
Liver Pathophysiology
Liver Pathophysiology
You might also like
- Usmle Free 150Document44 pagesUsmle Free 150ironslave100% (1)
- 15casebook in Gastroenterology PDFDocument109 pages15casebook in Gastroenterology PDFKMNo ratings yet
- Obesity Term PaperDocument20 pagesObesity Term PaperBave EnriquezNo ratings yet
- Biochemistry: For The Students of Pharmacy Technicians (Category-B)Document74 pagesBiochemistry: For The Students of Pharmacy Technicians (Category-B)Rajesh Kumar0% (1)
- Alanine Aminotransferase (Alt-Gpt)Document1 pageAlanine Aminotransferase (Alt-Gpt)Risqon Anjahiranda Adiputra50% (2)
- Metabolites: Physiological Responses of Post-Dietary Effects: Lessons From Pre-Clinical and Clinical StudiesDocument16 pagesMetabolites: Physiological Responses of Post-Dietary Effects: Lessons From Pre-Clinical and Clinical StudiesSarah OctaviaNo ratings yet
- Volume 13, Issue 2, August 2012 - Helicobacter Pylori Infection in Superficial Gastritis, Erosive Gastritis and Gastric UlcerDocument6 pagesVolume 13, Issue 2, August 2012 - Helicobacter Pylori Infection in Superficial Gastritis, Erosive Gastritis and Gastric UlcerAndy SelvianNo ratings yet
- Hrkansh NotesDocument424 pagesHrkansh NotesAhmed RagabNo ratings yet
- AP-Food List TPCM PDFDocument12 pagesAP-Food List TPCM PDFS K ChughNo ratings yet
- BiochemDocument10 pagesBiochemWaseem Abbas ShaikhNo ratings yet
- CD4 Count CutDocument51 pagesCD4 Count Cutibrahim 12No ratings yet
- Savva2016 PDFDocument8 pagesSavva2016 PDFHenry Rivero GarciaNo ratings yet
- Krauses Essential HumanDocument315 pagesKrauses Essential HumanEllah MaeNo ratings yet
- (Adhikari, 2019) PDFDocument8 pages(Adhikari, 2019) PDFPaulo Zadit Mendivelso OsorioNo ratings yet
- Section 2 - NutritionDocument9 pagesSection 2 - NutritionOsmany MadrigalNo ratings yet
- Pantothenic Acid and Weight ReductionDocument16 pagesPantothenic Acid and Weight ReductionkirpicsisNo ratings yet
- FructoseDocument23 pagesFructoseManish TiwariNo ratings yet
- Mojahid Sheet Complete PDFDocument176 pagesMojahid Sheet Complete PDFOsman SomiNo ratings yet
- Carbohydrate MetabolismDocument16 pagesCarbohydrate MetabolismKiran NiaziNo ratings yet
- Define VitaminsDocument22 pagesDefine Vitaminsantesar reheemNo ratings yet
- Research Essay Final DraftDocument14 pagesResearch Essay Final Draftapi-519288352No ratings yet
- Request For Strategic Advice On Business Schools in Scottish UniversitiesDocument22 pagesRequest For Strategic Advice On Business Schools in Scottish UniversitiesThe Royal Society of EdinburghNo ratings yet
- Advanced Nutritional BiochemistryDocument90 pagesAdvanced Nutritional BiochemistryAkinleye peter100% (1)
- Biological ChemistryDocument28 pagesBiological ChemistryArsilan Aziz LoneNo ratings yet
- Chapter 5 Glucose HomeostasisDocument15 pagesChapter 5 Glucose Homeostasistliviu334066No ratings yet
- Disorders of The Alimentary TractDocument25 pagesDisorders of The Alimentary Tract수안현100% (1)
- What Are LipoproteinsDocument18 pagesWhat Are Lipoproteinsarsal1cheema-88705No ratings yet
- Basetext CombiDocument58 pagesBasetext CombiJiHyun ParkNo ratings yet
- Social Anxiety and Its Effects1Document12 pagesSocial Anxiety and Its Effects1api-395503981No ratings yet
- AlcoholismDocument19 pagesAlcoholismKweng Kweng DoongNo ratings yet
- Renukaprasad Ys - Medicine - Thesis NewDocument110 pagesRenukaprasad Ys - Medicine - Thesis NewLokesh ChopraNo ratings yet
