Download as pdf or txt
You might also like
- 40567a Microsoft Excel Associate 2019 EbookDocument508 pages40567a Microsoft Excel Associate 2019 EbookLuis Fernando Herrera Sandoval100% (3)
- PI-08-195 A R4 AIS Transponder System TroubleShootingDocument20 pagesPI-08-195 A R4 AIS Transponder System TroubleShootingTaufiq Omar Hasan100% (1)
- Temple Run PDFDocument73 pagesTemple Run PDFM. Saleem100% (1)
- Vertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenDocument11 pagesVertebral Fracture Risk (VFR) Score For Fracture Prediction in Postmenopausal WomenAdhiatma DotNo ratings yet
- 1471 2318 13 71Document9 pages1471 2318 13 71LucasNo ratings yet
- Maturitas: SciencedirectDocument6 pagesMaturitas: Sciencedirectaeroforce20No ratings yet
- Melton 1998Document9 pagesMelton 1998Jossie AcuñaNo ratings yet
- F. Lapi, M. Simonetti, R. Michieli, A. Pasqua, M.L. Brandi, B. Frediani, C. Cricelli, G. MazzagliaDocument6 pagesF. Lapi, M. Simonetti, R. Michieli, A. Pasqua, M.L. Brandi, B. Frediani, C. Cricelli, G. Mazzagliafirdha afghaniNo ratings yet
- Interpreting A DXA Scan in Clinical Practice: Rheumatology Department, Military Hospital Mohammed V, Rabat, MoroccoDocument17 pagesInterpreting A DXA Scan in Clinical Practice: Rheumatology Department, Military Hospital Mohammed V, Rabat, MoroccoJaita SawettachaiNo ratings yet
- Relación Entre Fuerza Prensil y Contenido Mineral ÓseoDocument11 pagesRelación Entre Fuerza Prensil y Contenido Mineral ÓseoFrancisco Mancilla LobosNo ratings yet
- JCSM 12477Document14 pagesJCSM 12477Oscar AlzateNo ratings yet
- Effects of Weight-Bearing Exercise On Bone Health in Girls: A Meta-AnalysisDocument18 pagesEffects of Weight-Bearing Exercise On Bone Health in Girls: A Meta-AnalysiskalikNo ratings yet
- Association Between Knee Osteoarthritis and Volumetric Bone Mineral DensityDocument14 pagesAssociation Between Knee Osteoarthritis and Volumetric Bone Mineral Densitytranminhtri21062001No ratings yet
- OsteoporosisDocument6 pagesOsteoporosisGheavita Chandra DewiNo ratings yet
- Research Article: Potential Extensions of The US FRAX AlgorithmDocument8 pagesResearch Article: Potential Extensions of The US FRAX AlgorithmAnonymous V5l8nmcSxbNo ratings yet
- Age Ageing-2015-Guadalupe-Grau-790-5Document6 pagesAge Ageing-2015-Guadalupe-Grau-790-5dariorguezNo ratings yet
- Prediction of Hip and Hand Fractures in Older Persons With or Without A Diagnosis of PeriodontitisDocument5 pagesPrediction of Hip and Hand Fractures in Older Persons With or Without A Diagnosis of PeriodontitismarishaNo ratings yet
- A Meta-Analysis of Breastfeeding and Osteoporotic Fracture Risk in The FemalesDocument5 pagesA Meta-Analysis of Breastfeeding and Osteoporotic Fracture Risk in The Femalesanisa rizkyNo ratings yet
- Cross Sectional Study-Bone Mineral Density in Athletes of Different Discipline - TOSSJ-3-129Document5 pagesCross Sectional Study-Bone Mineral Density in Athletes of Different Discipline - TOSSJ-3-129SPN CDYNo ratings yet
- Specker 2015 - Does Exercise Influence Pediatric Bone - A Systematic ReviewDocument15 pagesSpecker 2015 - Does Exercise Influence Pediatric Bone - A Systematic ReviewStavros LitsosNo ratings yet
- (2023) Effects of Running On The Development of Knee OsteoarthritisDocument6 pages(2023) Effects of Running On The Development of Knee Osteoarthritiscalixto1995No ratings yet
- The Challenges of Diagnosing Osteoporosis - and The Limitations of Currently Available - ToolsDocument13 pagesThe Challenges of Diagnosing Osteoporosis - and The Limitations of Currently Available - ToolsJevon JavierNo ratings yet
