Download as pdf or txt
You might also like
- E 1756 - 08 (2015)Document3 pagesE 1756 - 08 (2015)Eric Gozzer100% (1)
- Best Final Year Civil Engineering Student Projects - Thesis123 PDFDocument3 pagesBest Final Year Civil Engineering Student Projects - Thesis123 PDFAlisa Jane Tuboro80% (15)
- Respiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesFrom EverandRespiratory Care Review: An Intense Look at Respiratory Care Through Case StudiesNo ratings yet
- BKM Z60 80 B III Service Manual PDFDocument54 pagesBKM Z60 80 B III Service Manual PDFKelly VillamilNo ratings yet
- JAD - 2017 - 2111 - Revision 1 - V0Document46 pagesJAD - 2017 - 2111 - Revision 1 - V0PedroNo ratings yet
- JAD 9656 Edit ReportDocument9 pagesJAD 9656 Edit ReportPedroNo ratings yet
- Gordon Et Al., (2019) Efecct of Pulmonary Rehabilitation On Symptoms of Anxiety and Depression in Chronic Obstructive Pulmonary DiseaseDocument12 pagesGordon Et Al., (2019) Efecct of Pulmonary Rehabilitation On Symptoms of Anxiety and Depression in Chronic Obstructive Pulmonary DiseaseAna Flávia SordiNo ratings yet
- Dec14 16 PDFDocument7 pagesDec14 16 PDFijasrjournalNo ratings yet
- EXCELENTEDocument7 pagesEXCELENTEJorge GámezNo ratings yet
- Anxiety and Depression in Patients With Chronic Obstructive Pulmonary Disease (COPD) - A ReviewDocument6 pagesAnxiety and Depression in Patients With Chronic Obstructive Pulmonary Disease (COPD) - A ReviewArja' WaasNo ratings yet
- Farvervesteergard-Mindfulness-based Cognitive Therapy inDocument11 pagesFarvervesteergard-Mindfulness-based Cognitive Therapy injuan pabloNo ratings yet
- Respiratory ResearchDocument32 pagesRespiratory ResearchNuno DuarteNo ratings yet
- 2022 Article 2121Document8 pages2022 Article 2121adytiaevans12No ratings yet
- Cardiometabolic Risk in Patients With First Episode of - 2022 - Neuroscience ApDocument1 pageCardiometabolic Risk in Patients With First Episode of - 2022 - Neuroscience AploloasbNo ratings yet
- Are Respiratory Abnormalities Specific For Panic Disorder? A Meta-AnalysisDocument8 pagesAre Respiratory Abnormalities Specific For Panic Disorder? A Meta-AnalysischickiecoopNo ratings yet
- Rschgate Psychoisi TX W TherDocument11 pagesRschgate Psychoisi TX W Therscribd4kmhNo ratings yet
- CBT IsbDocument12 pagesCBT IsbAlex DuranNo ratings yet
- Evaluation of Frequency and Severity of Anxiety and Mood Disorders Among Patients With Graves' DiseaseDocument5 pagesEvaluation of Frequency and Severity of Anxiety and Mood Disorders Among Patients With Graves' DiseaseBaru Chandrasekhar RaoNo ratings yet
- 00526-2021 FullDocument10 pages00526-2021 FullFaeza HasnanNo ratings yet
- Appi Ajp 162 12 2220Document13 pagesAppi Ajp 162 12 2220LosineKrishnaNo ratings yet
- Depression and Chronic InflamationDocument12 pagesDepression and Chronic InflamationVlad VochituNo ratings yet
- Heart Rate Variability For Treatment Response Between Patients With Major Depressive Disorder Versus Panic Disorder A 12-Week Follow-Up StudyDocument9 pagesHeart Rate Variability For Treatment Response Between Patients With Major Depressive Disorder Versus Panic Disorder A 12-Week Follow-Up StudyEden DingNo ratings yet
- DFHDF DFJKJK DFDocument8 pagesDFHDF DFJKJK DFAndrés Araneda VásquezNo ratings yet
- The Journal of Alternative and Complementary MedicineDocument7 pagesThe Journal of Alternative and Complementary Medicineharshadpardeshi45No ratings yet
- How To Measure Sustained Psychic Transformations I - 221027 - 134246Document31 pagesHow To Measure Sustained Psychic Transformations I - 221027 - 134246Mariana PanteceNo ratings yet
- Treating Depression With The Evidence-Based Psychotherapies: A Critique of The EvidenceDocument8 pagesTreating Depression With The Evidence-Based Psychotherapies: A Critique of The Evidencechica_asNo ratings yet
- University of Bohol Maria Clara Street, Tagbilaran City Bohol-6300 College of Pharmacy First Term 2 Semester A.Y 2020-2021Document19 pagesUniversity of Bohol Maria Clara Street, Tagbilaran City Bohol-6300 College of Pharmacy First Term 2 Semester A.Y 2020-2021MA. JANNELLE P. RESANENo ratings yet
