Download as pdf or txt
You might also like
- The Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionFrom EverandThe Osteoperiosteal Flap: A Simplified Approach to Alveolar Bone ReconstructionRating: 4 out of 5 stars4/5 (1)
- RSPH Level 4 Award in Haccp Management For Food ManufacturingDocument19 pagesRSPH Level 4 Award in Haccp Management For Food ManufacturingHema HemaNo ratings yet
- Play Therapy (Report Outline)Document4 pagesPlay Therapy (Report Outline)Jan Michael SuarezNo ratings yet
- Osseodensificação Com o TarcioDocument7 pagesOsseodensificação Com o Tarcioalessandra camposNo ratings yet
- Asds 06 1448Document7 pagesAsds 06 1448Joao Carlos JuniorNo ratings yet
- Edéntulo Tota Superior HíbridaDocument7 pagesEdéntulo Tota Superior HíbridaAlexis BenitesNo ratings yet
- Current Approaches To Septal Saddle Nose Reconstruction Using AutograftsDocument7 pagesCurrent Approaches To Septal Saddle Nose Reconstruction Using AutograftsRosaMinnitiNo ratings yet
- 2 Evaluation of Anatomical Considerations in The PosteriorDocument7 pages2 Evaluation of Anatomical Considerations in The PosteriorJoyce GalvezNo ratings yet
- Nasal Prosthesis - A Case ReportDocument4 pagesNasal Prosthesis - A Case ReportInternational Organization of Scientific Research (IOSR)No ratings yet
- Ab 2019Document7 pagesAb 2019Dome CárdenasNo ratings yet
- Semilunar Conchal Cartilage Graft in Saddle Nose ReconstructionDocument4 pagesSemilunar Conchal Cartilage Graft in Saddle Nose ReconstructionlucaNo ratings yet
- Maxillary Obturator Prosthesis Rehabilitation Following Maxillectomy For Ameloblastoma: A Clinical Case ReportDocument5 pagesMaxillary Obturator Prosthesis Rehabilitation Following Maxillectomy For Ameloblastoma: A Clinical Case ReportIJAR JOURNALNo ratings yet
- Adj 12563Document5 pagesAdj 12563anushiNo ratings yet
- Ângelo Et Al 2020Document5 pagesÂngelo Et Al 2020henriquetaranNo ratings yet
- Kyung 2015Document4 pagesKyung 2015mohamed elazabNo ratings yet
- Implant-Supported Nasal Prosthesis. Clinical Case Report: Prótesis Nasal Implantosoportada. Reporte de Un Caso ClínicoDocument6 pagesImplant-Supported Nasal Prosthesis. Clinical Case Report: Prótesis Nasal Implantosoportada. Reporte de Un Caso ClínicoMelina Nataly Robles AcuñaNo ratings yet
- Int Endodontic J - 2022 - Bai - Enhanced Conservation of Vital Pulp and Apical Tissues by The Application of Crown RotationDocument7 pagesInt Endodontic J - 2022 - Bai - Enhanced Conservation of Vital Pulp and Apical Tissues by The Application of Crown RotationShakeel AhmedNo ratings yet
- Lefort 2Document7 pagesLefort 2jazminhuarcaya2709No ratings yet
- Chipalia 2014 Articulocompleto PDFDocument11 pagesChipalia 2014 Articulocompleto PDFLeid ArizaNo ratings yet
- 5657 DownDocument17 pages5657 DownMai ThúyNo ratings yet
- Cirugía OralDocument7 pagesCirugía OralLenny GrauNo ratings yet
- Bone Dust and Diced Cartilage Combined With Blood Glue: A Practical Technique For Dorsum EnhancementDocument5 pagesBone Dust and Diced Cartilage Combined With Blood Glue: A Practical Technique For Dorsum EnhancementVLADIMIR RAMIREZ-BLANCOMDNo ratings yet
- Implant Rehabilitation in The Edentulous Jaw: The "All-On-4" Immediate Function ConceptDocument8 pagesImplant Rehabilitation in The Edentulous Jaw: The "All-On-4" Immediate Function ConceptAnonymous i7fNNiRqh2No ratings yet
- 1 s2.0 S1073874617300245 Main PDFDocument11 pages1 s2.0 S1073874617300245 Main PDFOrtodoncia UNAL 2020No ratings yet
- Aaid Joi D 11 00068Document8 pagesAaid Joi D 11 00068Hema SinghNo ratings yet
- Decoronation of An Ankylosed Permanent Incisor: Alveolar Ridge Preservation and Rehabilitation by An Implant Supported Porcelain CrownDocument4 pagesDecoronation of An Ankylosed Permanent Incisor: Alveolar Ridge Preservation and Rehabilitation by An Implant Supported Porcelain CrownJuan Carlos MeloNo ratings yet
- Implant Nghiêng Vs Tiêu Xương C 2Document10 pagesImplant Nghiêng Vs Tiêu Xương C 2NhatHai PhanNo ratings yet
