindo Ojeda100% (1)
- Weight Monitoring FormDocument1 pageWeight Monitoring FormChristopher Torres50% (2)
- Roster of Beneficiaries Availees EditableDocument1 pageRoster of Beneficiaries Availees EditableEirrehc Ronacin100% (1)
- SGLGB Form 1 Barangay ProfileDocument3 pagesSGLGB Form 1 Barangay ProfileMark Lenon Par Mapaye100% (1)
- Post Activity Report CleanUp DriveDocument2 pagesPost Activity Report CleanUp DriveJoshua Regalado100% (2)
- BHW Solicitation LetterDocument1 pageBHW Solicitation LetterCheska MarieNo ratings yet
- 4Ps BARANGAY CERTIFICATIONDocument1 page4Ps BARANGAY CERTIFICATIONBarangay Taguitic100% (2)
- Barangay Health Worker Registration FormDocument1 pageBarangay Health Worker Registration FormJairah Marie100% (2)
- Authority To Purchase Garbage TruckDocument1 pageAuthority To Purchase Garbage TruckApple PoyeeNo ratings yet
- Bpops Plan SampleDocument4 pagesBpops Plan SampleQUeen Dai SY RamirezNo ratings yet
- Annex B PPAN Accomplishment Report Template BarangayDocument2 pagesAnnex B PPAN Accomplishment Report Template Barangayrandy hernandez100% (1)
- Annex A - Advisory - Barangay Road Clearing - Monthly Cumulative Monitoring Report - Jan 6Document1 pageAnnex A - Advisory - Barangay Road Clearing - Monthly Cumulative Monitoring Report - Jan 6잔돈100% (1)
- OPT Plus Form 1. List of Preschoolers With Weight and Height Measurement and Identified Nutritional StatusDocument16 pagesOPT Plus Form 1. List of Preschoolers With Weight and Height Measurement and Identified Nutritional StatusLei Koyou100% (1)
- Accomplishment Report of Barangay Messenger 2023Document1 pageAccomplishment Report of Barangay Messenger 2023mycel poloyapoyNo ratings yet
- Barangay Sinabaan Barangay Protection OrderDocument1 pageBarangay Sinabaan Barangay Protection OrderOmar Dizon IINo ratings yet
- Barangay Certification: Office of The Punong Barangay Barangay Jugno CouncilDocument1 pageBarangay Certification: Office of The Punong Barangay Barangay Jugno CouncilMarivic Donque Sienes100% (1)
- Certificate of Indigency - Low Income - New Format 2023Document1 pageCertificate of Indigency - Low Income - New Format 2023Barangay Magsaysay Parang100% (2)
- Certification For VawcDocument1 pageCertification For Vawcrafael solamNo ratings yet
- EOPT Tool For Barangay or Purok - 1000children1Document492 pagesEOPT Tool For Barangay or Purok - 1000children1Gillian Dale71% (7)
- 1601EQ 2nd Qtr. 2019 PDFDocument2 pages1601EQ 2nd Qtr. 2019 PDFmarifel barinqueNo ratings yet
- Bns 0-23 MonthsDocument2 pagesBns 0-23 MonthsApril Joy Sumagit Hidalgo100% (1)
- Bdrrm-Eo Barangay AmobocanDocument7 pagesBdrrm-Eo Barangay AmobocanJasper Quilang CiriacoNo ratings yet
- JetmaticDocument1 pageJetmaticRue BeeNo ratings yet
- Letter To Request Kasalan ParokyaDocument2 pagesLetter To Request Kasalan ParokyaArniel Fred Tormis FernandezNo ratings yet
- Opt Vit A. and Deworming FormDocument1 pageOpt Vit A. and Deworming Formelyss100% (1)
- 2022 Moa Tree ParkDocument2 pages2022 Moa Tree ParkAnne Socorro AbellanosaNo ratings yet
