Download as pdf or txt
You might also like
- Maths No ProblemDocument14 pagesMaths No ProblemJamila Mammadova100% (2)
- Method Statement Stone ColumnDocument10 pagesMethod Statement Stone ColumnSantosh ZunjarNo ratings yet
- Chronic Suppurative Otitis Media in AdultsDocument10 pagesChronic Suppurative Otitis Media in AdultsRstadam TagalogNo ratings yet
- Hauptwerk Installation and User GuideDocument316 pagesHauptwerk Installation and User Guideanubis7770% (1)
- A Comparative Study of The Obligation of PDFDocument658 pagesA Comparative Study of The Obligation of PDFYoussefdrm BessadimrNo ratings yet
- Schwannoma Vestibular TinnitusDocument6 pagesSchwannoma Vestibular TinnitusThomasMáximoMancinelliRinaldoNo ratings yet
- Omsk DGN SNHLDocument4 pagesOmsk DGN SNHLdinaNo ratings yet
- Jurnal 1 Titin SuhartinaDocument8 pagesJurnal 1 Titin SuhartinaTitinNo ratings yet
- Wideband Acoustic Absorbance in Otosclerosis Does Stapedotomy Restore Normal Tympanic Cavity FunctionDocument8 pagesWideband Acoustic Absorbance in Otosclerosis Does Stapedotomy Restore Normal Tympanic Cavity FunctionZoe RgNo ratings yet
- 2010 Grossi Pycnogenol Improves Tinnitus SymptomsDocument5 pages2010 Grossi Pycnogenol Improves Tinnitus Symptomsjulian_rosengrenNo ratings yet
- En A13v73n5Document4 pagesEn A13v73n5Tessa Septian AnugrahNo ratings yet
- Medicine: Characteristics of Hearing Loss in Patients With Herpes Zoster OticusDocument6 pagesMedicine: Characteristics of Hearing Loss in Patients With Herpes Zoster OticusnabilulhakNo ratings yet
- Extended High Frequency Hearing Loss in Tinnitus-Positive Chronic Suppurative Otitis Media PatientDocument5 pagesExtended High Frequency Hearing Loss in Tinnitus-Positive Chronic Suppurative Otitis Media PatientadindaNo ratings yet
- Hearing Loss AssessmentDocument31 pagesHearing Loss AssessmentKIBET ERNEST MUTAINo ratings yet
- Restoration of Hearing LossDocument10 pagesRestoration of Hearing LossZhungli QuanNo ratings yet
- Audiologic Characteristics of Hearing and Tinnitus in Occupational Noise-Induced Hearing Loss PDFDocument5 pagesAudiologic Characteristics of Hearing and Tinnitus in Occupational Noise-Induced Hearing Loss PDFKaty Marlen GongoraNo ratings yet
- Healthcare 11 00676 v2Document10 pagesHealthcare 11 00676 v2andiNo ratings yet
- Correlation Between Sensorineural Hearing Loss andDocument5 pagesCorrelation Between Sensorineural Hearing Loss andWilson WibisonoNo ratings yet
- EgyptJOtolaryngol313162-8588218 235122Document8 pagesEgyptJOtolaryngol313162-8588218 235122G RAVIKISHORENo ratings yet
- Nasopharyngeal Cancer Mimicking Otitic Barotrauma in A Resource-Challenged Center: A Case ReportDocument5 pagesNasopharyngeal Cancer Mimicking Otitic Barotrauma in A Resource-Challenged Center: A Case ReportikbalsidiqNo ratings yet
- Upper Airway Obstructions and Chronic Otitis Media: A Clinical StudyDocument4 pagesUpper Airway Obstructions and Chronic Otitis Media: A Clinical StudyMuhammadImamNo ratings yet
- Sensorineural Hearing Loss in Mucosal Type of Chronic Otitis MediaDocument4 pagesSensorineural Hearing Loss in Mucosal Type of Chronic Otitis MediaIla MahiraNo ratings yet
- tmp9718 TMPDocument6 pagestmp9718 TMPFrontiersNo ratings yet
- Atelectasis 1Document17 pagesAtelectasis 1Arief FakhrizalNo ratings yet
- 9009 44225 1 PB PDFDocument5 pages9009 44225 1 PB PDFwandajunitasNo ratings yet
- Electronic Physician (ISSN: 2008-5842) : 1.1. BackgroundDocument5 pagesElectronic Physician (ISSN: 2008-5842) : 1.1. BackgroundFi NoNo ratings yet
