Download as pdf or txt
You might also like
- Toronto Police Report On "Systemic Racism" in Officer Use of Force and Strip SearchesDocument119 pagesToronto Police Report On "Systemic Racism" in Officer Use of Force and Strip SearchesToronto Star100% (2)
- 2024-01-29 Municipal Permitting - Flushing Out The Nonsense enDocument37 pages2024-01-29 Municipal Permitting - Flushing Out The Nonsense enToronto StarNo ratings yet
- Application of The Convention On The Prevention and Punishment of The Crime of Genocide in The Gaza StripDocument29 pagesApplication of The Convention On The Prevention and Punishment of The Crime of Genocide in The Gaza StripToronto StarNo ratings yet
- Our Campus, Our SafetyDocument44 pagesOur Campus, Our SafetyToronto Star100% (2)
- Coronation Order of ServiceDocument50 pagesCoronation Order of ServiceCTV News100% (5)
- Letter To Minister Downey Re Bingo Halls and OLGDocument3 pagesLetter To Minister Downey Re Bingo Halls and OLGToronto StarNo ratings yet
- Project 5 PDFDocument3 pagesProject 5 PDFapi-509845050No ratings yet
- Assets Liabilities & Net Worth: Check 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 28,127Document7 pagesAssets Liabilities & Net Worth: Check 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 0 28,127Sofía MargaritaNo ratings yet
- PHAC Modelling - 20210903ENDocument17 pagesPHAC Modelling - 20210903ENCPAC TVNo ratings yet
- Update On COVID-19 in Canada, March 26, 2021Document20 pagesUpdate On COVID-19 in Canada, March 26, 2021Andy RigaNo ratings yet
- Federal COVID-19 Modelling: March 26, 2021Document20 pagesFederal COVID-19 Modelling: March 26, 2021CPAC TVNo ratings yet
- Update On COVID-19 in Canada - Epidemiology and Preparedness April 1, 2022Document10 pagesUpdate On COVID-19 in Canada - Epidemiology and Preparedness April 1, 2022Andy RigaNo ratings yet
- Sour Crude Diet: Venezuela Production Decline Shifts Lighter Crude Slates For Heavy RefinersDocument21 pagesSour Crude Diet: Venezuela Production Decline Shifts Lighter Crude Slates For Heavy RefinersLindsey BondNo ratings yet
- Adaptive Resilience To The Pandemic at The National LevelDocument5 pagesAdaptive Resilience To The Pandemic at The National LevelCrimson MetalNo ratings yet
- Bos Covid-19 Updates 1.26.2021Document28 pagesBos Covid-19 Updates 1.26.2021Jennifer ChurchillNo ratings yet
- 11 January 2021: RT PCR Lab: 114 Genexpert Lab: 27 Rapid Antigen: 40Document8 pages11 January 2021: RT PCR Lab: 114 Genexpert Lab: 27 Rapid Antigen: 40Abir HabibNo ratings yet
- PRMG 30-Project Budgeting and Financial Control Assignment (6) Cash Flow AnalysisDocument4 pagesPRMG 30-Project Budgeting and Financial Control Assignment (6) Cash Flow AnalysisamerNo ratings yet
- Example KPI With GraphsDocument4 pagesExample KPI With GraphsSathesh AustinNo ratings yet
- NR - CRT Facturi Comb. Ig., Cosm. Hrana Telefon Intret. Lumina GAZ Net, CabluDocument2 pagesNR - CRT Facturi Comb. Ig., Cosm. Hrana Telefon Intret. Lumina GAZ Net, CablugelubotNo ratings yet
- Product Sales: Customer Type 2021 AvgDocument5 pagesProduct Sales: Customer Type 2021 AvgkamalNo ratings yet
- COVID School and Age Related Data Update.2021.03.18Document4 pagesCOVID School and Age Related Data Update.2021.03.18Jackie SmithNo ratings yet
- Construction Industry AnalysisDocument132 pagesConstruction Industry AnalysisEleanorXuNo ratings yet
- Serba Farm Organic PlantationDocument23 pagesSerba Farm Organic PlantationET Hadi SaputraNo ratings yet
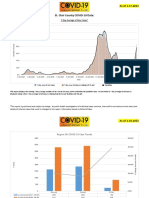
- Dekalb Covid-19 Epidemiology Report: Daily and Cumulative Covid-19 Case Counts, Dekalb CountyDocument13 pagesDekalb Covid-19 Epidemiology Report: Daily and Cumulative Covid-19 Case Counts, Dekalb CountyZachary HansenNo ratings yet