- Preparing The New Psychology Professoriate:: Helping Graduate Students Become Competent TeachersDocument176 pagesPreparing The New Psychology Professoriate:: Helping Graduate Students Become Competent TeachersNeilermindNo ratings yet
- 2020 Investigacion Publicaciones NeuropsychologicalDeficitsDocument24 pages2020 Investigacion Publicaciones NeuropsychologicalDeficitsJose Antonio Piqueras RodríguezNo ratings yet
- Waxes: Structure, Composition, Occurrence and AnalysisDocument27 pagesWaxes: Structure, Composition, Occurrence and AnalysisNanda Rizky FathiyaNo ratings yet
- Chemistry ProjectDocument17 pagesChemistry ProjectSurajNo ratings yet
- Tection Thin, F3-Cryptoxanthin, Lycopene, A-Carotene,: Trans-P-CarDocument6 pagesTection Thin, F3-Cryptoxanthin, Lycopene, A-Carotene,: Trans-P-CarMaría JoséNo ratings yet
- CO Week 3 Endokrin MICHAEL GERALDI L.Document10 pagesCO Week 3 Endokrin MICHAEL GERALDI L.Michael GNo ratings yet
- Anxiety: Wiki Loves Monuments: Photograph A Monument, Help Wikipedia and Win!Document35 pagesAnxiety: Wiki Loves Monuments: Photograph A Monument, Help Wikipedia and Win!Jennie KimNo ratings yet
- Careers in SociologyDocument11 pagesCareers in SociologyMuhammad GhufranNo ratings yet
- Heart DiseaseDocument38 pagesHeart DiseaseDr.Sunil KumarNo ratings yet
- Intro Research EngDocument24 pagesIntro Research EngRupert John LeeNo ratings yet
- Arun Chem ProjectDocument33 pagesArun Chem ProjectGaurav TomarNo ratings yet
- Cloudera EDH ExecutiveBriefDocument4 pagesCloudera EDH ExecutiveBriefMark LoboNo ratings yet
- IV. Recognizing National Issues and Concern - E-Substance Abuse EducationDocument9 pagesIV. Recognizing National Issues and Concern - E-Substance Abuse EducationMicsjadeCastillo0% (1)
- Scientific Study Thoughts Feelings Behaviors Empirical Psychological Measurable Cultural Norms Human Behavior Mental States SituationsDocument8 pagesScientific Study Thoughts Feelings Behaviors Empirical Psychological Measurable Cultural Norms Human Behavior Mental States SituationsJohan Shane CarsidoNo ratings yet
- Research EssayDocument10 pagesResearch Essaynel50% (2)
- Textbook of Introduction To EnvironmentaDocument134 pagesTextbook of Introduction To EnvironmentayadvinderNo ratings yet
- Foundation Course-I Project (SEM-1) 2017-18: and Remedial MeasuresDocument21 pagesFoundation Course-I Project (SEM-1) 2017-18: and Remedial MeasuresYasin Shaikh75% (4)
- 03 Prevalence Clinical 2Document12 pages03 Prevalence Clinical 2Rafael Martins0% (1)
- Fundamentals of PhytonutritionDocument5 pagesFundamentals of PhytonutritionNasir AhmedNo ratings yet
- RBJ DWX HMUa X4Document371 pagesRBJ DWX HMUa X4Delia Dascalu0% (1)
- Dietary Fiber & MetabolismDocument24 pagesDietary Fiber & MetabolismRomana VulturarNo ratings yet
- Facts About Milk 2Document15 pagesFacts About Milk 2hanisah ahmad jaafarNo ratings yet
- The Lipids What Are Lipids?Document16 pagesThe Lipids What Are Lipids?Sire100% (1)
- Corneal DystrophyDocument5 pagesCorneal DystrophyDejan JanevNo ratings yet
- B-Complex Vitamins Role in Energy ReleaseDocument5 pagesB-Complex Vitamins Role in Energy ReleaseEno WijayantiNo ratings yet
- Panic Attack Symptomatology and Anxiety Sensitivity in AdolescentsDocument10 pagesPanic Attack Symptomatology and Anxiety Sensitivity in AdolescentsBálint KapturNo ratings yet
- NMLSbookDocument386 pagesNMLSbookejsimonsenNo ratings yet
- XLR I Prospectus 2016Document60 pagesXLR I Prospectus 2016rishabh01234No ratings yet
- Acute PericarditisDocument8 pagesAcute Pericarditisalina abu rumiNo ratings yet
