Download as pdf or txt
You might also like
- Clinical Internal Medicine Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2From EverandClinical Internal Medicine Review 2023: For USMLE Step 2 CK and COMLEX-USA Level 2Rating: 4 out of 5 stars4/5 (2)
- Cancer ScreeningDocument37 pagesCancer ScreeningTomb RaiderNo ratings yet
- Pap TestDocument24 pagesPap TestAmirah MuhammadNo ratings yet
- Best Tarot Book 25Document5 pagesBest Tarot Book 25Classic Bobby100% (3)
- OCSPScreeningGuidelines June2020Document1 pageOCSPScreeningGuidelines June2020ixNo ratings yet
- Pap SmearDocument32 pagesPap SmearAmira Nasir100% (1)
- Pap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.DDocument22 pagesPap Smear Guidelines: Baylor College of Medicine Anoop Agrawal, M.Dshygirl72No ratings yet
- Guidelines Colposcopy and Pap Smear Triage GuidelinesDocument12 pagesGuidelines Colposcopy and Pap Smear Triage Guidelinesbabarpdu100% (1)
- Management of Cervical Smears GoldenDocument47 pagesManagement of Cervical Smears GoldenFelixNo ratings yet
- Managment of Abnormal Pap SmearDocument78 pagesManagment of Abnormal Pap SmearMohammad AlrefaiNo ratings yet
- CYT 2113 Cytology I: Lesson 7: Introduction To Pap Smear TestDocument48 pagesCYT 2113 Cytology I: Lesson 7: Introduction To Pap Smear TestCarinaJongLeeNo ratings yet
- Abnormal Paps: DR Vidhi ChaudharyDocument29 pagesAbnormal Paps: DR Vidhi Chaudharyvidhi chaudharyNo ratings yet
- Pap Smear - Overview, Indications, PreparationDocument11 pagesPap Smear - Overview, Indications, PreparationBayu Surya DanaNo ratings yet
- CS-PUB-LAB-1 Cervical Cytology Management Recommendations Explanatory GuideDocument11 pagesCS-PUB-LAB-1 Cervical Cytology Management Recommendations Explanatory GuideMc Coral100% (1)
- P Ap SmearDocument4 pagesP Ap SmearKinjal VasavaNo ratings yet
- Screening of Cancer CervixDocument39 pagesScreening of Cancer CervixAnkur Yadav100% (1)
- Pap SmearDocument8 pagesPap Smearsmv2No ratings yet
- Management of The Abnormal Pap SmearDocument29 pagesManagement of The Abnormal Pap SmearMakWohWeiNo ratings yet
- Cervical Cancer ScreeningDocument1 pageCervical Cancer Screeningtavo823No ratings yet
- My Pap Smear Is Abnormal !Document70 pagesMy Pap Smear Is Abnormal !Alena JosephNo ratings yet
- Cervical Cancer Screening - AHS GuidelineDocument9 pagesCervical Cancer Screening - AHS GuidelineBasil al-hashaikehNo ratings yet
- 2021 Adult Preventive Health GuidelinesDocument8 pages2021 Adult Preventive Health GuidelinesAnthony El HageNo ratings yet
- 2019AdultPreventiveHealthGuidelines PDFDocument7 pages2019AdultPreventiveHealthGuidelines PDFvesvNo ratings yet
- The American Cancer Society Recommends The Following Guidelines For EarlyDocument2 pagesThe American Cancer Society Recommends The Following Guidelines For EarlyRatih Kusuma Dewi ArfaNo ratings yet
- Cervical CancerDocument4 pagesCervical CancerInomy Claudia Katherine ImbiriNo ratings yet
- 2021 Intraepithelial Neoplasia and Carcinoma of The Cervix (Document48 pages2021 Intraepithelial Neoplasia and Carcinoma of The Cervix (KarenNo ratings yet
- Gynae-L - MukundaDocument50 pagesGynae-L - MukundadocivirusNo ratings yet
- Pap SmearDocument4 pagesPap SmearRamy AsollaremNo ratings yet
- HMC Pap Guidelines November 2007Document1 pageHMC Pap Guidelines November 2007Nikki Mariz DepayNo ratings yet
- Management of Abnormal Pap Smears PresentationDocument17 pagesManagement of Abnormal Pap Smears Presentationapi-210786702100% (2)
- Cervical Cancer ScreeningDocument25 pagesCervical Cancer Screening6ixSideCreate MNo ratings yet
- PDFsam ObGynDocument4 pagesPDFsam ObGynAlessandro ZadraNo ratings yet
- N-Acetyl-Cysteine in Anovulatory Women: The Impact of Postcoital TestDocument4 pagesN-Acetyl-Cysteine in Anovulatory Women: The Impact of Postcoital TestRahma Evasari LubisNo ratings yet
- Faq085-Ervical Cancer ScreeningDocument3 pagesFaq085-Ervical Cancer ScreeningTjoema AsriNo ratings yet