- Accepted Manuscript: Corresponding AuthorDocument38 pagesAccepted Manuscript: Corresponding AuthorAna Souza LimaNo ratings yet
- Osteoporosis Thesis StatementDocument7 pagesOsteoporosis Thesis StatementJeff Nelson100% (2)
- Fractura de TobilloDocument10 pagesFractura de TobilloWendy Lorely Téllez HernándezNo ratings yet
- Correlation Between Metabolic Syndrome and Knee Osteoarthritis: Data From The Korean National Health and Nutrition Examination Survey (Knhanes)Document8 pagesCorrelation Between Metabolic Syndrome and Knee Osteoarthritis: Data From The Korean National Health and Nutrition Examination Survey (Knhanes)Agatha GeraldyneNo ratings yet
- Osteoporosis in Ankylosing Spondylitis - Prevalence, Risk Factors and Methods of AssessmentDocument12 pagesOsteoporosis in Ankylosing Spondylitis - Prevalence, Risk Factors and Methods of AssessmentCODREANU ADANo ratings yet
- Ajmg 185 1023Document10 pagesAjmg 185 1023Luis Briones Lau.LiNo ratings yet
- 2019 Article 2449Document10 pages2019 Article 2449contoisaNo ratings yet
- Kamonseki 2018Document31 pagesKamonseki 2018nathan.lindao25No ratings yet
- Santana 2019 - de Santana - Brasil - VAT y MortalidadDocument11 pagesSantana 2019 - de Santana - Brasil - VAT y Mortalidad2192036250No ratings yet
- International Journal of Health Sciences and Research: Osteoporosis-Do We Need To Think Beyond Bone Mineral Density?Document5 pagesInternational Journal of Health Sciences and Research: Osteoporosis-Do We Need To Think Beyond Bone Mineral Density?Ahmad Ghozi Al AkhmarNo ratings yet
- Risk Factors For Knee Replacement Due To Primary Osteoarthritis, A Population Based, Prospective Cohort Study of 315,495 IndividualsDocument11 pagesRisk Factors For Knee Replacement Due To Primary Osteoarthritis, A Population Based, Prospective Cohort Study of 315,495 Individualsnur hasanahNo ratings yet
- Efectos A Largo Plazo de Anorexia y Baja Masa OseaDocument6 pagesEfectos A Largo Plazo de Anorexia y Baja Masa OsealeticiadelfinofotosNo ratings yet
- Fragility Fracture Discriminative Ability of Radius Quantitative Ultrasound: A Systematic Review and Meta-AnalysisDocument16 pagesFragility Fracture Discriminative Ability of Radius Quantitative Ultrasound: A Systematic Review and Meta-AnalysisTarib TrifaNo ratings yet
- BackgroundDocument15 pagesBackgroundcony.juulNo ratings yet
- KJFM 34 281Document8 pagesKJFM 34 281Dian AuliaNo ratings yet
- A Meta-Analysis of Breastfeeding and Osteoporotic Fracture Risk in The FemalesDocument9 pagesA Meta-Analysis of Breastfeeding and Osteoporotic Fracture Risk in The FemalesIndah RahmaaNo ratings yet
- PalmerDocument11 pagesPalmeryuryNo ratings yet
- Screening For Osteoporosis - UpToDateDocument22 pagesScreening For Osteoporosis - UpToDatesindy suarezNo ratings yet
- Ymj 59 317Document8 pagesYmj 59 317ItaloLozanoPalominoNo ratings yet
- Review: DXA Scanning in Clinical PracticeDocument13 pagesReview: DXA Scanning in Clinical PracticeDinesh MudaliarNo ratings yet
- Musculoskeletal ComplaintsDocument18 pagesMusculoskeletal ComplaintsLucila BernasconiNo ratings yet
- Kanis Ja 2002Document8 pagesKanis Ja 2002M MNo ratings yet
- Aging V12i24 202140Document10 pagesAging V12i24 202140Ismail ZeroualNo ratings yet
- Weight Cycling and Knee Joint DegenerationDocument20 pagesWeight Cycling and Knee Joint DegenerationТати ГалаNo ratings yet
- Diagnosis of Osteoporosis and Assessment of Fracture Risk John A Kanis 2002Document8 pagesDiagnosis of Osteoporosis and Assessment of Fracture Risk John A Kanis 2002Jossie AcuñaNo ratings yet