- ACC 221 Assignment (2024)Document9 pagesACC 221 Assignment (2024)Rahman OmaryNo ratings yet
- CS ForecastingDocument4 pagesCS ForecastingDe Gala ShailynNo ratings yet
- Hammed IITA Conference May1023Document7 pagesHammed IITA Conference May1023yinkaNo ratings yet
- 2023 2Q Earnings ReleaseDocument15 pages2023 2Q Earnings ReleaseProtik MazumdarNo ratings yet
- Liab SolutionDocument8 pagesLiab SolutionAngelshine LacanlaleNo ratings yet
- 05NTD 2022 - UPDATES IN VECTOR CONTROL IN MALAYSIA: What Is New?Document61 pages05NTD 2022 - UPDATES IN VECTOR CONTROL IN MALAYSIA: What Is New?Institute for Clinical ResearchNo ratings yet
- External Situation Report 86 - 19 January 2022Document26 pagesExternal Situation Report 86 - 19 January 2022IndahNo ratings yet
- OCBC NISP Market Outlook 2021 - Steven Yudha - AshmoreDocument16 pagesOCBC NISP Market Outlook 2021 - Steven Yudha - AshmoreNurul Meutia SalsabilaNo ratings yet
- Update On COVID-19 in Canada: Epidemiology and ModellingDocument22 pagesUpdate On COVID-19 in Canada: Epidemiology and ModellingCPAC TVNo ratings yet
- Update On COVID-19 in Canada: Epidemiology and ModellingDocument22 pagesUpdate On COVID-19 in Canada: Epidemiology and ModellingAndy RigaNo ratings yet
- Tipos de Inventarios: Descripcion Mts 2 Valor MetroDocument3 pagesTipos de Inventarios: Descripcion Mts 2 Valor Metrocarlos perezNo ratings yet
- Chapter2charts For StudentsDocument68 pagesChapter2charts For StudentsRomar PogoyNo ratings yet
- Tahsil Profile: Census of India 2011Document6 pagesTahsil Profile: Census of India 2011Megha SawantNo ratings yet
- Activity Sheet - Bank FormsDocument3 pagesActivity Sheet - Bank FormsJane Dela cruzNo ratings yet
- Dashboard PenjualanDocument690 pagesDashboard PenjualanXen DedNo ratings yet
- ARcover Brochure Final1Document2 pagesARcover Brochure Final1Esther LeeNo ratings yet
- COVID19 Impact Analysis 5.11Document23 pagesCOVID19 Impact Analysis 5.11Arun KumarNo ratings yet
- Investing in The Time of Covid 19 PDFDocument31 pagesInvesting in The Time of Covid 19 PDFROHIT RANENo ratings yet
- BookDocument1 pageBookZahidNo ratings yet
- Af 160145Document4 pagesAf 160145nurinNo ratings yet
- BACS Weekly Monetary Report 25-07-18Document7 pagesBACS Weekly Monetary Report 25-07-18Gian MarcosNo ratings yet
- Bubble ChartDocument2 pagesBubble ChartRalph Brandon BulusanNo ratings yet
- Chicago COVID-19 Update V3 4.14.2020Document2 pagesChicago COVID-19 Update V3 4.14.2020Shannon Margaret BlumNo ratings yet
- Practice FileDocument22 pagesPractice Fileএ.বি.এস. আশিকNo ratings yet
- Monthly Report: July AA & Nylon 66 Chip Market ReportDocument5 pagesMonthly Report: July AA & Nylon 66 Chip Market ReportNISHSHANKANo ratings yet
- Inr Cr. Q Revenue Contribution To PE Contribution To Group Fixed Cost TVCDocument12 pagesInr Cr. Q Revenue Contribution To PE Contribution To Group Fixed Cost TVCSaagar ChitkaraNo ratings yet
- Journal Entries and Adjustments - Bea Manufacturing Co.Document2 pagesJournal Entries and Adjustments - Bea Manufacturing Co.NikolaiNo ratings yet
- M0Del Answers T0 Cpa 2 Examinati0N Set 0N 3 December 1996Document3 pagesM0Del Answers T0 Cpa 2 Examinati0N Set 0N 3 December 1996gakumoNo ratings yet
- Contoh Family BudgetDocument3 pagesContoh Family BudgetReno VehardianNo ratings yet
- BreakevenDocument15 pagesBreakevenanjitaNo ratings yet
- Business Plan: Proponent: Center Capital: Proposed ProjectDocument3 pagesBusiness Plan: Proponent: Center Capital: Proposed ProjectBorly GonzagaNo ratings yet