- Bipolar Disorder: Open Access: Clinical Utility of The Predominant Polarity in Bipolar Disorder PatientsDocument3 pagesBipolar Disorder: Open Access: Clinical Utility of The Predominant Polarity in Bipolar Disorder PatientsrischaNo ratings yet
- PubMed - Yoga Menurunkan Sistol Dan Diastol Pada PrehipertensiDocument10 pagesPubMed - Yoga Menurunkan Sistol Dan Diastol Pada PrehipertensiHanifah Sarah N.l.aNo ratings yet
- Efficacy of Bright Light Therapy in Bipolar Depression - Kupeli 2018Document22 pagesEfficacy of Bright Light Therapy in Bipolar Depression - Kupeli 2018Julio JuarezNo ratings yet
- DDocument18 pagesDsilvia donaNo ratings yet
- 10 1016@j Msard 2017 07 008Document15 pages10 1016@j Msard 2017 07 008loloasbNo ratings yet
- Parkinson TerapiaDocument13 pagesParkinson TerapiaIsabela FiuzaNo ratings yet
- Breathing ControlDocument7 pagesBreathing Controlesti kusumaNo ratings yet
- Art 3Document7 pagesArt 3Karen Paola Higuera GastelumNo ratings yet
- Example 2Document5 pagesExample 2Сергей СтанишевNo ratings yet
- Tratamiento Deglución en Enfermedad de ParkinsonDocument8 pagesTratamiento Deglución en Enfermedad de ParkinsonMacarena Paz ÁlvarezNo ratings yet
- Dance For PDDocument6 pagesDance For PDfozia hayyatNo ratings yet
- Effectiveness of Horticultural Therapy: A Systematic Review of Randomized Controlled TrialsDocument14 pagesEffectiveness of Horticultural Therapy: A Systematic Review of Randomized Controlled TrialsIntanAgustiFernandesNo ratings yet
- Effect of 4 7 8 Breathing Technique On ADocument9 pagesEffect of 4 7 8 Breathing Technique On AHafsa AzizNo ratings yet
- Depressive Symptoms in Patients With Subclinical Hypothyroidism The Effect of Treatment With Levothyroxine A Double Blind Randomized Clinical TrialDocument6 pagesDepressive Symptoms in Patients With Subclinical Hypothyroidism The Effect of Treatment With Levothyroxine A Double Blind Randomized Clinical TrialastrogliaNo ratings yet
- El Nazer 2014Document26 pagesEl Nazer 2014priyaNo ratings yet
- 10 1016@j Psyneuen 2017 09 007Document43 pages10 1016@j Psyneuen 2017 09 007Febyan AbotNo ratings yet
- A 12-Month, Moderate-Intensity Exercise Training Program Improves Fitness and Quality of Life in Adults With Asthma: A Controlled TrialDocument3 pagesA 12-Month, Moderate-Intensity Exercise Training Program Improves Fitness and Quality of Life in Adults With Asthma: A Controlled TrialAmir SaifudinNo ratings yet
- Avances en Terapia de Rehabilitacion CardiopulmonarDocument13 pagesAvances en Terapia de Rehabilitacion CardiopulmonarMaría Camila Zuluaga AriasNo ratings yet
- Jurnal SleepDocument14 pagesJurnal SleepFitri Mariana NainggolanNo ratings yet
- Mondelli Et Al. - 2015 - Cortisol and Inflammatory Biomarkers Predict Poor Treatment Response in First Episode Psychosis-AnnotatedDocument9 pagesMondelli Et Al. - 2015 - Cortisol and Inflammatory Biomarkers Predict Poor Treatment Response in First Episode Psychosis-AnnotatedMiraNo ratings yet
- Piis0149291815001484 PDFDocument10 pagesPiis0149291815001484 PDFWarunee MingpunNo ratings yet
- Prada2015 Article AdditionOfMethylphenidateToIntDocument11 pagesPrada2015 Article AdditionOfMethylphenidateToIntPaula TrindadeNo ratings yet
- Hads - Cambios MinimosDocument9 pagesHads - Cambios MinimosJorge GámezNo ratings yet
- Jurnal HBOT PD Autis PDFDocument13 pagesJurnal HBOT PD Autis PDFSekar Ayu WulandariNo ratings yet
- 3 2 18 947Document6 pages3 2 18 947erichaNo ratings yet
- EreduaDocument5 pagesEreduaAnder GilNo ratings yet
- Rajiv P. Sharma Et Al - CSF Neurotensin Concentrations and Antipsychotic Treatment in Schizophrenia and Schizoaffective DisorderDocument3 pagesRajiv P. Sharma Et Al - CSF Neurotensin Concentrations and Antipsychotic Treatment in Schizophrenia and Schizoaffective DisorderLonkesNo ratings yet
- Tos CronicaDocument12 pagesTos CronicasaloNo ratings yet
- 8 T MG MRWRW8 Ms 99 NC NM XFy QPDocument3 pages8 T MG MRWRW8 Ms 99 NC NM XFy QPJulieta MartinezNo ratings yet
- Paliperidona Revision 18 PagsDocument19 pagesPaliperidona Revision 18 PagsRodrigo SosaNo ratings yet