- Surgical Treatment of Tympanosclerosis: Tympanosclerosis in The Rat Tympanic Membrane: An Experimental StudyDocument10 pagesSurgical Treatment of Tympanosclerosis: Tympanosclerosis in The Rat Tympanic Membrane: An Experimental StudyAamir YousufNo ratings yet
- OtosclerosisDocument9 pagesOtosclerosisHelgaNo ratings yet
- Progressive Asymmetry in Occupational Noise-Induced Hearing Loss A Large Population-Based Cohort Study With A 15-Year Follow-Up PDFDocument6 pagesProgressive Asymmetry in Occupational Noise-Induced Hearing Loss A Large Population-Based Cohort Study With A 15-Year Follow-Up PDFKaty Marlen GongoraNo ratings yet
- Clinical Manifestations of Aural Fullness: Original ArticleDocument7 pagesClinical Manifestations of Aural Fullness: Original ArticleoctaviosnNo ratings yet
- 585 600 HellemanDocument17 pages585 600 HellemanBudi Darmawan DiswanNo ratings yet
- Characteristics of The Wideband Absorbance of Aco - 2021 - International JournalDocument7 pagesCharacteristics of The Wideband Absorbance of Aco - 2021 - International JournalHung Son TaNo ratings yet
- Tuberculous Otomastoiditis: Analysis of Otological TB With Intact Tympanic MembraneDocument8 pagesTuberculous Otomastoiditis: Analysis of Otological TB With Intact Tympanic MembraneNandini GuptaNo ratings yet
- Stapedotomy With Incus Vibroplasty - A Novel Surgical Solution of Advanced Otosclerosis and Its Place Among Existing Therapeutic Modalities - Hungarian Single Institutional ExperiencesDocument10 pagesStapedotomy With Incus Vibroplasty - A Novel Surgical Solution of Advanced Otosclerosis and Its Place Among Existing Therapeutic Modalities - Hungarian Single Institutional ExperiencesLuis De jesus SolanoNo ratings yet
- Otitis Media With EffusionDocument8 pagesOtitis Media With Effusiondr.ARISKI VLOGNo ratings yet
- Round and Oval Window Reinforcement For The Treatment of HyperacusisDocument5 pagesRound and Oval Window Reinforcement For The Treatment of HyperacusistonzmanojNo ratings yet
- O To SclerosisDocument9 pagesO To SclerosisHelgaNo ratings yet
- d098 PDFDocument7 pagesd098 PDFMayiz Renata LimerseNo ratings yet
- Otitis Media With E UsionDocument10 pagesOtitis Media With E UsionMas KaryonNo ratings yet
- Long-Term Outcomes of Acute Low-Tone Hearing LossDocument5 pagesLong-Term Outcomes of Acute Low-Tone Hearing LossFriska GriffinNo ratings yet
- 4.pre and Post Operative Evaluation of Hearing in Chronic Suppurative Otitis MediaDocument6 pages4.pre and Post Operative Evaluation of Hearing in Chronic Suppurative Otitis MediaharryNo ratings yet
- PEATE Doença de MeniereDocument8 pagesPEATE Doença de MeniereLuanna CarlosNo ratings yet
- Kwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesDocument25 pagesKwame Nkrumah University of Science and Technology: College of Health Sciences School of Medical SciencesEmmanuel DanquahNo ratings yet
- 409-Article Text-1439-1-10-20211018Document12 pages409-Article Text-1439-1-10-20211018Anonymous a2nxIq5No ratings yet
- Association of Hearing Impairment With Incident Depressive Symptoms: A Community-Based Prospective StudyDocument8 pagesAssociation of Hearing Impairment With Incident Depressive Symptoms: A Community-Based Prospective StudyQuentin LISANNo ratings yet
- Seminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M LuxonDocument9 pagesSeminar: Benjamin E Schreiber, Charlotte Agrup, Dorian O Haskard, Linda M Luxonmaria_garaveNo ratings yet