- Case Study Road To Management TraineeDocument7 pagesCase Study Road To Management Traineethanh nguyen trongNo ratings yet
- Flash Integrado - Mining Operations 2021 - EPDocument19 pagesFlash Integrado - Mining Operations 2021 - EPJulio Cesar CcenteNo ratings yet
- Qu Hưu Trí Na Uy - Gpfg-Half-Year-Report - 2022Document41 pagesQu Hưu Trí Na Uy - Gpfg-Half-Year-Report - 2022huynhtruonglyNo ratings yet
- Budget Plan Safewood FixDocument1 pageBudget Plan Safewood FixCynthia Dhyaa NNo ratings yet
- 01 Steop enDocument28 pages01 Steop enMutesa ChrisNo ratings yet
- National Review of The Feed Sector in Vietnam: Xavier BocquilletDocument18 pagesNational Review of The Feed Sector in Vietnam: Xavier BocquilletTuấn Thế NguyễnNo ratings yet
- Oppenheimer Holdings Inc. Annual Report 2010Document52 pagesOppenheimer Holdings Inc. Annual Report 2010lulupupututuNo ratings yet
- Oct3 NSM Keynote2 - LGB - PSADocument22 pagesOct3 NSM Keynote2 - LGB - PSALGU San FranciscoNo ratings yet
- Finance ReportDocument4 pagesFinance ReportVo Pham Que Chi (K16HCM)No ratings yet
- Combo ChartDocument6 pagesCombo ChartjoangopanNo ratings yet
- Succession Bingo Board SMDocument1 pageSuccession Bingo Board SMToronto StarNo ratings yet
- Michele Landsberg Introduces Marian XDocument1 pageMichele Landsberg Introduces Marian XToronto StarNo ratings yet
- ETFO AgreementDocument2 pagesETFO AgreementToronto StarNo ratings yet
- Ruling On Access To Trump ArraignmentDocument6 pagesRuling On Access To Trump ArraignmentToronto StarNo ratings yet
- Metrolinx - Metrolinx Statement On Eglinton Crosstown LRTDocument1 pageMetrolinx - Metrolinx Statement On Eglinton Crosstown LRTToronto StarNo ratings yet
- Ruling On Access To Trump ArraignmentDocument6 pagesRuling On Access To Trump ArraignmentToronto StarNo ratings yet
- Nick Nurse Relieved of Head Coaching DutiesDocument1 pageNick Nurse Relieved of Head Coaching DutiesToronto StarNo ratings yet
- Pollara EconoOutlook2023Document18 pagesPollara EconoOutlook2023Toronto StarNo ratings yet
- Play Dressup With Our Royal Paper DollsDocument2 pagesPlay Dressup With Our Royal Paper DollsToronto StarNo ratings yet
- Bulletin Licence PlateDocument1 pageBulletin Licence PlateToronto StarNo ratings yet
- Canadian Forces Administrative Order (CFAO 19-20)Document3 pagesCanadian Forces Administrative Order (CFAO 19-20)Toronto StarNo ratings yet
- Dominic Cardy's Resignation LetterDocument2 pagesDominic Cardy's Resignation LetterToronto StarNo ratings yet
- Letter Bill 39Document1 pageLetter Bill 39Toronto StarNo ratings yet
- Overview Report: Fundraising in Support of ProtestorsDocument61 pagesOverview Report: Fundraising in Support of ProtestorsToronto StarNo ratings yet
- COVID-19 PANDEMIC - Specific COVID-19 Benefits - AG ReportDocument92 pagesCOVID-19 PANDEMIC - Specific COVID-19 Benefits - AG ReportToronto StarNo ratings yet
- 2022 Dora Award WinnersDocument7 pages2022 Dora Award WinnersToronto Star100% (2)
- Ontario Deaths in Custody On The Rise 2022Document16 pagesOntario Deaths in Custody On The Rise 2022Toronto StarNo ratings yet
- Sept. 7 Toronto StarDocument1 pageSept. 7 Toronto StarToronto StarNo ratings yet
- Exhibit # 5 - Doc - Victim Impact Statement From S. MACKAYDocument1 pageExhibit # 5 - Doc - Victim Impact Statement From S. MACKAYToronto StarNo ratings yet
- Search Warrant MALDocument7 pagesSearch Warrant MALpelofskyj100% (1)
- Toronto StarDocument1 pageToronto StarToronto StarNo ratings yet
- Exhibit # 4 - Doc - Victim Impact Statement From T.kuuzUZDocument2 pagesExhibit # 4 - Doc - Victim Impact Statement From T.kuuzUZToronto StarNo ratings yet
