Download as pdf or txt
You might also like
- Luis Barragán, de Antonio RiggenDocument83 pagesLuis Barragán, de Antonio RiggenJorge Octavio Ocaranza VelascoNo ratings yet
- 50 Strategies For Differentiated InstructionDocument19 pages50 Strategies For Differentiated InstructionMisael AmoraNo ratings yet
- Talking Fashion: Pierre Cardin Interviewed by Jan KedvesDocument5 pagesTalking Fashion: Pierre Cardin Interviewed by Jan KedvesJanKedves100% (1)
- Virus Respiratorio SincicialDocument10 pagesVirus Respiratorio SincicialNicole Castillo AguirreNo ratings yet
- Pediatrics in Review 2014 Piedimonte 519 30Document15 pagesPediatrics in Review 2014 Piedimonte 519 30Felipe CeaNo ratings yet
- Etm 20 6 9350 PDFDocument8 pagesEtm 20 6 9350 PDFJessica Asitimbay ZuritaNo ratings yet
- Respiratory Syncytial Virus Infection and Bronchiolitis: Practice GapsDocument14 pagesRespiratory Syncytial Virus Infection and Bronchiolitis: Practice GapsAnge CerónNo ratings yet
- Drysdale 2017Document6 pagesDrysdale 2017ltorresacostaNo ratings yet
- Respiratory SyncytialDocument32 pagesRespiratory Syncytialtummalapalli venkateswara rao100% (2)
- RSVDocument8 pagesRSVilyas9558No ratings yet
- DX VirologicoDocument15 pagesDX VirologicoCarlos Avelino Juárez SantiagoNo ratings yet
- State of The Art: Eliane Roseli Barreira, Alexander Roberto Precioso, Albert BoussoDocument6 pagesState of The Art: Eliane Roseli Barreira, Alexander Roberto Precioso, Albert BoussoPaola MoraNo ratings yet
- Jurnal OkeDocument8 pagesJurnal OkeAuliaRahmanNo ratings yet
- Genetic Susceptibility To Respiratory Syncytial Virus Bronchiolitis Is Predominantly Associated With Innate Immune GenesDocument9 pagesGenetic Susceptibility To Respiratory Syncytial Virus Bronchiolitis Is Predominantly Associated With Innate Immune GenesNarjes Sharif AskariNo ratings yet
- Asmainf AmamDocument10 pagesAsmainf AmamgabibarbozaNo ratings yet
- BQL RX ConsDocument3 pagesBQL RX ConsAwe Angga WirahmadiNo ratings yet
- Respiratory Syncytial VirusDocument16 pagesRespiratory Syncytial VirusAradhanaRamchandaniNo ratings yet
- Fatal Pulmonary Infection With Respiratory SyncytiDocument5 pagesFatal Pulmonary Infection With Respiratory Syncyti21701101046 Devi NavilaNo ratings yet
- Brief: Human Metapneumovirus InfectionDocument4 pagesBrief: Human Metapneumovirus InfectionmedicotayacajaNo ratings yet
- Role of Viruses in AsthmaDocument14 pagesRole of Viruses in AsthmaForensik UMINo ratings yet
- Cold Weather VirusesDocument13 pagesCold Weather VirusesAndreeaAlexandruNo ratings yet
- Judicious Use of Antibiotics: A Guide For Oregon CliniciansDocument32 pagesJudicious Use of Antibiotics: A Guide For Oregon CliniciansRiyan SaputraNo ratings yet
- Upper Respiratory Tract InfectionDocument10 pagesUpper Respiratory Tract InfectionBrandon McgeeNo ratings yet
- Towards Personalized Medicine in Bronchiolitis: Word Count: 972Document7 pagesTowards Personalized Medicine in Bronchiolitis: Word Count: 972Pediatría grupoNo ratings yet
- Nursing-Management A Respriotry Syncytial Bronchiolitis PDFDocument7 pagesNursing-Management A Respriotry Syncytial Bronchiolitis PDFAdarsh MuniNo ratings yet
- Oxygen Therapy of Very Low Birth Weight Neonates With PneumoniaDocument5 pagesOxygen Therapy of Very Low Birth Weight Neonates With PneumoniaYohana TrissyaNo ratings yet
- Coxsackie VirusDocument10 pagesCoxsackie Virusjyothsna yarraNo ratings yet
- Live Attenuated Human Rotavirus Vaccine, Rotarix™: David I. Bernstein, MD, MADocument7 pagesLive Attenuated Human Rotavirus Vaccine, Rotarix™: David I. Bernstein, MD, MACagar Irwin TaufanNo ratings yet
- Probiotics in Respiratory Virus Infections: ReviewDocument14 pagesProbiotics in Respiratory Virus Infections: ReviewErik Jaya GunawanNo ratings yet
- New MOC ResourcesDocument22 pagesNew MOC ResourcesYidnekachew Girma AssefaNo ratings yet
- Crup 3Document22 pagesCrup 3Wilber Martin BaltodanoNo ratings yet