- Effect of Tinnitus in Distortion Products Otoacoustic Emissions (Dpoaes) in Normal Hearing PatientsDocument6 pagesEffect of Tinnitus in Distortion Products Otoacoustic Emissions (Dpoaes) in Normal Hearing Patientsvictoria barrientoNo ratings yet
- 10 Therole 20050598Document4 pages10 Therole 20050598DalRiveraPardoNo ratings yet
- Batson2017 OtosclerosisDocument6 pagesBatson2017 OtosclerosisnuhajazminNo ratings yet
- Day-Case Stapes Surgery: Day-Case Versus Inpatient Stapes Surgery For Otosclerosis: A Randomized Controlled TrialDocument7 pagesDay-Case Stapes Surgery: Day-Case Versus Inpatient Stapes Surgery For Otosclerosis: A Randomized Controlled TrialNurul Khairiyah AmriNo ratings yet
- CURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eDocument3 pagesCURRENT Diagnosis & Treatment in Otolaryngology-Head & Neck Surgery, 3eStephanie Vania EmbangNo ratings yet
- Jurnal Atresia KoanaDocument6 pagesJurnal Atresia KoanaArv IraNo ratings yet
- Art 16Document9 pagesArt 16sandra patricia monterrey gomezNo ratings yet
- Bone Conduction Thresholds in Patients With Otosclerosis: Eero Vartiainen, MD, and Seppo Karjalainen, MDDocument3 pagesBone Conduction Thresholds in Patients With Otosclerosis: Eero Vartiainen, MD, and Seppo Karjalainen, MDKeyko LampitaNo ratings yet
- Artikel & Jurnal THTDocument7 pagesArtikel & Jurnal THTRheza AldianoNo ratings yet
- 10 1016@j Ijporl 2019 06 019Document7 pages10 1016@j Ijporl 2019 06 019Eva PerdanaNo ratings yet
- 10 Bilateral Schwartze Sign, Decision-Making For Surgery. Iranian Journal of OtorhinolaryngologyDocument1 page10 Bilateral Schwartze Sign, Decision-Making For Surgery. Iranian Journal of OtorhinolaryngologyNurulSyaidahNo ratings yet
- Cochlear and Vestibular Functional Study in Patients With Sudden Deafness and Lyme DiseaseDocument5 pagesCochlear and Vestibular Functional Study in Patients With Sudden Deafness and Lyme DiseaseAura RachmawatiNo ratings yet
- Case Report OMEDocument8 pagesCase Report OMEYosephine ninaNo ratings yet
- Tinnitus and Hearing Survey Cultural Adaptati 2021 Brazilian Journal of OtoDocument7 pagesTinnitus and Hearing Survey Cultural Adaptati 2021 Brazilian Journal of OtoNavin SNNo ratings yet
- Otitis Media With Effusion Caused by A Parapharyngeal Tumor Showing Normal Nasopharyngeal FindingsDocument3 pagesOtitis Media With Effusion Caused by A Parapharyngeal Tumor Showing Normal Nasopharyngeal FindingsHazizul TohaNo ratings yet
- ETM-1478 - Functional Results MastoidectomyDocument13 pagesETM-1478 - Functional Results MastoidectomyHoria MocanuNo ratings yet
- Kung 2007Document10 pagesKung 2007Sarah fadlainiNo ratings yet
- Orthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsFrom EverandOrthodontics in Obstructive Sleep Apnea Patients: A Guide to Diagnosis, Treatment Planning, and InterventionsSu-Jung KimNo ratings yet
- Tourist LoyaltyDocument19 pagesTourist LoyaltyAditya HendraNo ratings yet
- EP150Document1 pageEP150Aditya HendraNo ratings yet
- TURANZA T005A Product Brochure Bridgestone Tyre SingaporeDocument1 pageTURANZA T005A Product Brochure Bridgestone Tyre SingaporeAditya HendraNo ratings yet
- Millennial 'S Engagement With Fashion BrandsDocument15 pagesMillennial 'S Engagement With Fashion BrandsAditya HendraNo ratings yet
- A Cross Sectional Study On The Bacteriologic Pattern of Chronic Otitis Media and Its Antibiotic SensitivityDocument5 pagesA Cross Sectional Study On The Bacteriologic Pattern of Chronic Otitis Media and Its Antibiotic SensitivityAditya HendraNo ratings yet
