Download as pdf or txt
You might also like
- DBTDocument210 pagesDBTKatheryn P100% (34)
- CSP 515 - Mangaging Stress Anxiety Asca Lesson Plan TemplateDocument5 pagesCSP 515 - Mangaging Stress Anxiety Asca Lesson Plan Templateapi-548398232No ratings yet
- CSP 621 - Mindsets and Behaviors Action Plan 1Document3 pagesCSP 621 - Mindsets and Behaviors Action Plan 1api-548398232No ratings yet
- Case ConceptualizationDocument4 pagesCase ConceptualizationShannon Johnson80% (5)
- Suicidal Ideation Coping ResponsesDocument32 pagesSuicidal Ideation Coping ResponsesKath BuñoNo ratings yet
- Research-Paper About SuicideDocument10 pagesResearch-Paper About SuicideAndrei DaduralNo ratings yet
- FACTSHEET YouthSuicideRevisedSpring2010Document10 pagesFACTSHEET YouthSuicideRevisedSpring2010Riyan SudrajadNo ratings yet
- Effect of Suicide Among Adolescent - ResearchDocument5 pagesEffect of Suicide Among Adolescent - Researchdanielcaampued7No ratings yet
- Suicide Contagion, Gender, and Suicide AttemptsDocument8 pagesSuicide Contagion, Gender, and Suicide AttemptsJulian David Carvajal GuevaraNo ratings yet
- EditedDocument13 pagesEditedKeii blackhoodNo ratings yet
- Norman FinalDocument8 pagesNorman FinalDee Dong-Hyun KimNo ratings yet
- Artikel LGBT 2020Document18 pagesArtikel LGBT 20200120 Annafia HanifNo ratings yet
- Professional Issues in School Counseling and Suicide PreventionDocument27 pagesProfessional Issues in School Counseling and Suicide PreventionNurul Fatehah Binti KamaruzaliNo ratings yet
- Psychology and Suicidal ThoughtsDocument10 pagesPsychology and Suicidal ThoughtsMark MansonNo ratings yet
- A Multivariate Analysis of Suicide Ideation Among University Students in The PhilippinesDocument17 pagesA Multivariate Analysis of Suicide Ideation Among University Students in The Philippinesako si XianNo ratings yet
- Edited 61 PagesDocument63 pagesEdited 61 PagesRichard BonghanoyNo ratings yet
- Savitha. S 1 and Dr. Sreemathi.N.LDocument10 pagesSavitha. S 1 and Dr. Sreemathi.N.LAnonymous CwJeBCAXpNo ratings yet
- Chapter IiDocument3 pagesChapter IiTupas Alpiche Lyka SheherezadeNo ratings yet
- Related StudiesDocument5 pagesRelated StudiesRicojay FernandezNo ratings yet
- Thinking and Doing Prevention: A Critical Analysis of Contemporary Youth Crime and Suicide Prevention DiscoursesDocument10 pagesThinking and Doing Prevention: A Critical Analysis of Contemporary Youth Crime and Suicide Prevention DiscoursesSandeep SuvarnaNo ratings yet
- Background Scope of The Problem Risk Factors Case Studies of Youth Suicide Conclusions and Recommendations ReferencesDocument13 pagesBackground Scope of The Problem Risk Factors Case Studies of Youth Suicide Conclusions and Recommendations ReferencesbntmaniNo ratings yet
- Final Na Ni HaDocument56 pagesFinal Na Ni HaRichard BonghanoyNo ratings yet
- Psychological Consequences of Sexual TraumaDocument11 pagesPsychological Consequences of Sexual Traumamary engNo ratings yet
- Code No. Red. StyDocument64 pagesCode No. Red. StyRichard BonghanoyNo ratings yet
- 1 s2.0 S2666354620300892 MainDocument11 pages1 s2.0 S2666354620300892 MainMaría Camila Trujillo LópezNo ratings yet
- Term ProjectDocument28 pagesTerm ProjectNishit PatelNo ratings yet
- 22 5 Casey PaperDocument15 pages22 5 Casey PaperAmulya AnandNo ratings yet