- Paramyxoviruses Engl BriefDocument138 pagesParamyxoviruses Engl BriefOnofrei MariaNo ratings yet
- Some Immunological Parameters of Viral Pediatric PneumoniaDocument8 pagesSome Immunological Parameters of Viral Pediatric PneumoniaTJPRC PublicationsNo ratings yet
- Bronchiolitis EtiologyDocument6 pagesBronchiolitis EtiologyRonNo ratings yet
- Coronavirus Infections and Immune ResponsesDocument33 pagesCoronavirus Infections and Immune ResponsesBasilio Papuico RomeroNo ratings yet
- Management of Acute Respiratory Diseases PDFDocument21 pagesManagement of Acute Respiratory Diseases PDFFernandoXavierNo ratings yet
- Accepted Manuscript: Paediatric Respiratory ReviewsDocument32 pagesAccepted Manuscript: Paediatric Respiratory ReviewslaurentiaNo ratings yet
- Contribution of Dendritic Cells in Protective ImmuDocument19 pagesContribution of Dendritic Cells in Protective ImmuJuanmaSousaNo ratings yet
- Diagnosis and treatment of various types of coronavirus pneumonia of Sars disease and respiratory infectious diseases, and research on the source of infection of animal coronavirus pneumonia (Fang Ruida) Davis. KDocument39 pagesDiagnosis and treatment of various types of coronavirus pneumonia of Sars disease and respiratory infectious diseases, and research on the source of infection of animal coronavirus pneumonia (Fang Ruida) Davis. Kweld AdonisNo ratings yet
- Frequency of Respiratory Virus-Associated Infectio-1Document13 pagesFrequency of Respiratory Virus-Associated Infectio-1neumopediatriainerNo ratings yet
- Tesis VSR y RinovirusDocument11 pagesTesis VSR y RinovirusMaría Nurys Acevedo CerchiaroNo ratings yet
- Nasopharyngeal Polymicrobial Colonization During Health, Viral Upper Respiratory Infection and Upper Respiratory Bacterial InfectionDocument9 pagesNasopharyngeal Polymicrobial Colonization During Health, Viral Upper Respiratory Infection and Upper Respiratory Bacterial InfectionAmanda PutraNo ratings yet
- (2011, Rothman AL) Immunity To Dengue Virus - A Tale of Original Antigenic Sin and Tropical Cytokine StormsDocument12 pages(2011, Rothman AL) Immunity To Dengue Virus - A Tale of Original Antigenic Sin and Tropical Cytokine StormsRebeca de PaivaNo ratings yet
- RSV AsthmaDocument10 pagesRSV AsthmaGhaisania AthiraNo ratings yet
- Recurrent Respiratory Papillomatosis by HPV: Review of The Literature and Update On The Use of CidofovirDocument7 pagesRecurrent Respiratory Papillomatosis by HPV: Review of The Literature and Update On The Use of CidofovirListya ParamitaNo ratings yet
- Respiratory Viruses, Eosinophilia and Their Roles in Childhood AsthmaDocument11 pagesRespiratory Viruses, Eosinophilia and Their Roles in Childhood AsthmaeddcitoNo ratings yet
- RSV Presentation ChibuezeDocument13 pagesRSV Presentation ChibuezeChibueze AfugbuomNo ratings yet
- The Relationship Between Respiratory Syncytial Virus and AsthmaDocument10 pagesThe Relationship Between Respiratory Syncytial Virus and AsthmaKessi VikaneswariNo ratings yet
- Aspergillosis: Epidemiology, Diagnosis, and TreatmentDocument20 pagesAspergillosis: Epidemiology, Diagnosis, and TreatmentsilviaNo ratings yet
- Acute Otitis Media: EtiologyDocument4 pagesAcute Otitis Media: EtiologyMahir FikaNo ratings yet
- PIIS0140673610613803Document9 pagesPIIS0140673610613803arga setyo adjiNo ratings yet
- Recurrent Infections in FQDocument12 pagesRecurrent Infections in FQraul floresNo ratings yet
- Practice Essentials: View Media GalleryDocument22 pagesPractice Essentials: View Media GalleryAza Patullah ZaiNo ratings yet
- Microbioma y OtorrinoDocument19 pagesMicrobioma y Otorrinodayenu barraNo ratings yet
- J Infect Dis.-2016-Dengue Vaccine The Need, The Challenges, and ProgressDocument3 pagesJ Infect Dis.-2016-Dengue Vaccine The Need, The Challenges, and ProgressRaja Ahmad Rusdan MusyawirNo ratings yet
- Early Human Development: A. Nicolai, M. Ferrara, C. Schiavariello, F. Gentile, M.E. Grande, C. Alessandroni, F. MidullaDocument5 pagesEarly Human Development: A. Nicolai, M. Ferrara, C. Schiavariello, F. Gentile, M.E. Grande, C. Alessandroni, F. MidullalalaNo ratings yet