- Shopping MotivesDocument20 pagesShopping MotivesAditya HendraNo ratings yet
- Chiappini 2020Document7 pagesChiappini 2020Aditya HendraNo ratings yet
- Antecedents of Green Purchase Behaviour: An Examination of Altruism and Environmental KnowledgeDocument20 pagesAntecedents of Green Purchase Behaviour: An Examination of Altruism and Environmental KnowledgeAditya HendraNo ratings yet
- Retrospective Study of Fungal Elements by Potassium Hydroxide Mount in Chronic Otitis MediaDocument3 pagesRetrospective Study of Fungal Elements by Potassium Hydroxide Mount in Chronic Otitis MediaAditya HendraNo ratings yet
- Duygu 2020Document4 pagesDuygu 2020Aditya HendraNo ratings yet
- Journal Pre-Proof: American Journal of Otolaryngology - Head and Neck Medicine and SurgeryDocument11 pagesJournal Pre-Proof: American Journal of Otolaryngology - Head and Neck Medicine and SurgeryAditya HendraNo ratings yet
- Clinico-Epidemiological Profile of Chronic Otitis Media at A Tertiary Care HospitalDocument7 pagesClinico-Epidemiological Profile of Chronic Otitis Media at A Tertiary Care HospitalAditya HendraNo ratings yet
- Closure of Small Perforation in Tympanic Membrane by Use of Fat PlugDocument4 pagesClosure of Small Perforation in Tympanic Membrane by Use of Fat PlugAditya HendraNo ratings yet
- Tubercular Otitis Media: Demystifying Its Nuances and An Update On The Tenets of Emerging PerspectivesDocument9 pagesTubercular Otitis Media: Demystifying Its Nuances and An Update On The Tenets of Emerging PerspectivesAditya HendraNo ratings yet
- The Role of Intratympanic Dexamethasone in Sudden Sensorineural Hearing LossDocument5 pagesThe Role of Intratympanic Dexamethasone in Sudden Sensorineural Hearing LossAditya HendraNo ratings yet
- Otorhinolaryngology: Evaluation of The Vestibulo-Ocular Re Ex in Patients With Chronic Otitis MediaDocument8 pagesOtorhinolaryngology: Evaluation of The Vestibulo-Ocular Re Ex in Patients With Chronic Otitis MediaAditya HendraNo ratings yet
- Higher Education Under Fire: Implementing and Assessing A Culture Change For SustainmentDocument17 pagesHigher Education Under Fire: Implementing and Assessing A Culture Change For SustainmentAditya Hendra100% (1)
- Descriptive Study On Malignant Otitis Externa in Diabetic Patients at A Tertiary Care Hospital at MadurandhagamDocument5 pagesDescriptive Study On Malignant Otitis Externa in Diabetic Patients at A Tertiary Care Hospital at MadurandhagamAditya HendraNo ratings yet
- A First Time Lesson Study That Turned Into A Learning Study: Simone Klammer Barbara HanfstinglDocument15 pagesA First Time Lesson Study That Turned Into A Learning Study: Simone Klammer Barbara HanfstinglAditya HendraNo ratings yet
- Perceived Leadership Behaviours and Their Effects On IT Departments in Swiss Financial CompaniesDocument17 pagesPerceived Leadership Behaviours and Their Effects On IT Departments in Swiss Financial CompaniesAditya HendraNo ratings yet
- Cruise Brand Experience: Functional and Wellness Value Creation in Tourism BusinessDocument19 pagesCruise Brand Experience: Functional and Wellness Value Creation in Tourism BusinessAditya HendraNo ratings yet
- Online Company Blogs As Narrations of Plural Leadership: Arja Ropo, Elina I. Mäkinen and Inka SeppäDocument13 pagesOnline Company Blogs As Narrations of Plural Leadership: Arja Ropo, Elina I. Mäkinen and Inka SeppäAditya HendraNo ratings yet