- Cervical Cancer ScreeningDocument25 pagesCervical Cancer ScreeningDr VermaNo ratings yet
- Cancer Screening and Prevention:: Eliminating Deaths From Cervical CancerDocument45 pagesCancer Screening and Prevention:: Eliminating Deaths From Cervical CancerYingting ZooNo ratings yet
- Pendahuluan Pap SmearDocument14 pagesPendahuluan Pap SmearAyu NurlinaNo ratings yet
- ASCCP Management Guidelines - August 2014 PDFDocument24 pagesASCCP Management Guidelines - August 2014 PDFAnita BlazevskaNo ratings yet
- Gyn Screening PresentationDocument27 pagesGyn Screening Presentationapi-437704700100% (1)
- Approach To Breast..maha - PPTX 2Document38 pagesApproach To Breast..maha - PPTX 2Meno Ali50% (2)
- Unit 1 - Approach To The Patient - 30qDocument19 pagesUnit 1 - Approach To The Patient - 30qaeltee100% (1)
- FMcase 1Document24 pagesFMcase 1Ryan Townsend100% (2)
- Surabaya-Deteksi Dini Kanker Serviks UteriDocument32 pagesSurabaya-Deteksi Dini Kanker Serviks Uteripuskesmas manukan kulonNo ratings yet
- 22CRC 45new50 Brochure Trifold PRINTDocument2 pages22CRC 45new50 Brochure Trifold PRINTdingyshoreNo ratings yet
- Cervical Dysplasia and CancerDocument25 pagesCervical Dysplasia and CancerSarfarosh AhmadNo ratings yet
- NHS Cervical Screening: Helping You DecideDocument16 pagesNHS Cervical Screening: Helping You DecideBoy100% (1)
- Screening For Colorectal CancerDocument13 pagesScreening For Colorectal CancerPeewee AisyNo ratings yet
- Sitologi PDFDocument31 pagesSitologi PDFNadila Putri MaharaniNo ratings yet
- Health Maintenance GuidelinesDocument2 pagesHealth Maintenance GuidelinesmtataNo ratings yet
- Belle Cervical DiseaseDocument7 pagesBelle Cervical DiseaseRashed ShatnawiNo ratings yet
- Cervical Screening NewDocument17 pagesCervical Screening NewmesseeeNo ratings yet
- Undescended Testicle PathwayDocument8 pagesUndescended Testicle PathwayJessa MaeNo ratings yet
- Do Cervical Cancer Screening Recommendations Differ Among Women at Different Age Groups?Document8 pagesDo Cervical Cancer Screening Recommendations Differ Among Women at Different Age Groups?Nico Angelo CopoNo ratings yet
- Breast LectureDocument98 pagesBreast LectureTopher ReyesNo ratings yet
- Incorrect. The Correct Answer Is (D)Document5 pagesIncorrect. The Correct Answer Is (D)samgeorgyNo ratings yet
- Converted - SCREENING FOR CANCER OF THE CERVIXDocument29 pagesConverted - SCREENING FOR CANCER OF THE CERVIXSihle SibekoNo ratings yet
- Ectopic PregnancyDocument55 pagesEctopic PregnancyDr-Saja O. DmourNo ratings yet
- Sheryl Ann Pedines Bsn-IvDocument4 pagesSheryl Ann Pedines Bsn-IvSheryl Ann Barit PedinesNo ratings yet
- Infertility: PGI Ira Mikkaella GenobisDocument49 pagesInfertility: PGI Ira Mikkaella GenobisIra Mikkaella GenobisNo ratings yet
- Screening For Cancer of The Cervix: An Office Manual For Health Care ProvidersDocument16 pagesScreening For Cancer of The Cervix: An Office Manual For Health Care ProvidersYosie Yulanda PutraNo ratings yet
- Guidelines Screening USADocument2 pagesGuidelines Screening USAAyu RahmaNo ratings yet
- Explaining History of RomeDocument154 pagesExplaining History of RomeAli HusseinNo ratings yet
- Khalid Alfaki PedDocument21 pagesKhalid Alfaki PedAli HusseinNo ratings yet
- Result of Fmge (Screening Test), June 2021 SessionDocument121 pagesResult of Fmge (Screening Test), June 2021 SessionAli HusseinNo ratings yet
- Morning Pharma Dose Day 4Document2 pagesMorning Pharma Dose Day 4Ali HusseinNo ratings yet
- Morning Pharma Dose Day 3Document2 pagesMorning Pharma Dose Day 3Ali HusseinNo ratings yet
- June 2021 MCQ Psychiatry at DAMSDocument61 pagesJune 2021 MCQ Psychiatry at DAMSAli HusseinNo ratings yet
- Paediatric ALS A3Document1 pagePaediatric ALS A3Ali HusseinNo ratings yet
- Influenza Guideline 2015-16Document28 pagesInfluenza Guideline 2015-16Ali HusseinNo ratings yet
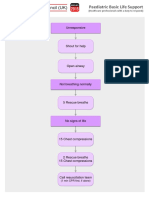
- Paediatric Basic Life Support: UnresponsiveDocument1 pagePaediatric Basic Life Support: UnresponsiveAli HusseinNo ratings yet