- Molecules: Viral Hepatitis and Iron Dysregulation: Molecular Pathways and The Role of LactoferrinDocument21 pagesMolecules: Viral Hepatitis and Iron Dysregulation: Molecular Pathways and The Role of Lactoferrint.araujoNo ratings yet
- Soluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesDocument11 pagesSoluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesShiela Montances100% (1)
- First Aid in The NatureDocument19 pagesFirst Aid in The NatureЮлия ЦыгановаNo ratings yet
- Hemophilia and Coagulation Disorders: DR Nishant VermaDocument68 pagesHemophilia and Coagulation Disorders: DR Nishant VermaЮлия ЦыгановаNo ratings yet
- Liver Pathology: CirrhosisDocument18 pagesLiver Pathology: CirrhosisЮлия ЦыгановаNo ratings yet
- Cirrhosis and Complications: Best of ILC 2019Document29 pagesCirrhosis and Complications: Best of ILC 2019Юлия ЦыгановаNo ratings yet
- Fatty Liver: Millions of Liver Suffer in SilenceDocument40 pagesFatty Liver: Millions of Liver Suffer in SilenceTafsir arefinNo ratings yet
- ATTAR49Document10 pagesATTAR49vlande897No ratings yet
- Lupin DiagnoticsDocument16 pagesLupin Diagnoticsdrsujeetkumar5869No ratings yet
- Clinical Examination Obstructive Jaundice PrabedasDocument47 pagesClinical Examination Obstructive Jaundice PrabedasThompson CatNo ratings yet
- PdfText (38) - 240317 - 201242Document7 pagesPdfText (38) - 240317 - 201242Anurag SharmaNo ratings yet
- Test #24 Q.Id 863 Question 1 of 39 Item Review Division: HepatologyDocument47 pagesTest #24 Q.Id 863 Question 1 of 39 Item Review Division: HepatologyJahangir AlamNo ratings yet
- Prime Full Body Check-Up: Test Description Value(s) Unit(s) Reference RangeDocument10 pagesPrime Full Body Check-Up: Test Description Value(s) Unit(s) Reference RangeNarendra KumarNo ratings yet
- Ramadanandliverdisorders PDFDocument7 pagesRamadanandliverdisorders PDFRaissa Virgy RiandaNo ratings yet
- Effects of Vernonia Amygdalina (Bitter Leaf) On The Bio-Marker of Oxidative Stress in Accetaminophen Induced Liver Damage of Albino RatsDocument12 pagesEffects of Vernonia Amygdalina (Bitter Leaf) On The Bio-Marker of Oxidative Stress in Accetaminophen Induced Liver Damage of Albino Ratsiaset123No ratings yet
- Daftar PustakaDocument8 pagesDaftar PustakaErlin IrawatiNo ratings yet
- Referinte Analize LabDocument14 pagesReferinte Analize LabDiana CâmpeanNo ratings yet
- Alt GPTDocument1 pageAlt GPTEnrique DuarteNo ratings yet
- Haematology, Biochemistry, Serology and Immunology, Microbiology, Cytology, Histopathology, Endocrinology, Ultrasonography & X-RayDocument2 pagesHaematology, Biochemistry, Serology and Immunology, Microbiology, Cytology, Histopathology, Endocrinology, Ultrasonography & X-RayPankaj BeniwalNo ratings yet
- Chemistry: Test Name Results Unit Reference Ranges Last Available ResultsDocument1 pageChemistry: Test Name Results Unit Reference Ranges Last Available ResultsHalima MajeedNo ratings yet
- Clinical EnzymologyDocument38 pagesClinical EnzymologyLloyd Jay LinNo ratings yet
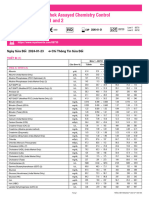
- Lyphochek Assayed Chemistry Control Levels 1 and 2: Ngày Sửa Đổi 2024-01-23 Chỉ Thông Tin Sửa ĐổiDocument2 pagesLyphochek Assayed Chemistry Control Levels 1 and 2: Ngày Sửa Đổi 2024-01-23 Chỉ Thông Tin Sửa ĐổiquankddNo ratings yet
- (Mod. IFCC Method) For The Determination of SGPT (ALT) Activity in Serum. (For in Vitro Diagnostic Use Only)Document1 page(Mod. IFCC Method) For The Determination of SGPT (ALT) Activity in Serum. (For in Vitro Diagnostic Use Only)Dinesh SreedharanNo ratings yet