- Bullying and Suicide in High School Students: Findings From The 2015 California Youth Risk Behavior SurveyDocument16 pagesBullying and Suicide in High School Students: Findings From The 2015 California Youth Risk Behavior SurveyHifzhi PadliannorNo ratings yet
- Suicidal Behaviour Among SchooDocument16 pagesSuicidal Behaviour Among Schoogs67461No ratings yet
- Essay: Causes of The Uproar of Mass ShootingsDocument5 pagesEssay: Causes of The Uproar of Mass ShootingsPaper24No ratings yet
- Almars Edited Chapter 1 To 3 For ResearchDocument73 pagesAlmars Edited Chapter 1 To 3 For ResearchRichard BonghanoyNo ratings yet
- Suicidal Behaviors and DepresionDocument12 pagesSuicidal Behaviors and DepresionAndrea GómezNo ratings yet
- A Longitudinal Study of Racial Discrimination and Risk For Death Ideation in African American YouthDocument17 pagesA Longitudinal Study of Racial Discrimination and Risk For Death Ideation in African American YouthAnis SumarniNo ratings yet
- Childhood Trauma and Current Psychological Functioning in Adults With Social Anxiety DisorderDocument7 pagesChildhood Trauma and Current Psychological Functioning in Adults With Social Anxiety DisorderAnda SlicNo ratings yet
- Adolescent Suicide Myths in The United StatesDocument14 pagesAdolescent Suicide Myths in The United Statesarhodes777No ratings yet
- Alix Etal (2019) JCSADocument17 pagesAlix Etal (2019) JCSAzvl hafizNo ratings yet
- Age Disparity Between GendersDocument22 pagesAge Disparity Between Gendersapi-659623153No ratings yet
- Levels of Dissociation and Nonsuicidal Self Injury A Quartile Risk ModelDocument20 pagesLevels of Dissociation and Nonsuicidal Self Injury A Quartile Risk ModelFlavia AraujoNo ratings yet
- FC Project 125Document13 pagesFC Project 125Kiran MauryaNo ratings yet
- The Role of Culture in Suicide Prevention in AdolescentsDocument6 pagesThe Role of Culture in Suicide Prevention in Adolescentskrivavi12No ratings yet
- Real Na This ThesisDocument69 pagesReal Na This ThesisJohnDominicMoralesNo ratings yet
- Sucidal BehaviourdocxDocument3 pagesSucidal BehaviourdocxDr. Anadi JangraNo ratings yet
- Prevention of Suicide and Suicidal Behaviour in AdolescentsDocument11 pagesPrevention of Suicide and Suicidal Behaviour in AdolescentsVijaya RaniNo ratings yet
- The Cultural Theory and Model of Suicide (2010)Document16 pagesThe Cultural Theory and Model of Suicide (2010)Aulia Kusuma Wardani 'elDhe'No ratings yet
- Running Head: Bullying and Adolescent PsychopathologyDocument8 pagesRunning Head: Bullying and Adolescent PsychopathologyColleen ClarkNo ratings yet
- Running Head: Mental Health in Higher Educaiton 1Document13 pagesRunning Head: Mental Health in Higher Educaiton 1api-449017192No ratings yet
- The Suicidal ClientDocument18 pagesThe Suicidal ClientReet_paed100% (2)
- Provide:: Suicide Fighting and Aggression Vehicular AccidentsDocument2 pagesProvide:: Suicide Fighting and Aggression Vehicular AccidentsMary SingletonNo ratings yet
- The Causation Behind Global Teenage Depression and Suicide 1Document20 pagesThe Causation Behind Global Teenage Depression and Suicide 1api-316737443No ratings yet
- The Relationship Between Depression and Aggressive Characteristics of Bullying in The JHS Department of STIPDocument9 pagesThe Relationship Between Depression and Aggressive Characteristics of Bullying in The JHS Department of STIPFelindBularonSaladaNo ratings yet
- Homework Suicide RatesDocument4 pagesHomework Suicide Ratesafetovibe100% (1)