- Shaping and Enhancing Airport Lounge Experiences: The Application of Brand Personality and Image Congruity TheoriesDocument20 pagesShaping and Enhancing Airport Lounge Experiences: The Application of Brand Personality and Image Congruity TheoriesAditya HendraNo ratings yet
- Scientific Management Scientific Management (Also Called Taylorism or The Taylor System) Is A Theory ofDocument2 pagesScientific Management Scientific Management (Also Called Taylorism or The Taylor System) Is A Theory ofDyan RetizaNo ratings yet
- ISO 22301 Lead Implementer - Two Page BrochureDocument2 pagesISO 22301 Lead Implementer - Two Page BrochurePECBCERTIFICATIONNo ratings yet
- Nature of Urban Interventions in Changing The OldDocument10 pagesNature of Urban Interventions in Changing The OldAneesha MuthurajNo ratings yet
- Griffin 1Document4 pagesGriffin 1Janine NogueraNo ratings yet
- Routing Security - MUM - MikroTik PDFDocument120 pagesRouting Security - MUM - MikroTik PDFAlex EnriquezNo ratings yet
- Strategic Intent Envisioning and MissionDocument23 pagesStrategic Intent Envisioning and Mission14122001riya2001No ratings yet
- National Open University of Nigeria: Wallet Payment StatusDocument4 pagesNational Open University of Nigeria: Wallet Payment Statusokoro collinsNo ratings yet
- Variations of Food Consumption Patterns in DCs and LDCsDocument3 pagesVariations of Food Consumption Patterns in DCs and LDCsCathPang-Mak100% (1)
- Experiment 1 Safety Measures: Use and Preparation of Chemical Substance 1.1 ObjectivesDocument8 pagesExperiment 1 Safety Measures: Use and Preparation of Chemical Substance 1.1 ObjectivesMaldini JosnonNo ratings yet
- RPD QuestionsDocument77 pagesRPD QuestionsDontoNo ratings yet
- DRUG STUDY CefuroximeDocument2 pagesDRUG STUDY CefuroximeParado Cabañal Skyliegh50% (2)
- 1COR22 - New in Christ - Notes PDFDocument2 pages1COR22 - New in Christ - Notes PDFeliastemer6528No ratings yet
- Rebound HammerDocument6 pagesRebound HammerDira AzmanNo ratings yet
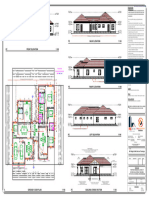
- MR Regis N MRS Dorcas Taruvinga - 050209Document1 pageMR Regis N MRS Dorcas Taruvinga - 050209pzarchitectural99No ratings yet
- All About Zookeeper and ClickHouse KeeperDocument45 pagesAll About Zookeeper and ClickHouse KeeperomyeudaihiepNo ratings yet
- Exoglove Research PaperDocument8 pagesExoglove Research Papersanket jainNo ratings yet
- Stability & Structre - SyllabusDocument7 pagesStability & Structre - SyllabusShanilNo ratings yet
- Water Quality For Supercritical Units Steag FormatDocument40 pagesWater Quality For Supercritical Units Steag FormatAmit MukherjeeNo ratings yet
- Major Fractures of The Pilon The Talus and The Calcaneus Current Concepts of TreatmentDocument241 pagesMajor Fractures of The Pilon The Talus and The Calcaneus Current Concepts of TreatmentPaul Radulescu - FizioterapeutNo ratings yet
- Employment Tribunals: Claimant RespondentDocument42 pagesEmployment Tribunals: Claimant RespondentMichael SmithNo ratings yet
- QuestionDocument4 pagesQuestionKira NguyễnNo ratings yet
- Huff ManDocument4 pagesHuff Mangopal_svsemails8998No ratings yet
- Worksheet 9 (Autosomes & Sex Chromosome)Document2 pagesWorksheet 9 (Autosomes & Sex Chromosome)HalaNo ratings yet
- 6 MD 85Document1,256 pages6 MD 85Yahya DarNo ratings yet
- Teachers Manual in Filipino 10 PDFDocument2 pagesTeachers Manual in Filipino 10 PDFIan Dagame0% (1)
- Surah Al Asr (Explanation)Document4 pagesSurah Al Asr (Explanation)Adil KhatriNo ratings yet