- Influenza Resp Viruses - 2023 - Colosia - Systematic Literature Review of The Signs and Symptoms of Respiratory Syncytial-1Document12 pagesInfluenza Resp Viruses - 2023 - Colosia - Systematic Literature Review of The Signs and Symptoms of Respiratory Syncytial-1AGUS DE COLSANo ratings yet
- Growth Chest InfectionsDocument18 pagesGrowth Chest InfectionsjibiannieNo ratings yet
- Research ArticleDocument17 pagesResearch ArticleNatanael KindangenNo ratings yet
- Microbial Diseases of The Respiratory System: Pertussis (Whooping Cough) PathogenesisDocument15 pagesMicrobial Diseases of The Respiratory System: Pertussis (Whooping Cough) PathogenesisCharlene SibugNo ratings yet
- Congenital and Neonatal Pneumonia PAEDIATRIC RESPIRATORY REVIEWS (2007) 8, 195-203 Michael D. NissenDocument9 pagesCongenital and Neonatal Pneumonia PAEDIATRIC RESPIRATORY REVIEWS (2007) 8, 195-203 Michael D. Nissenroggers72No ratings yet
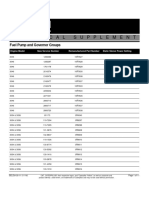
- FuelPump&GovernorGroups SELD0135 11Document11 pagesFuelPump&GovernorGroups SELD0135 11narit00007No ratings yet
- Combined Heating, Cooling & Power HandbookDocument10 pagesCombined Heating, Cooling & Power HandbookFREDIELABRADORNo ratings yet
- Purposive CommunicationDocument15 pagesPurposive CommunicationJm SalvaniaNo ratings yet
- ThesisDocument13 pagesThesiszavia_02No ratings yet
- Covert Extinction TherapyDocument6 pagesCovert Extinction TherapyAnet Augustine AnetNo ratings yet
- Greenhouse Manual2Document106 pagesGreenhouse Manual2Amit ShresthaNo ratings yet
- DB (04.2013) HiromiDocument7 pagesDB (04.2013) HiromiLew Quzmic Baltiysky75% (4)
- Nâng Cao 1 - 1 BảnDocument4 pagesNâng Cao 1 - 1 BảnThu TàiNo ratings yet
- Clone 123C3: Monoclonal Mouse Anti-Human CD56 Code M7304Document3 pagesClone 123C3: Monoclonal Mouse Anti-Human CD56 Code M7304Jaimier CajandabNo ratings yet
- Aecc 1Document1 pageAecc 1gdcenr recordsNo ratings yet
- Kyrgyzstan. ReportDocument27 pagesKyrgyzstan. Report200211555No ratings yet
- A Project Study On "BANKING AT HDFC BANK LTD.": MBA in Banking (Finance)Document99 pagesA Project Study On "BANKING AT HDFC BANK LTD.": MBA in Banking (Finance)Hitesh kumar jenaNo ratings yet
- Manual TreadDocument3 pagesManual Treadمدینة سرجيكل وہاڑیNo ratings yet
- Opera Omnia Desiderii Erasmi 1.1Document704 pagesOpera Omnia Desiderii Erasmi 1.1Professore2100% (1)
- FILM TREATMENT PE-Revised-11.30.20Document28 pagesFILM TREATMENT PE-Revised-11.30.20ArpoxonNo ratings yet
- HS Committee 64th Session - Amendments To HS Explanatory NotesDocument5 pagesHS Committee 64th Session - Amendments To HS Explanatory NotesChiNo ratings yet
- 419 WK 9Document23 pages419 WK 9nhmae gcabNo ratings yet
- Dr. Henry Petroski: Morning Lecture NotesDocument5 pagesDr. Henry Petroski: Morning Lecture Notesapi-299647486No ratings yet
- Rodriguez Vs GellaDocument33 pagesRodriguez Vs GellaRozaiineNo ratings yet
- DeputationDocument8 pagesDeputationAnand MauryaNo ratings yet
- High Court of Judicature at Allahabad: Case Status - CRIMINAL MISC. BAIL APPLICATION (BAIL) - (23700/2022)Document2 pagesHigh Court of Judicature at Allahabad: Case Status - CRIMINAL MISC. BAIL APPLICATION (BAIL) - (23700/2022)Ritesh SinghNo ratings yet
- Apbush DBQDocument2 pagesApbush DBQMaria Ines Carrillo100% (1)
- Ajava 6C 2160707 PDFDocument4 pagesAjava 6C 2160707 PDFanon4819No ratings yet
- Document 337737.1Document3 pagesDocument 337737.1elcaso34No ratings yet
- Oracle Switch ES1-24 Configuration GuideDocument88 pagesOracle Switch ES1-24 Configuration GuideNoe HernadezNo ratings yet
- Crecimiento Bajo en Carbono - Carbon-Disclosure-Project-2011Document80 pagesCrecimiento Bajo en Carbono - Carbon-Disclosure-Project-2011Alan Cereceda EscalonaNo ratings yet
- The Oriental Insurance Company LimitedDocument3 pagesThe Oriental Insurance Company Limitedrajeevjayan18No ratings yet