- Resolution 2020Document337 pagesResolution 2020Jovelyn AlaNo ratings yet
- Pweding I-EditDocument14 pagesPweding I-EditChristopher Torres100% (1)
- Aksyon Barangay Kontra Dengue (Abkd)Document1 pageAksyon Barangay Kontra Dengue (Abkd)jane franciscoNo ratings yet
- Orientation For The 2024 POPCEN CBMS BPQ Data Collection and SFGP Listing - 20240508Document65 pagesOrientation For The 2024 POPCEN CBMS BPQ Data Collection and SFGP Listing - 20240508Barangay CalaocanNo ratings yet
- Office of The Punong BarangayDocument1 pageOffice of The Punong BarangayBarangay Pangil100% (1)
- KP Form 28 TransmittalDocument39 pagesKP Form 28 TransmittalBarangay Magsaysay ParangNo ratings yet
- Certificate For Senior CitizenDocument1 pageCertificate For Senior CitizenVan Na Diz100% (1)
- The Barangay Mission & Vision Statement 2019Document4 pagesThe Barangay Mission & Vision Statement 2019Babuu BabuuNo ratings yet
- Republic of The Philippines Province of Iloilo Municipality of Lambunao BarangayDocument1 pageRepublic of The Philippines Province of Iloilo Municipality of Lambunao BarangayCarla Naural-citeb0% (1)
- Sta. Rosa - Certification - Senior CitizenDocument1 pageSta. Rosa - Certification - Senior CitizenJohny VillanuevaNo ratings yet
- Assessment Tool For BDRRMC - SimplifiedDocument2 pagesAssessment Tool For BDRRMC - Simplifiedmyrna teNo ratings yet
- Certification: Barangay Uep Zone IiDocument1 pageCertification: Barangay Uep Zone IiNimrodBanawisNo ratings yet
- OPT+ Weight For Age StatDocument3 pagesOPT+ Weight For Age StatSimoneides MacahisNo ratings yet
- Lgu SWM Scmar Revised March 2016 Annex ADocument2 pagesLgu SWM Scmar Revised March 2016 Annex ABrgy. Roxas100% (1)
- Monthly Barangay Consolidated Kasambahay Report For The Month of August 2020 Barangay: Mun. /city: Province: RegionDocument2 pagesMonthly Barangay Consolidated Kasambahay Report For The Month of August 2020 Barangay: Mun. /city: Province: RegionBrgy. Roxas100% (2)
- Vawc New Format QuarterlyDocument1 pageVawc New Format QuarterlyBrgy. Roxas100% (2)
- Revitalization of Barangay Anti-Drug Abuse Council (Badac)Document3 pagesRevitalization of Barangay Anti-Drug Abuse Council (Badac)Brgy. RoxasNo ratings yet
- Output Schedule of Implementation Fianancial Accomplishment: Barangay: Region: Province: MunicipalityDocument2 pagesOutput Schedule of Implementation Fianancial Accomplishment: Barangay: Region: Province: MunicipalityBrgy. RoxasNo ratings yet
- Kasambahay Form 2Document2 pagesKasambahay Form 2Brgy. Roxas83% (6)
- VAWC NEW FORMAT QuarterlyDocument1 pageVAWC NEW FORMAT QuarterlyBrgy. Roxas75% (4)
- Lgu SWM Scmar Revised March 2016 Annex ADocument2 pagesLgu SWM Scmar Revised March 2016 Annex ABrgy. RoxasNo ratings yet
- EthicsDocument6 pagesEthicsKyhl lourence ViernesNo ratings yet
- Mono Ethylene GlycolDocument9 pagesMono Ethylene GlycolAdminpp MpwkepriNo ratings yet
- 2011 NEC Code Changes HandbookDocument33 pages2011 NEC Code Changes HandbookBlackie KnightNo ratings yet