- Jurnal 4Document6 pagesJurnal 4Raymond FrazierNo ratings yet
- Hasler 2015Document32 pagesHasler 2015Seplou7iNo ratings yet
- Mds 21803Document7 pagesMds 21803Elisa FioraNo ratings yet
- Review of Related Literature of SchizophreniaDocument6 pagesReview of Related Literature of Schizophreniac5rqq644100% (1)
- Long Term Vs Short TermDocument9 pagesLong Term Vs Short TermHerizko KusumaNo ratings yet
- Cognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationFrom EverandCognitive Behavioral Psychopharmacology: The Clinical Practice of Evidence-Based Biopsychosocial IntegrationMark MuseNo ratings yet
- 9200 Power Meter: Installation & Operation GuideDocument28 pages9200 Power Meter: Installation & Operation GuideLuis Fernando Casas RomeroNo ratings yet
- Wendra Deka Saputra: P R O F Il EDocument1 pageWendra Deka Saputra: P R O F Il EvheNo ratings yet
- Report - Bogi Manish Kumar - PTS-05Document63 pagesReport - Bogi Manish Kumar - PTS-05Sai Prasad GoudNo ratings yet
- Emotional Disturbance Annotated BibliographyDocument3 pagesEmotional Disturbance Annotated Bibliographyapi-335203912No ratings yet
- T.E Question Papers (2012 Pattern) May 2015Document297 pagesT.E Question Papers (2012 Pattern) May 2015Prof. Avinash MahaleNo ratings yet
- Parenting Style in Pediatric Dentistry PDFDocument7 pagesParenting Style in Pediatric Dentistry PDFJude Aldo PaulNo ratings yet
- Lab 2: Anatomy of The Heart: General ConsiderationsDocument19 pagesLab 2: Anatomy of The Heart: General ConsiderationsDisshiNo ratings yet
- Viamed Catalog 2012 PDFDocument68 pagesViamed Catalog 2012 PDFLuis SorianoNo ratings yet
- 10-Formulation and Evaluation of Effervescent Tablets of ParacetamolDocument30 pages10-Formulation and Evaluation of Effervescent Tablets of ParacetamolRodrigo InostrozaNo ratings yet
- Magic Mushroom Spores - Where To Buy Psilocybin Spo - 240105 - 183240Document24 pagesMagic Mushroom Spores - Where To Buy Psilocybin Spo - 240105 - 183240coreeastcapitalNo ratings yet
- 10th Science EM Half Yearly 2022 Original Question Paper Thenkasi District English Medium PDF DownloadDocument2 pages10th Science EM Half Yearly 2022 Original Question Paper Thenkasi District English Medium PDF DownloadJbNo ratings yet
- New Promotional & Incentive Structure of PLI & RPLIDocument14 pagesNew Promotional & Incentive Structure of PLI & RPLIkaaushik maityNo ratings yet
- Cod and PodDocument5 pagesCod and PodYasser AshourNo ratings yet
- Engineering Manual: Variable Refrigerant Flow Outdoor Units 6.0 To 42.0 TonsDocument156 pagesEngineering Manual: Variable Refrigerant Flow Outdoor Units 6.0 To 42.0 TonsNey Raul Benji JoaquinNo ratings yet
- Frescolat MGAMenthone Glyceryl Acetal SDSDocument9 pagesFrescolat MGAMenthone Glyceryl Acetal SDSMihaNo ratings yet
- LEEA ACADEMY Course Study Materials - MCE - V1.0 Mar 2020-MergedDocument189 pagesLEEA ACADEMY Course Study Materials - MCE - V1.0 Mar 2020-MergedRana DanishNo ratings yet
- Dheeraj Coca Cola MbaDocument84 pagesDheeraj Coca Cola Mbaranaindia2011100% (1)
- A Nun's CuntDocument12 pagesA Nun's CuntjhukillNo ratings yet
- Constituents of Environment: Physical or Abiotic EnvironmentDocument6 pagesConstituents of Environment: Physical or Abiotic EnvironmentAvvai VijayaNo ratings yet
- A History of AspirinDocument3 pagesA History of AspirinMulyaniNo ratings yet
- Abu Dhabi Recommended Plant PDFDocument30 pagesAbu Dhabi Recommended Plant PDFelmerbarrerasNo ratings yet
- All at Sea Caribbean 0917Document112 pagesAll at Sea Caribbean 0917Scott NeumanNo ratings yet
- Attachment Theory in Adult PsychiatryDocument10 pagesAttachment Theory in Adult PsychiatryEsteli189No ratings yet
- CompetitorsDocument6 pagesCompetitorsSadaf HanifNo ratings yet
- Summary of AFSCME Tentative MOUDocument5 pagesSummary of AFSCME Tentative MOUjon_ortizNo ratings yet
- Lesson 6 NCM 103Document5 pagesLesson 6 NCM 103KIM KALIBAYNo ratings yet
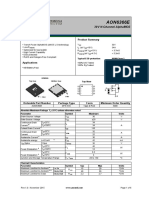
- AON6366E: General Description Product SummaryDocument6 pagesAON6366E: General Description Product SummaryHumberto YumaNo ratings yet