- Practice Sub 1Document10 pagesPractice Sub 1affeishaNo ratings yet
- Prevalence of Work Related Musculoskeletal Disorders in Early Onset Scoliosis SurgeonsDocument10 pagesPrevalence of Work Related Musculoskeletal Disorders in Early Onset Scoliosis SurgeonsAthenaeum Scientific PublishersNo ratings yet
- García Hermoso2018Document19 pagesGarcía Hermoso2018Sam Steven Hernandez JañaNo ratings yet
- Gomescampos Et Al 2019Document9 pagesGomescampos Et Al 2019Filipe UFRGSNo ratings yet
- Effects of High-Impact Exercise On Ultrasonic and Biochemical Indices of Skeletal Status: A Prospective Study in Young Male GymnastsDocument9 pagesEffects of High-Impact Exercise On Ultrasonic and Biochemical Indices of Skeletal Status: A Prospective Study in Young Male GymnastsCláudio MeirelesNo ratings yet
- Digital Panoramic Radiography As A Useful Tool For Detection of Bone Loss: A Comparative StudyDocument7 pagesDigital Panoramic Radiography As A Useful Tool For Detection of Bone Loss: A Comparative StudyDorin N. GheorgheNo ratings yet
- 1 s2.0 S1466853X24000257Document6 pages1 s2.0 S1466853X24000257Verónica Obando ToroNo ratings yet
- ARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsDocument5 pagesARTICLEMuscle Mass Measured Using Bioelectrical Impedanceanalysis, Calf Circumference and Grip Strength in OlderadultsPPDS Rehab Medik UnhasNo ratings yet
- Sarcopenia: ReviewDocument6 pagesSarcopenia: ReviewmariaespaNo ratings yet
- Hartmann 2009Document10 pagesHartmann 2009Douglas GrigolettoNo ratings yet
- The Optimal Cut-Points For Weight and Non-Weight Quantitative Ultrasound of The Calcaneus To Screen Osteoporosis in Postmenopausal WomenDocument8 pagesThe Optimal Cut-Points For Weight and Non-Weight Quantitative Ultrasound of The Calcaneus To Screen Osteoporosis in Postmenopausal WomensucilestariNo ratings yet
- Bone Stress Injury Middle Age RunnersDocument28 pagesBone Stress Injury Middle Age RunnersAnggia PNo ratings yet
- JCM 10 00522 v2Document12 pagesJCM 10 00522 v2Setiaty PandiaNo ratings yet
- JJBMRDocument9 pagesJJBMRDeby AnditaNo ratings yet
- Could Obesity Be Considered As Risk Factor For NonDocument9 pagesCould Obesity Be Considered As Risk Factor For NontheaNo ratings yet
- Hubungan Post Anesthesia Shivering DenganDocument6 pagesHubungan Post Anesthesia Shivering DenganGio VandaNo ratings yet
- Perioperative Thermoregulation and Heat BalanceDocument10 pagesPerioperative Thermoregulation and Heat BalanceGio VandaNo ratings yet
- The Prehospital Management of Hypothermia - An Up-To-DateDocument16 pagesThe Prehospital Management of Hypothermia - An Up-To-DateGio VandaNo ratings yet
- Gio 28 InggrissDocument17 pagesGio 28 InggrissGio VandaNo ratings yet
- Shivering Thermogenesis in Humans Origin, Contribution and MetabolicDocument10 pagesShivering Thermogenesis in Humans Origin, Contribution and MetabolicGio VandaNo ratings yet
- Gio 26 InggrisDocument33 pagesGio 26 InggrisGio VandaNo ratings yet
- Realignment Surgery For Malunited Ankle Fracture: Clinical ArticleDocument5 pagesRealignment Surgery For Malunited Ankle Fracture: Clinical ArticleGio VandaNo ratings yet
- Pediatric Anesthesiology Fellows' Perception of Quality of Attending Supervision and Medical ErrorsDocument5 pagesPediatric Anesthesiology Fellows' Perception of Quality of Attending Supervision and Medical ErrorsGio VandaNo ratings yet
- 10 1111@jonm 12776Document7 pages10 1111@jonm 12776Gio VandaNo ratings yet