- Alt (GPT) Ifcc LS BXC0213 A25 A15 PDFDocument2 pagesAlt (GPT) Ifcc LS BXC0213 A25 A15 PDFjef1234321No ratings yet
- Sanet - ST Handbook - Of.200.medicinal - Plants 2 PDFDocument2,076 pagesSanet - ST Handbook - Of.200.medicinal - Plants 2 PDFsmr76788% (8)
- Akc and CKC Registration Certificates-MergedDocument20 pagesAkc and CKC Registration Certificates-Mergedapi-370468914No ratings yet
- Daviss Comprehensive Handbook of Laboratory Diagnostic Tests With Nursing Implications 6th Edition Leeuwen Test BankDocument18 pagesDaviss Comprehensive Handbook of Laboratory Diagnostic Tests With Nursing Implications 6th Edition Leeuwen Test BankCoreyMoyereinmw100% (17)
- LankaBangla Credit Card Reward Program October 2018Document4 pagesLankaBangla Credit Card Reward Program October 2018sabbirmohiNo ratings yet
- EnzymesDocument60 pagesEnzymesRia AlcantaraNo ratings yet
- A. Hematology Reagent Temperature: Reagent or Test TemperaturesDocument7 pagesA. Hematology Reagent Temperature: Reagent or Test TemperaturesyowubhatoriNo ratings yet
- Liver Function Tests and How To Relate ThemDocument82 pagesLiver Function Tests and How To Relate ThemG VenkateshNo ratings yet
- Sigma Metrics and Quality Goal Index Ratio - 2Document6 pagesSigma Metrics and Quality Goal Index Ratio - 2Phi De TranNo ratings yet
- Pgy 3419 2amino Acid Metabolism 2021 PDFDocument47 pagesPgy 3419 2amino Acid Metabolism 2021 PDFDesmond BwalyaNo ratings yet
- Acute and Sub-Chronic Pre-Clinical Toxicological Study of Averrhoa Carambola L. (Oxalidaceae)Document9 pagesAcute and Sub-Chronic Pre-Clinical Toxicological Study of Averrhoa Carambola L. (Oxalidaceae)Red DiggerNo ratings yet





























































































Download as doc, pdf, or txt
You might also like
- Usmle Free 150Document44 pagesUsmle Free 150ironslave100% (1)
- 15casebook in Gastroenterology PDFDocument109 pages15casebook in Gastroenterology PDFKMNo ratings yet
- Obesity Term PaperDocument20 pagesObesity Term PaperBave EnriquezNo ratings yet
- Biochemistry: For The Students of Pharmacy Technicians (Category-B)Document74 pagesBiochemistry: For The Students of Pharmacy Technicians (Category-B)Rajesh Kumar0% (1)
- Alanine Aminotransferase (Alt-Gpt)Document1 pageAlanine Aminotransferase (Alt-Gpt)Risqon Anjahiranda Adiputra50% (2)
- Metabolites: Physiological Responses of Post-Dietary Effects: Lessons From Pre-Clinical and Clinical StudiesDocument16 pagesMetabolites: Physiological Responses of Post-Dietary Effects: Lessons From Pre-Clinical and Clinical StudiesSarah OctaviaNo ratings yet
- Volume 13, Issue 2, August 2012 - Helicobacter Pylori Infection in Superficial Gastritis, Erosive Gastritis and Gastric UlcerDocument6 pagesVolume 13, Issue 2, August 2012 - Helicobacter Pylori Infection in Superficial Gastritis, Erosive Gastritis and Gastric UlcerAndy SelvianNo ratings yet
- Hrkansh NotesDocument424 pagesHrkansh NotesAhmed RagabNo ratings yet
- AP-Food List TPCM PDFDocument12 pagesAP-Food List TPCM PDFS K ChughNo ratings yet
- BiochemDocument10 pagesBiochemWaseem Abbas ShaikhNo ratings yet
- CD4 Count CutDocument51 pagesCD4 Count Cutibrahim 12No ratings yet
- Savva2016 PDFDocument8 pagesSavva2016 PDFHenry Rivero GarciaNo ratings yet
- Krauses Essential HumanDocument315 pagesKrauses Essential HumanEllah MaeNo ratings yet
- (Adhikari, 2019) PDFDocument8 pages(Adhikari, 2019) PDFPaulo Zadit Mendivelso OsorioNo ratings yet