- ABHISHEK GANGULI - NTCC - IMPACT OF STUDENTS MENTAL HEALTHDocument36 pagesABHISHEK GANGULI - NTCC - IMPACT OF STUDENTS MENTAL HEALTHPriyanshu KumarNo ratings yet
- MPH Curriculum ExampleDocument3 pagesMPH Curriculum ExampleMark EbrahimNo ratings yet
- Research Output No. 1Document7 pagesResearch Output No. 1Jigz JimenezNo ratings yet
- Both HLKLDocument1 pageBoth HLKLbesoNo ratings yet
- Soal UTS - Advanced Reading and Writing - ELB4B3 - 160524 - 145417Document5 pagesSoal UTS - Advanced Reading and Writing - ELB4B3 - 160524 - 145417shenny sitindjakNo ratings yet
- Professional Teachers - ELEMENTARY 09-2023Document123 pagesProfessional Teachers - ELEMENTARY 09-2023PRC Baguio100% (2)
- Ascariasis: Roundworm Ascaris LumbricoidesDocument18 pagesAscariasis: Roundworm Ascaris LumbricoidesSuneel Kumar PrajapatiNo ratings yet
- HANDOUT ON Care of Eye and Care of Nails and FeetDocument4 pagesHANDOUT ON Care of Eye and Care of Nails and Feetchaitali shankarNo ratings yet
- Community Risk assessment-HCVA-PCVA - For Pasig City PDFDocument62 pagesCommunity Risk assessment-HCVA-PCVA - For Pasig City PDFBoie SantosNo ratings yet
- A Handbook of Menstrual Diseases in Chinese MedicineDocument1,225 pagesA Handbook of Menstrual Diseases in Chinese MedicineJeffrey Paardekooper0% (1)
- CB ReportDocument6 pagesCB ReportArshad JamilNo ratings yet
- Nosh AspirinDocument37 pagesNosh Aspirincharm_yashikaNo ratings yet
- Task 2 - Sustainability Report IKEA 2020Document3 pagesTask 2 - Sustainability Report IKEA 2020Aurora Azzahra100% (1)
- PHD Thesis in Health InformaticsDocument4 pagesPHD Thesis in Health Informaticsfjbnd9fq100% (2)
- Kesehatan Mental Dan Strategi Koping Dalam Perspektif Budaya: Sebuah Studi Sosiodemografi Di Kampung AminweriDocument16 pagesKesehatan Mental Dan Strategi Koping Dalam Perspektif Budaya: Sebuah Studi Sosiodemografi Di Kampung AminweriScritte SNo ratings yet
- Social Media AddictionDocument27 pagesSocial Media AddictionChristy TayagNo ratings yet
- PECELPPF333004A2Document17 pagesPECELPPF333004A2RuddyNo ratings yet
- Q4 Lesson 4 Diseases Brought About by Animals, InsectsDocument15 pagesQ4 Lesson 4 Diseases Brought About by Animals, InsectsLudwig Van Tamayo NumockNo ratings yet
- RUNDOWN Ilmiah TGL 29 Sept 2020Document8 pagesRUNDOWN Ilmiah TGL 29 Sept 2020rodtobingNo ratings yet
- Current Issues Paper - Sexual Identification Gender IdentityDocument6 pagesCurrent Issues Paper - Sexual Identification Gender Identitytania molinaNo ratings yet
- MSDS Loctite Nordbak Wearing Compound ResinDocument6 pagesMSDS Loctite Nordbak Wearing Compound ResinSadamNo ratings yet
- Building A Bridge The Right Way PDFDocument6 pagesBuilding A Bridge The Right Way PDFsteppenwolf88No ratings yet
- CEN 1-19 - Level-6 - DV ROUND 4 Schedule Publishing Document 06-07-2023Document2 pagesCEN 1-19 - Level-6 - DV ROUND 4 Schedule Publishing Document 06-07-2023Lalit Prabh AnandNo ratings yet
- Redundant Publication, Selective Reporting and Misrepresentation of DataDocument39 pagesRedundant Publication, Selective Reporting and Misrepresentation of Dataphd21306001 Ayushi GargNo ratings yet