- 1 s2.0 S1268773120301703 MainDocument7 pages1 s2.0 S1268773120301703 MainGio VandaNo ratings yet
- Giovanda 23Document10 pagesGiovanda 23Gio VandaNo ratings yet
- The Effects of Anesthetic Technique On Postoperative Opioid Consumption in Ankle Fracture SurgeryDocument16 pagesThe Effects of Anesthetic Technique On Postoperative Opioid Consumption in Ankle Fracture SurgeryGio VandaNo ratings yet
- Aircraft Design Project Designing A Competitor Fighter AircraftDocument45 pagesAircraft Design Project Designing A Competitor Fighter AircraftKarthick. GNo ratings yet
- A Complete Manual On Ornamental Fish Culture: January 2013Document222 pagesA Complete Manual On Ornamental Fish Culture: January 2013Carlos MorenoNo ratings yet
- Oracle Golden Gate 11g SyllabusDocument4 pagesOracle Golden Gate 11g SyllabusksknrindianNo ratings yet
- Phpwyt 7 NaDocument170 pagesPhpwyt 7 Na0176rahulsharmaNo ratings yet
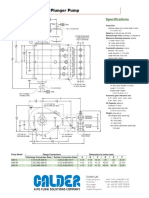
- 300Q-5 Quintuplex Plunger PumpDocument2 pages300Q-5 Quintuplex Plunger PumpJuanNo ratings yet
- Examiners' Commentaries 2020: AC2097 Management AccountingDocument30 pagesExaminers' Commentaries 2020: AC2097 Management Accountingduong duongNo ratings yet
- Aspire 7750z PDFDocument274 pagesAspire 7750z PDFToni011973No ratings yet
- Catalogo de Bandas Atv - Vehiculos Todo Terreno-: Pagina MarcaDocument28 pagesCatalogo de Bandas Atv - Vehiculos Todo Terreno-: Pagina MarcaGarcia Leo DiegoNo ratings yet
- Chapter #2 (Part 1)Document17 pagesChapter #2 (Part 1)Consiko leeNo ratings yet
- Carpio-Morales v. CA Case DigestDocument2 pagesCarpio-Morales v. CA Case DigestLIERANo ratings yet
- Government Gazette OfficeDocument2 pagesGovernment Gazette OfficeVez HindjouNo ratings yet
- Competitiveness of Beekeeping in MalaysiaDocument70 pagesCompetitiveness of Beekeeping in MalaysiaRobin WongNo ratings yet
- Mea12 PDFDocument59 pagesMea12 PDFSriNo ratings yet
- Qdoc - Tips - Volvo Penta Installation ManualDocument53 pagesQdoc - Tips - Volvo Penta Installation ManualJorge GomezNo ratings yet
- Final Population Age Structure, Sex Composition and Rural - Urban CompositionDocument6 pagesFinal Population Age Structure, Sex Composition and Rural - Urban CompositionMaraQuezNo ratings yet
- 3 Star Hotel - BaalbeckDocument19 pages3 Star Hotel - BaalbeckAkm EngidaNo ratings yet
- Laws4112 (2014) Exam Notes (Uq)Document132 pagesLaws4112 (2014) Exam Notes (Uq)tc_bassNo ratings yet
- Percona MySQL Support Services For Better Application PerformanceDocument6 pagesPercona MySQL Support Services For Better Application PerformanceGhanshyam BaviskarNo ratings yet
- PHP Handout PFDocument18 pagesPHP Handout PFsuha9734100% (1)
- Manual KYK 30000Document20 pagesManual KYK 30000Benny ScorpyoNo ratings yet
- B 8.4 Student Activity: Using GreenhousesDocument3 pagesB 8.4 Student Activity: Using GreenhousesCK BNo ratings yet
- Reading and Writing Via CodeDocument7 pagesReading and Writing Via CodedaviqueirozdemedeirosNo ratings yet
- Humanbe, Self - Assessment Motivation SelfDocument5 pagesHumanbe, Self - Assessment Motivation SelfHans LeeNo ratings yet
- Nagothane Manufacturing Division Summer Internship ReportDocument5 pagesNagothane Manufacturing Division Summer Internship ReportMrudu PadteNo ratings yet
- Falcon 7X CommunicationsDocument105 pagesFalcon 7X Communicationsjunmech-1No ratings yet
- Gr10 Math P1 Nov 2022Document20 pagesGr10 Math P1 Nov 2022samcuthbert4No ratings yet
- BIO218 Test 10Document5 pagesBIO218 Test 10Egi SugianaNo ratings yet