- Review Cirugía Preprotésica. ArtículoDocument9 pagesReview Cirugía Preprotésica. ArtículoAnita Estela Batz MatulNo ratings yet
- Immediate Dentoalveolar Restoration in Compromised Sockets: Technique and Bone BiologyDocument14 pagesImmediate Dentoalveolar Restoration in Compromised Sockets: Technique and Bone BiologyMichal PerkowskiNo ratings yet
- Print 6Document5 pagesPrint 6hafidh akbarNo ratings yet
- Ren e Shu 2022Document4 pagesRen e Shu 2022henriquetaranNo ratings yet
- Depeyre Et Al 2016Document8 pagesDepeyre Et Al 2016henriquetaranNo ratings yet
- Is Flapless Implant Surgery A Viable Option in Posterior Maxilla? A ReviewDocument8 pagesIs Flapless Implant Surgery A Viable Option in Posterior Maxilla? A ReviewMr-Ton DrgNo ratings yet
- 18 TH JC - SindhuDocument8 pages18 TH JC - SindhuDadi SindhuNo ratings yet
- Gox 10 E4359Document3 pagesGox 10 E4359gbaez.88No ratings yet
- Nasal Hump Treatment With Cartilaginous Push-DownDocument46 pagesNasal Hump Treatment With Cartilaginous Push-Downdiego suescunNo ratings yet
- Subperiosteal ImplantsDocument5 pagesSubperiosteal ImplantsHélio AlvesNo ratings yet
- Esthetic and Functional Reconstruction of Large Mandibular Defects Using Free Fibula Flap and Implant-Retained Prosthetics - A Case Series With Long-Term Follow-UpDocument7 pagesEsthetic and Functional Reconstruction of Large Mandibular Defects Using Free Fibula Flap and Implant-Retained Prosthetics - A Case Series With Long-Term Follow-UppankajNo ratings yet
- The Joint Tip Graft: A Joint Support For Rim, Facet and Infratip Lobule in RhinoplastyDocument7 pagesThe Joint Tip Graft: A Joint Support For Rim, Facet and Infratip Lobule in RhinoplastyGöksel TurhalNo ratings yet
- Zufia e Sans 2022Document14 pagesZufia e Sans 2022henriquetaranNo ratings yet
- Ams 5 108Document4 pagesAms 5 108Alice EmailsNo ratings yet
- Rohner 2002Document9 pagesRohner 2002Jorge LopezNo ratings yet
- Implant-Retained Auricular Prosthesis: A Case Report: January 2010 - Vol.4Document4 pagesImplant-Retained Auricular Prosthesis: A Case Report: January 2010 - Vol.4noranNo ratings yet
- Articol PMFDocument6 pagesArticol PMFclaudia lupuNo ratings yet
- Chair-Side Fabrication of A FixedDocument7 pagesChair-Side Fabrication of A FixedKataryne Dos SantosNo ratings yet
- Immediate Teeth in Fibulas Expanded Clinical ApplDocument10 pagesImmediate Teeth in Fibulas Expanded Clinical ApplPaulo Ferreira OrtodontiaNo ratings yet
- Shetye 2017Document7 pagesShetye 2017Evgeniya KocherginaNo ratings yet
- Plastic Surgery Thesis ProtocolDocument7 pagesPlastic Surgery Thesis ProtocolPavan KumarNo ratings yet
- Pi Is 1010518215004084Document8 pagesPi Is 1010518215004084Ceza CezaaNo ratings yet
- Australian Dental Journal - 2018 - Spencer - Implant Based Rehabilitation Options For The Atrophic Edentulous JawDocument8 pagesAustralian Dental Journal - 2018 - Spencer - Implant Based Rehabilitation Options For The Atrophic Edentulous JawAswathi RaghuthamanNo ratings yet
- Mandibular Bone Block Harvesting From The Retromolar Region: A 10-Year Prospective Clinical StudyDocument10 pagesMandibular Bone Block Harvesting From The Retromolar Region: A 10-Year Prospective Clinical StudyFerenc NagyNo ratings yet
- 2005 Laster Width Distraction OsteogenesisDocument7 pages2005 Laster Width Distraction Osteogenesislisal1saNo ratings yet
- Removal Of..Document4 pagesRemoval Of..Andrea ValverdeNo ratings yet
- A Simplified Method For The Fabrication of Obturator:a Case ReportDocument4 pagesA Simplified Method For The Fabrication of Obturator:a Case ReportinventionjournalsNo ratings yet
- GraftsDocument23 pagesGraftsLinngamuNo ratings yet
- 2011 Article 60 PDFDocument4 pages2011 Article 60 PDFCamilla FrançaNo ratings yet
- RJDS Sep 2022 Article 85-94Document10 pagesRJDS Sep 2022 Article 85-94venugopal ssNo ratings yet
- Surgical Management of Giant Radicular Cyst of Maxillary Central and Lateral Incisor Followed by Apicoectomy - A Case ReportDocument10 pagesSurgical Management of Giant Radicular Cyst of Maxillary Central and Lateral Incisor Followed by Apicoectomy - A Case ReportIJAR JOURNALNo ratings yet