- The Biopsychosocial ModelDocument13 pagesThe Biopsychosocial ModelelenichatziNo ratings yet
- Perception of Suicidal Attempts Among College Students in MalaysiaDocument12 pagesPerception of Suicidal Attempts Among College Students in MalaysiaJuvis EsguerraNo ratings yet
- DOMESTIC VIOLENCE EssayDocument1 pageDOMESTIC VIOLENCE EssayCarla ParraNo ratings yet
- Mass Shootings Today - PaperDocument12 pagesMass Shootings Today - Paperxavierstagg5No ratings yet
- Thesis Proposal GallanoDocument26 pagesThesis Proposal GallanogaboteteNo ratings yet
- Development of Self-Inflicted Injury Comorbidities and Continuities With Borderline and Antisocial Personality TraitsDocument18 pagesDevelopment of Self-Inflicted Injury Comorbidities and Continuities With Borderline and Antisocial Personality Traitsme13No ratings yet
- Duke University 304-2216-1-pb WxyzDocument11 pagesDuke University 304-2216-1-pb Wxyzapi-231034227No ratings yet
- Associations Among Bullying Cyberbullying and Suicide in Highschool Students-LibreDocument10 pagesAssociations Among Bullying Cyberbullying and Suicide in Highschool Students-LibreGusti Ngurah Andhika PNo ratings yet
- SuicideDocument6 pagesSuicideAnonymous S0MyRHNo ratings yet
- The Link Between Childhood Abuse, Delinquency and Long-Term ProblemsDocument10 pagesThe Link Between Childhood Abuse, Delinquency and Long-Term Problemsapi-483730069No ratings yet
- Parental Bonding and Vulnerabilitv Adolescent Suicide: Martin Waite2Document9 pagesParental Bonding and Vulnerabilitv Adolescent Suicide: Martin Waite2kirti singhNo ratings yet
- Suicide and Eating Disordered Behavior Among Individuals of African Descent:: Acculturation and PsychopathologyFrom EverandSuicide and Eating Disordered Behavior Among Individuals of African Descent:: Acculturation and PsychopathologyNo ratings yet
- Chs 2021-2022 Profile VDocument2 pagesChs 2021-2022 Profile Vapi-548398232No ratings yet
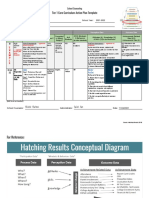
- CSP 617 - Interviewing Job Skills Hatching Results Tier 1 Action PlanDocument2 pagesCSP 617 - Interviewing Job Skills Hatching Results Tier 1 Action Planapi-548398232No ratings yet
- Walker Jhs 3rd Quarter Data Communication 21-22Document1 pageWalker Jhs 3rd Quarter Data Communication 21-22api-548398232No ratings yet
- CSP 515 - Mangaging Stress Anxiety Hatching Results Tier 1 Action PlanDocument2 pagesCSP 515 - Mangaging Stress Anxiety Hatching Results Tier 1 Action Planapi-548398232No ratings yet
- CSP 617 - Job Preparation Interviewing Job Skills 1Document35 pagesCSP 617 - Job Preparation Interviewing Job Skills 1api-548398232No ratings yet
- Walker - Social Skills PeersDocument18 pagesWalker - Social Skills Peersapi-548398232No ratings yet
- Walker - Study SkillsDocument15 pagesWalker - Study Skillsapi-548398232No ratings yet
- Mindfulness Group Lesson 6Document11 pagesMindfulness Group Lesson 6api-548398232No ratings yet
- Mental Health Toolkit Group 2Document33 pagesMental Health Toolkit Group 2api-548398232No ratings yet
- Final CSCP Ang Han Schubert 1 1Document35 pagesFinal CSCP Ang Han Schubert 1 1api-548398232No ratings yet
- Anxiety Disorders Lesson PlanDocument32 pagesAnxiety Disorders Lesson PlanPedrosa NardNo ratings yet
- Treating Comorbid PTSD and BPDDocument52 pagesTreating Comorbid PTSD and BPDdoppler_No ratings yet
- Texto 1Document9 pagesTexto 1Eve CincottaNo ratings yet