- Affidavit For The FBI Search of President Donald Trump's HomeDocument55 pagesAffidavit For The FBI Search of President Donald Trump's HomeTrisha Powell CrainNo ratings yet
- Exhibit # 9 - Doc-Victim Impact Statement From M. JUSTINODocument2 pagesExhibit # 9 - Doc-Victim Impact Statement From M. JUSTINOToronto StarNo ratings yet
- Fatty Liver InformationDocument2 pagesFatty Liver Informationohayo3590No ratings yet
- JAAOS - Volume 11 - Issue 01 January & February 2003Document77 pagesJAAOS - Volume 11 - Issue 01 January & February 2003kenthepaNo ratings yet
- Arterial Blood Gas Analysis Profile in Extremely Premature Neonates Admitted in A Tertiary Care Neonatal Intensive Care UnitDocument6 pagesArterial Blood Gas Analysis Profile in Extremely Premature Neonates Admitted in A Tertiary Care Neonatal Intensive Care UnitIJAR JOURNALNo ratings yet
- Better Combat DescriptionsDocument1 pageBetter Combat DescriptionsDamon FagenNo ratings yet
- ENT BCQsDocument19 pagesENT BCQsSajid AliNo ratings yet
- Complete Blood Picture (CBP), EDTA Whole Blood: Master - SushanthDocument4 pagesComplete Blood Picture (CBP), EDTA Whole Blood: Master - SushanthAbdul MuqeemNo ratings yet
- Electrode Placement: Midclavicular LineDocument4 pagesElectrode Placement: Midclavicular LineJeneleth DayaodaoNo ratings yet
- Specialty Doctor/Senior Clinical Fellow in NEONATOLOGY (Middle Grade, ST4 To 8 Equivalent)Document10 pagesSpecialty Doctor/Senior Clinical Fellow in NEONATOLOGY (Middle Grade, ST4 To 8 Equivalent)madimadi11No ratings yet
- Laporan Pemakaian Dan Lembar Permintaan Obat (Lplpo)Document12 pagesLaporan Pemakaian Dan Lembar Permintaan Obat (Lplpo)SeptiyaniNo ratings yet
- CreatinineDocument3 pagesCreatinineElixirNo ratings yet
- Concept Map of DMDocument1 pageConcept Map of DMRobert Timothy YapNo ratings yet
- Bruxism and Its TreatmentDocument22 pagesBruxism and Its TreatmentShahid ShaikhNo ratings yet
- Yes, Now You Can Correct Your Presbyopia ("Chaalees") With Custom LasikDocument2 pagesYes, Now You Can Correct Your Presbyopia ("Chaalees") With Custom LasikChandana KarthikNo ratings yet
- Bab 3Document32 pagesBab 3Ciptaningrum Marisa PNo ratings yet
- Diabetes Mellitus NCPDocument5 pagesDiabetes Mellitus NCPCazze SunioNo ratings yet
- Addison's Disease (Primary Adrenal Insufficiency)Document5 pagesAddison's Disease (Primary Adrenal Insufficiency)sunnnydayNo ratings yet
- MOH Laboratory Requisition PDFDocument1 pageMOH Laboratory Requisition PDFeadmitNo ratings yet
- Chapter 6 NeuroemergencyDocument21 pagesChapter 6 NeuroemergencyEdo FebrianNo ratings yet
- Single Tooth Implant Placement in Anterior Maxilla PDFDocument5 pagesSingle Tooth Implant Placement in Anterior Maxilla PDFankitaNo ratings yet
- ELSO Guidelines For ECMO CentersDocument7 pagesELSO Guidelines For ECMO CentersFernando AlvesNo ratings yet
- SLE PathophysiologyDocument3 pagesSLE PathophysiologyyasiraNo ratings yet
- Renal CalculusDocument34 pagesRenal CalculusChandrashekar N.k.No ratings yet
- Da Lieu - Bac Si - Ao Hai YenDocument5 pagesDa Lieu - Bac Si - Ao Hai YenBinh LeNo ratings yet
- Ophtha SGD 1Document4 pagesOphtha SGD 1Richelle IgnacioNo ratings yet
- Cyclical Training - Guide and CalendarDocument3 pagesCyclical Training - Guide and CalendarLau PerezNo ratings yet
- GCT Giant Cell Tumor PresentationDocument22 pagesGCT Giant Cell Tumor PresentationHasyasya Furnita KosaziNo ratings yet
- Lab - 9-Antimicrobial Agent: Assist. Lec. Wasan HatemDocument14 pagesLab - 9-Antimicrobial Agent: Assist. Lec. Wasan HatemMustafa A. DawoodNo ratings yet
- Rheumatoid 4Document14 pagesRheumatoid 4Mohamed AbozeidNo ratings yet
- AnticonvulsantDocument37 pagesAnticonvulsantPamela MendozaNo ratings yet