- Section 2 - NutritionDocument9 pagesSection 2 - NutritionOsmany MadrigalNo ratings yet
- Pantothenic Acid and Weight ReductionDocument16 pagesPantothenic Acid and Weight ReductionkirpicsisNo ratings yet
- FructoseDocument23 pagesFructoseManish TiwariNo ratings yet
- Mojahid Sheet Complete PDFDocument176 pagesMojahid Sheet Complete PDFOsman SomiNo ratings yet
- Carbohydrate MetabolismDocument16 pagesCarbohydrate MetabolismKiran NiaziNo ratings yet
- Define VitaminsDocument22 pagesDefine Vitaminsantesar reheemNo ratings yet
- Research Essay Final DraftDocument14 pagesResearch Essay Final Draftapi-519288352No ratings yet
- Request For Strategic Advice On Business Schools in Scottish UniversitiesDocument22 pagesRequest For Strategic Advice On Business Schools in Scottish UniversitiesThe Royal Society of EdinburghNo ratings yet
- Advanced Nutritional BiochemistryDocument90 pagesAdvanced Nutritional BiochemistryAkinleye peter100% (1)
- Biological ChemistryDocument28 pagesBiological ChemistryArsilan Aziz LoneNo ratings yet
- Chapter 5 Glucose HomeostasisDocument15 pagesChapter 5 Glucose Homeostasistliviu334066No ratings yet
- Disorders of The Alimentary TractDocument25 pagesDisorders of The Alimentary Tract수안현100% (1)
- What Are LipoproteinsDocument18 pagesWhat Are Lipoproteinsarsal1cheema-88705No ratings yet
- Basetext CombiDocument58 pagesBasetext CombiJiHyun ParkNo ratings yet
- Social Anxiety and Its Effects1Document12 pagesSocial Anxiety and Its Effects1api-395503981No ratings yet
- AlcoholismDocument19 pagesAlcoholismKweng Kweng DoongNo ratings yet
- Renukaprasad Ys - Medicine - Thesis NewDocument110 pagesRenukaprasad Ys - Medicine - Thesis NewLokesh ChopraNo ratings yet
- Preparing The New Psychology Professoriate:: Helping Graduate Students Become Competent TeachersDocument176 pagesPreparing The New Psychology Professoriate:: Helping Graduate Students Become Competent TeachersNeilermindNo ratings yet
- 2020 Investigacion Publicaciones NeuropsychologicalDeficitsDocument24 pages2020 Investigacion Publicaciones NeuropsychologicalDeficitsJose Antonio Piqueras RodríguezNo ratings yet
- Waxes: Structure, Composition, Occurrence and AnalysisDocument27 pagesWaxes: Structure, Composition, Occurrence and AnalysisNanda Rizky FathiyaNo ratings yet
- Chemistry ProjectDocument17 pagesChemistry ProjectSurajNo ratings yet
- Tection Thin, F3-Cryptoxanthin, Lycopene, A-Carotene,: Trans-P-CarDocument6 pagesTection Thin, F3-Cryptoxanthin, Lycopene, A-Carotene,: Trans-P-CarMaría JoséNo ratings yet
- CO Week 3 Endokrin MICHAEL GERALDI L.Document10 pagesCO Week 3 Endokrin MICHAEL GERALDI L.Michael GNo ratings yet
- Anxiety: Wiki Loves Monuments: Photograph A Monument, Help Wikipedia and Win!Document35 pagesAnxiety: Wiki Loves Monuments: Photograph A Monument, Help Wikipedia and Win!Jennie KimNo ratings yet
- Careers in SociologyDocument11 pagesCareers in SociologyMuhammad GhufranNo ratings yet
- Heart DiseaseDocument38 pagesHeart DiseaseDr.Sunil KumarNo ratings yet
- Intro Research EngDocument24 pagesIntro Research EngRupert John LeeNo ratings yet
- Arun Chem ProjectDocument33 pagesArun Chem ProjectGaurav TomarNo ratings yet
- Cloudera EDH ExecutiveBriefDocument4 pagesCloudera EDH ExecutiveBriefMark LoboNo ratings yet
- IV. Recognizing National Issues and Concern - E-Substance Abuse EducationDocument9 pagesIV. Recognizing National Issues and Concern - E-Substance Abuse EducationMicsjadeCastillo0% (1)