- How To Approach Any Cancer Patient: Levofloxacin)Document2 pagesHow To Approach Any Cancer Patient: Levofloxacin)Ali HusseinNo ratings yet
- Paediatric Choking Treatment-A3Document1 pagePaediatric Choking Treatment-A3Ali HusseinNo ratings yet
- G.R. No. 138774 March 8, 2001 Regina Francisco and Zenaida PASCUAL, Petitioners, Aida Francisco-ALFONSO, Respondent. Pardo, J.Document12 pagesG.R. No. 138774 March 8, 2001 Regina Francisco and Zenaida PASCUAL, Petitioners, Aida Francisco-ALFONSO, Respondent. Pardo, J.JuralexNo ratings yet
- Shangla Girls School: Summer Camp 2019Document5 pagesShangla Girls School: Summer Camp 2019Moyz RahmanNo ratings yet
- 55122505241#5852#55122505241#9 - 16 - 2022 12 - 00 - 00 AmDocument2 pages55122505241#5852#55122505241#9 - 16 - 2022 12 - 00 - 00 AmAdham ZidanNo ratings yet
- FN-LM07 Filipinos Conquering The WorldDocument3 pagesFN-LM07 Filipinos Conquering The WorldMichelle Em GerabanNo ratings yet
- Biomarkers of Bone Health and Osteoporosis Risk Symposium On Diet and Bone HealthDocument6 pagesBiomarkers of Bone Health and Osteoporosis Risk Symposium On Diet and Bone HealthDaniel SilvaNo ratings yet
- Assignment 2 Rahul Garg, 2020115006 IDocument8 pagesAssignment 2 Rahul Garg, 2020115006 ISrijan ChakrabortyNo ratings yet
- Details of Module and Its Structure: Ms. Kulwant KaurDocument14 pagesDetails of Module and Its Structure: Ms. Kulwant KaurAnkur TiwariNo ratings yet
- People Vs Rizal (1981)Document21 pagesPeople Vs Rizal (1981)Abigail DeeNo ratings yet
- Odeona Grecian Urn: by John KeatsDocument10 pagesOdeona Grecian Urn: by John KeatsjayeNo ratings yet
- How To Answer Stupid Job Interview Questions - LinkedInDocument17 pagesHow To Answer Stupid Job Interview Questions - LinkedInAnkur SharmaNo ratings yet
- NIT03 WAR Museurm PDFDocument78 pagesNIT03 WAR Museurm PDFDeepak SinghNo ratings yet
- Vaf PDFDocument11 pagesVaf PDFМаксим Ляшенко100% (1)
- Template For Repertoire ProposalDocument9 pagesTemplate For Repertoire ProposalAhmad SyabilNo ratings yet
- Exfoliative Respiratory Cytology (Part 1 of 2)Document15 pagesExfoliative Respiratory Cytology (Part 1 of 2)Jenn100% (2)
- Placement Exam FaqDocument2 pagesPlacement Exam FaqsglovescarsNo ratings yet
- EEE 209 Presentation 1 IntroductionDocument8 pagesEEE 209 Presentation 1 IntroductionMert YılmazNo ratings yet
- COT3 IDocument2 pagesCOT3 IKamsha Uy100% (1)
- Online Bike Parts Store and Rental SystemDocument4 pagesOnline Bike Parts Store and Rental SystemriysNo ratings yet
- 5564 Quantitative TechniquesDocument8 pages5564 Quantitative TechniquesTalat RaniNo ratings yet
- R. Molski, Polish Antitrust Law in Its Fight Against Cartels - Awaiting A BreakthroughDocument28 pagesR. Molski, Polish Antitrust Law in Its Fight Against Cartels - Awaiting A Breakthroughcsair1No ratings yet
- Particle Physics (Physics Factsheet)Document27 pagesParticle Physics (Physics Factsheet)Utsav Dhakal83% (6)
- Grade 9: Research Quiz: Citation FormatsDocument20 pagesGrade 9: Research Quiz: Citation Formatsvia macario100% (1)
- Self Incompatibility: Dr. L.K.GangwarDocument38 pagesSelf Incompatibility: Dr. L.K.GangwarSiddhant Singh100% (1)
- Powerpoint By: Mohamad Sepehri, Ph.D. Jacksonville UniversityDocument31 pagesPowerpoint By: Mohamad Sepehri, Ph.D. Jacksonville UniversityNilesh DhakeNo ratings yet
- Marketing Management AssessmentDocument5 pagesMarketing Management AssessmentMajdi SuleimanNo ratings yet
- Proof by Induction - FactorialsDocument1 pageProof by Induction - FactorialsejlflopNo ratings yet
- Pengaruh Otago Exercise Dan Gaze Stability Exercise Terhadap Keseimbangan Pada Lanjut UsiaDocument10 pagesPengaruh Otago Exercise Dan Gaze Stability Exercise Terhadap Keseimbangan Pada Lanjut UsiaBimo AnggoroNo ratings yet
- Periodic Safety Update Reports: Adel Alrwisan B.SC, M.SC, PPCDocument16 pagesPeriodic Safety Update Reports: Adel Alrwisan B.SC, M.SC, PPCHala MohamedNo ratings yet
- 1Document11 pages1Amjad PiroutiNo ratings yet