- Mode Deactivation Therapy For Aggression and Oppositional Behavior in Adolescents - An Integrative Methodology Using ACT, DBT, and CBTDocument206 pagesMode Deactivation Therapy For Aggression and Oppositional Behavior in Adolescents - An Integrative Methodology Using ACT, DBT, and CBTAlguém100% (1)
- Interpersonal Psychotherapy For Depressed Adolescents (IPT-A)Document8 pagesInterpersonal Psychotherapy For Depressed Adolescents (IPT-A)Wiwin Apsari WahyuniNo ratings yet
- MCQ Paper 2016 NZ PDFDocument53 pagesMCQ Paper 2016 NZ PDFAbdul Sadiq100% (1)
- Borderline Personality Disorder - Wikipedia The Free Encyclope PDFDocument34 pagesBorderline Personality Disorder - Wikipedia The Free Encyclope PDFstephNo ratings yet
- Psych 7A FinalDocument16 pagesPsych 7A FinalMatthew Kim100% (1)
- Thoma 2015Document39 pagesThoma 2015Izabella de LimaNo ratings yet
- Attachment DisorderDocument44 pagesAttachment DisorderFive ChNo ratings yet
- Self MonitoringDocument6 pagesSelf MonitoringHilal KhattakNo ratings yet
- Chapter 5 - Multiple ChoiceDocument15 pagesChapter 5 - Multiple ChoiceNicky PhakathiNo ratings yet
- Eating Disorders: by Dr. Min Min Phyo 20 August 2019Document74 pagesEating Disorders: by Dr. Min Min Phyo 20 August 2019thu thuNo ratings yet
- What To Know About ArachnophobiaDocument4 pagesWhat To Know About ArachnophobiaJuandi Cardenas100% (2)
- CBT NYC Newsletter Fall03Document6 pagesCBT NYC Newsletter Fall03Mike ChristopherNo ratings yet
- The Science and Practice of Case ConceptualizationDocument12 pagesThe Science and Practice of Case ConceptualizationFrancisco Erdozain100% (1)
- Addendum HCDocument271 pagesAddendum HCClara Franco RamirezNo ratings yet
- Evidence-Based Psychotherapy Interventions To Improve Psychosocial Functioning in Veterans With PTSDDocument10 pagesEvidence-Based Psychotherapy Interventions To Improve Psychosocial Functioning in Veterans With PTSDM SalNo ratings yet
- The Psychological Effects of LightDocument95 pagesThe Psychological Effects of LightSusie Olczak100% (1)
- Forensic Psychologyin PracticeDocument17 pagesForensic Psychologyin PracticeDeepika L.No ratings yet
- Bette ResumeDocument1 pageBette Resumeapi-707499894No ratings yet
- Suicidio PDFDocument9 pagesSuicidio PDFLUCIAMELENDEZSNo ratings yet
- Shame, Pride and Eating Disorders PDFDocument14 pagesShame, Pride and Eating Disorders PDFhodmezevasarhelj100% (1)
- Tokoh CBTDocument5 pagesTokoh CBTrara.01No ratings yet
- (APA Handbooks in Psychology) Gregory J. Madden - APA Handbook of Behavior Analysis. 2-American Psychological Association (2016)Document472 pages(APA Handbooks in Psychology) Gregory J. Madden - APA Handbook of Behavior Analysis. 2-American Psychological Association (2016)Cristian Yesid Urbano MejiaNo ratings yet
- Beyond Acceptance and Commitment Therapy, Process-Based Therapy - Ong, Levin & Twohig (Paper)Document12 pagesBeyond Acceptance and Commitment Therapy, Process-Based Therapy - Ong, Levin & Twohig (Paper)Sergio Liera AguilarNo ratings yet
- Personal Philosophy of Integration and Case ExampleDocument14 pagesPersonal Philosophy of Integration and Case ExampleGosia GratefulNo ratings yet
- Letting Go of Your Ex: CBT Skills To Heal The Pain of A Breakup and Overcome Love Addiction 1st Edition Cortney Soderlind WarrenDocument70 pagesLetting Go of Your Ex: CBT Skills To Heal The Pain of A Breakup and Overcome Love Addiction 1st Edition Cortney Soderlind Warrenfingeajalah100% (8)