- Scientific Study Thoughts Feelings Behaviors Empirical Psychological Measurable Cultural Norms Human Behavior Mental States SituationsDocument8 pagesScientific Study Thoughts Feelings Behaviors Empirical Psychological Measurable Cultural Norms Human Behavior Mental States SituationsJohan Shane CarsidoNo ratings yet
- Research EssayDocument10 pagesResearch Essaynel50% (2)
- Textbook of Introduction To EnvironmentaDocument134 pagesTextbook of Introduction To EnvironmentayadvinderNo ratings yet
- Foundation Course-I Project (SEM-1) 2017-18: and Remedial MeasuresDocument21 pagesFoundation Course-I Project (SEM-1) 2017-18: and Remedial MeasuresYasin Shaikh75% (4)
- 03 Prevalence Clinical 2Document12 pages03 Prevalence Clinical 2Rafael Martins0% (1)
- Fundamentals of PhytonutritionDocument5 pagesFundamentals of PhytonutritionNasir AhmedNo ratings yet
- RBJ DWX HMUa X4Document371 pagesRBJ DWX HMUa X4Delia Dascalu0% (1)
- Dietary Fiber & MetabolismDocument24 pagesDietary Fiber & MetabolismRomana VulturarNo ratings yet
- Facts About Milk 2Document15 pagesFacts About Milk 2hanisah ahmad jaafarNo ratings yet
- The Lipids What Are Lipids?Document16 pagesThe Lipids What Are Lipids?Sire100% (1)
- Corneal DystrophyDocument5 pagesCorneal DystrophyDejan JanevNo ratings yet
- B-Complex Vitamins Role in Energy ReleaseDocument5 pagesB-Complex Vitamins Role in Energy ReleaseEno WijayantiNo ratings yet
- Panic Attack Symptomatology and Anxiety Sensitivity in AdolescentsDocument10 pagesPanic Attack Symptomatology and Anxiety Sensitivity in AdolescentsBálint KapturNo ratings yet
- NMLSbookDocument386 pagesNMLSbookejsimonsenNo ratings yet
- XLR I Prospectus 2016Document60 pagesXLR I Prospectus 2016rishabh01234No ratings yet
- Acute PericarditisDocument8 pagesAcute Pericarditisalina abu rumiNo ratings yet
- Molecules: Viral Hepatitis and Iron Dysregulation: Molecular Pathways and The Role of LactoferrinDocument21 pagesMolecules: Viral Hepatitis and Iron Dysregulation: Molecular Pathways and The Role of Lactoferrint.araujoNo ratings yet
- Soluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesDocument11 pagesSoluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesShiela Montances100% (1)
- First Aid in The NatureDocument19 pagesFirst Aid in The NatureЮлия ЦыгановаNo ratings yet
- Hemophilia and Coagulation Disorders: DR Nishant VermaDocument68 pagesHemophilia and Coagulation Disorders: DR Nishant VermaЮлия ЦыгановаNo ratings yet
- Liver Pathology: CirrhosisDocument18 pagesLiver Pathology: CirrhosisЮлия ЦыгановаNo ratings yet
- Cirrhosis and Complications: Best of ILC 2019Document29 pagesCirrhosis and Complications: Best of ILC 2019Юлия ЦыгановаNo ratings yet
- Fatty Liver: Millions of Liver Suffer in SilenceDocument40 pagesFatty Liver: Millions of Liver Suffer in SilenceTafsir arefinNo ratings yet
- ATTAR49Document10 pagesATTAR49vlande897No ratings yet
- Lupin DiagnoticsDocument16 pagesLupin Diagnoticsdrsujeetkumar5869No ratings yet
- Clinical Examination Obstructive Jaundice PrabedasDocument47 pagesClinical Examination Obstructive Jaundice PrabedasThompson CatNo ratings yet
- PdfText (38) - 240317 - 201242Document7 pagesPdfText (38) - 240317 - 201242Anurag SharmaNo ratings yet
- Test #24 Q.Id 863 Question 1 of 39 Item Review Division: HepatologyDocument47 pagesTest #24 Q.Id 863 Question 1 of 39 Item Review Division: HepatologyJahangir AlamNo ratings yet