- 6 Dahl ApplianceDocument6 pages6 Dahl ApplianceDentist Here100% (1)
- Full Mouth Rehabilitation of Completely Edentulous Patient With Full Arch Screw-Retained Prosthesis 2017Document9 pagesFull Mouth Rehabilitation of Completely Edentulous Patient With Full Arch Screw-Retained Prosthesis 2017marwaNo ratings yet
- Горизонтальная дистракцияDocument7 pagesГоризонтальная дистракцияIrinaBorodulinaNo ratings yet
- Otoplasty Through Ventral Skin Incision and Shaping of The Antihelix by Abrasion-A Retrospective StudyDocument8 pagesOtoplasty Through Ventral Skin Incision and Shaping of The Antihelix by Abrasion-A Retrospective StudyKihyun YooNo ratings yet
- Recipe of Medical AirDocument13 pagesRecipe of Medical AirMd. Rokib ChowdhuryNo ratings yet
- Inter Journal 2Document14 pagesInter Journal 2NasmurizalNo ratings yet
- Chapter Iii: Flexibility Training Exercise: Physical Activities Towards Health and Fitness IIDocument5 pagesChapter Iii: Flexibility Training Exercise: Physical Activities Towards Health and Fitness II방민준No ratings yet
- List of WW and PTDocument4 pagesList of WW and PTKhitel Mojares VentocillaNo ratings yet
- CLP Info SheetDocument6 pagesCLP Info SheetCarolina Mateus MoreiraNo ratings yet
- Tsvieli 2019Document17 pagesTsvieli 2019ekaNo ratings yet
- At The Hospital Quick Reference Glossary PDFDocument12 pagesAt The Hospital Quick Reference Glossary PDFFaisal IqbalNo ratings yet
- Station 1 Abdominal MRCP PACES Practice Mark SheetDocument1 pageStation 1 Abdominal MRCP PACES Practice Mark SheetdoctorebrahimNo ratings yet
- What Is This Thing Called Spatial Planning - Nigel TaylorDocument17 pagesWhat Is This Thing Called Spatial Planning - Nigel TaylorFatma Rana WallaNo ratings yet
- Ethics Death and DyingDocument15 pagesEthics Death and DyingJerbs Llames100% (1)
- CPR Salbutamol+Ipratropium Neb (BRODIX PLUS) 35'sDocument2 pagesCPR Salbutamol+Ipratropium Neb (BRODIX PLUS) 35'sRacquel SolivenNo ratings yet
- Hospital: ServicesDocument60 pagesHospital: ServicesChanpreet SinghNo ratings yet
- Abutment Selection in Fixed Partial DentureDocument37 pagesAbutment Selection in Fixed Partial Dentureanmol nehaNo ratings yet
- ICN Framework of Disaster NursingDocument18 pagesICN Framework of Disaster NursingKRIZIA ANE A. SULONG100% (1)
- Benefits of Living DonationDocument1 pageBenefits of Living DonationRanga RajanNo ratings yet
- MMS-WPS Starting ProcedureDocument1 pageMMS-WPS Starting Procedurebagus918No ratings yet
- Ego Resilience ScaleDocument2 pagesEgo Resilience ScalejyoNo ratings yet
- Lifting Plan: Table of ContentDocument11 pagesLifting Plan: Table of ContentkhurramNo ratings yet
- Cystotomy 37 LDocument19 pagesCystotomy 37 LDr Anais AsimNo ratings yet
- Basic Life Support For PrintingDocument57 pagesBasic Life Support For Printingيزن عليماتNo ratings yet
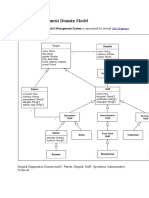
- Hospital Management Domain ModelDocument4 pagesHospital Management Domain Modelvinod kapateNo ratings yet
- الإجازات المرضية - منصة صحةDocument2 pagesالإجازات المرضية - منصة صحةShatha miNo ratings yet
- Stai GreekDocument16 pagesStai GreekBravannoyNo ratings yet
- 1656306523-ELite 580 - 4 PageDocument3 pages1656306523-ELite 580 - 4 PageJay JaniNo ratings yet
- Bullying in Social Media: An Effect Study of Cyber Bullying On The YouthDocument21 pagesBullying in Social Media: An Effect Study of Cyber Bullying On The Youthiqra urooj100% (1)
- EPA Consensus Project Paper Accuracy of Photogrammetry Devices Intraoral Scanners and Conventional Techniques For The Full Arch Implant Impressions A Systematic ReviewDocument12 pagesEPA Consensus Project Paper Accuracy of Photogrammetry Devices Intraoral Scanners and Conventional Techniques For The Full Arch Implant Impressions A Systematic Reviewcasto.carpetasmiaNo ratings yet
- Edu 422 NotesDocument13 pagesEdu 422 NotesAbdulazeez AishatNo ratings yet
- Appellant SDocument8 pagesAppellant SVEDASHREENo ratings yet