- Prime Full Body Check-Up: Test Description Value(s) Unit(s) Reference RangeDocument10 pagesPrime Full Body Check-Up: Test Description Value(s) Unit(s) Reference RangeNarendra KumarNo ratings yet
- Ramadanandliverdisorders PDFDocument7 pagesRamadanandliverdisorders PDFRaissa Virgy RiandaNo ratings yet
- Effects of Vernonia Amygdalina (Bitter Leaf) On The Bio-Marker of Oxidative Stress in Accetaminophen Induced Liver Damage of Albino RatsDocument12 pagesEffects of Vernonia Amygdalina (Bitter Leaf) On The Bio-Marker of Oxidative Stress in Accetaminophen Induced Liver Damage of Albino Ratsiaset123No ratings yet
- Daftar PustakaDocument8 pagesDaftar PustakaErlin IrawatiNo ratings yet
- Referinte Analize LabDocument14 pagesReferinte Analize LabDiana CâmpeanNo ratings yet
- Alt GPTDocument1 pageAlt GPTEnrique DuarteNo ratings yet
- Haematology, Biochemistry, Serology and Immunology, Microbiology, Cytology, Histopathology, Endocrinology, Ultrasonography & X-RayDocument2 pagesHaematology, Biochemistry, Serology and Immunology, Microbiology, Cytology, Histopathology, Endocrinology, Ultrasonography & X-RayPankaj BeniwalNo ratings yet
- Chemistry: Test Name Results Unit Reference Ranges Last Available ResultsDocument1 pageChemistry: Test Name Results Unit Reference Ranges Last Available ResultsHalima MajeedNo ratings yet
- Clinical EnzymologyDocument38 pagesClinical EnzymologyLloyd Jay LinNo ratings yet
- Lyphochek Assayed Chemistry Control Levels 1 and 2: Ngày Sửa Đổi 2024-01-23 Chỉ Thông Tin Sửa ĐổiDocument2 pagesLyphochek Assayed Chemistry Control Levels 1 and 2: Ngày Sửa Đổi 2024-01-23 Chỉ Thông Tin Sửa ĐổiquankddNo ratings yet
- (Mod. IFCC Method) For The Determination of SGPT (ALT) Activity in Serum. (For in Vitro Diagnostic Use Only)Document1 page(Mod. IFCC Method) For The Determination of SGPT (ALT) Activity in Serum. (For in Vitro Diagnostic Use Only)Dinesh SreedharanNo ratings yet
- Alt (GPT) Ifcc LS BXC0213 A25 A15 PDFDocument2 pagesAlt (GPT) Ifcc LS BXC0213 A25 A15 PDFjef1234321No ratings yet
- Sanet - ST Handbook - Of.200.medicinal - Plants 2 PDFDocument2,076 pagesSanet - ST Handbook - Of.200.medicinal - Plants 2 PDFsmr76788% (8)
- Akc and CKC Registration Certificates-MergedDocument20 pagesAkc and CKC Registration Certificates-Mergedapi-370468914No ratings yet
- Daviss Comprehensive Handbook of Laboratory Diagnostic Tests With Nursing Implications 6th Edition Leeuwen Test BankDocument18 pagesDaviss Comprehensive Handbook of Laboratory Diagnostic Tests With Nursing Implications 6th Edition Leeuwen Test BankCoreyMoyereinmw100% (17)
- LankaBangla Credit Card Reward Program October 2018Document4 pagesLankaBangla Credit Card Reward Program October 2018sabbirmohiNo ratings yet
- EnzymesDocument60 pagesEnzymesRia AlcantaraNo ratings yet
- A. Hematology Reagent Temperature: Reagent or Test TemperaturesDocument7 pagesA. Hematology Reagent Temperature: Reagent or Test TemperaturesyowubhatoriNo ratings yet
- Liver Function Tests and How To Relate ThemDocument82 pagesLiver Function Tests and How To Relate ThemG VenkateshNo ratings yet
- Sigma Metrics and Quality Goal Index Ratio - 2Document6 pagesSigma Metrics and Quality Goal Index Ratio - 2Phi De TranNo ratings yet
- Pgy 3419 2amino Acid Metabolism 2021 PDFDocument47 pagesPgy 3419 2amino Acid Metabolism 2021 PDFDesmond BwalyaNo ratings yet
- Acute and Sub-Chronic Pre-Clinical Toxicological Study of Averrhoa Carambola L. (Oxalidaceae)Document9 pagesAcute and Sub-Chronic Pre-Clinical Toxicological Study of Averrhoa Carambola L. (Oxalidaceae)Red DiggerNo ratings yet