Download as docx, pdf, or txt
You might also like
- Housecalls 101: Policy and Procedure Manual for Medical Home VisitsFrom EverandHousecalls 101: Policy and Procedure Manual for Medical Home VisitsNo ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Filipino Culture Values and Practices in Relation To Drug Administration 1 4 PDFDocument3 pagesFilipino Culture Values and Practices in Relation To Drug Administration 1 4 PDFBianca Marithè RejanoNo ratings yet
- Health AssessmentDocument28 pagesHealth AssessmentPiyush Dutta100% (2)
- Chapter 1 Critical ThinkingDocument3 pagesChapter 1 Critical Thinkingsam100% (2)
- Nursing ProcessDocument68 pagesNursing ProcessRaquel M. Mendoza86% (7)
- Nursing ProcessDocument99 pagesNursing ProcessGeetaVikasShiroor60% (5)
- Subjective Cues:: Nursing Care ProcessDocument8 pagesSubjective Cues:: Nursing Care ProcessBianca Marithè RejanoNo ratings yet
- 1 - Participate in Workplace CommunicaitonDocument38 pages1 - Participate in Workplace CommunicaitonSahlee Rose Falcunit GacaNo ratings yet
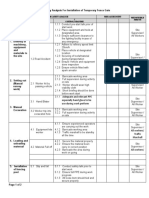
- ULSADO-JSA - Installation of Temporary Fence GateDocument2 pagesULSADO-JSA - Installation of Temporary Fence GateKelvin TanNo ratings yet
- Remember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your OwnDocument11 pagesRemember: Goals and Plan of Care Should Be Base According To Client's Problems/needs NOT According To Your Ownavinash dhameriyaNo ratings yet
- Concepts, Process, and Practice Kozier & Erb's 9 Edition: Fundamentals of NursingDocument7 pagesConcepts, Process, and Practice Kozier & Erb's 9 Edition: Fundamentals of NursingLester Paul SivilaNo ratings yet
- Nursing Process: Ns. Nuning Khurotul Af'ida, S.Kep.,M.KepDocument91 pagesNursing Process: Ns. Nuning Khurotul Af'ida, S.Kep.,M.KepDindaaNo ratings yet
- Fundamentals in NursingDocument17 pagesFundamentals in Nursingreymar.martinez88No ratings yet
- Assignment of Nursing Process FinalDocument43 pagesAssignment of Nursing Process FinalSandhya Gupta100% (1)
- NCM103 the Nursing ProcessDocument10 pagesNCM103 the Nursing ProcessJude RiveraNo ratings yet
- Nursing Process SOAPIEDocument33 pagesNursing Process SOAPIEChoi Gong Ju100% (4)
- CU02A WEEK02-NursingProcessinPMHNPractice28VAL2928129MODULEDocument8 pagesCU02A WEEK02-NursingProcessinPMHNPractice28VAL2928129MODULEduca.danrainer02No ratings yet
- Presentation On Health AssessmentDocument12 pagesPresentation On Health AssessmentSimran ChauhanNo ratings yet
- Reviewer Final 1Document6 pagesReviewer Final 1zabalaiiirogeliopaclibarNo ratings yet
- Purposes of The Nursing ProcessDocument11 pagesPurposes of The Nursing ProcessNica NixNo ratings yet
- Nursing Care Plan - PPT HandoutDocument43 pagesNursing Care Plan - PPT HandoutCharlie Abagon100% (4)
- Nursing ProcessDocument62 pagesNursing ProcessplethoraldorkNo ratings yet
- Nursing ProcessDocument7 pagesNursing ProcessAdrian Dela PeñaNo ratings yet
- Fundies II Exam 1 Blue PrintDocument24 pagesFundies II Exam 1 Blue PrintStephanieNo ratings yet
- Nursing ProcessDocument62 pagesNursing ProcessMara MaraNo ratings yet
- Week3-5Nursing Process-OUTLINEDocument4 pagesWeek3-5Nursing Process-OUTLINEemman.magtibayNo ratings yet
- Nursing AssesmentDocument38 pagesNursing AssesmentbbpanickerNo ratings yet
- The Nursing Process in Psychiatric/Mental Health Nursing: PlanningDocument49 pagesThe Nursing Process in Psychiatric/Mental Health Nursing: PlanningJonalynCollodChewacheo50% (2)
- Ha WK2Document9 pagesHa WK2MARY ROSE FAJUTINANo ratings yet
- Health AssessmentDocument15 pagesHealth AssessmentmeghanaNo ratings yet
- Health Assessment AssignmentDocument15 pagesHealth Assessment Assignmentpslokesha84No ratings yet
- Nursing ProcessDocument15 pagesNursing ProcessCreole Kaye RubiaNo ratings yet
- Nursing Process ModuleDocument21 pagesNursing Process ModuledocgioreNo ratings yet
- Introduction To Health AssessmentDocument5 pagesIntroduction To Health AssessmentHanna BuadaNo ratings yet
- Ha NotesDocument39 pagesHa NotesGlecy Ann MagnoNo ratings yet
- NSG Process NEWDocument135 pagesNSG Process NEWRhea Lyn LamosteNo ratings yet
- Nursing AssesmentDocument39 pagesNursing AssesmentRed Jimeno100% (1)
- #1 - 1st Day NCM 01 - Lec - Reviewer PrelimDocument14 pages#1 - 1st Day NCM 01 - Lec - Reviewer PrelimNurse TinNo ratings yet
- NCM 103 Handouts 4-1Document4 pagesNCM 103 Handouts 4-1Alexsa AranteNo ratings yet
- TFN Review 1Document5 pagesTFN Review 1Anthony RiggsNo ratings yet
- Nursing Process: S6.M6.Ppt-NcpDocument16 pagesNursing Process: S6.M6.Ppt-NcpDevit AriantiNo ratings yet
- Introduction To Health AssessmentDocument3 pagesIntroduction To Health AssessmentAngela SaavedraNo ratings yet
- HA LEC 01 Introduction To Health AssessmentDocument24 pagesHA LEC 01 Introduction To Health AssessmentHarisu VCNo ratings yet
- Nursing Process 2Document90 pagesNursing Process 2rerenrahmawatiNo ratings yet
- NursingDocument61 pagesNursingMrs Rehan50% (2)
- #3 - 2nd Day NCM 01 - Lab - Reviewer PrelimDocument20 pages#3 - 2nd Day NCM 01 - Lab - Reviewer PrelimNurse TinNo ratings yet
- Review of Nursing Plan ANPIEDocument2 pagesReview of Nursing Plan ANPIEJenn WardNo ratings yet
- Module 1 Rle-AssessmentDocument3 pagesModule 1 Rle-AssessmentKyle VargasNo ratings yet
- The Nursing ProcessDocument28 pagesThe Nursing Processjoyce_marie_20% (1)
- Decena, Cyrille Justine A. BSN-1A NCM 100 Lec - HomeworkDocument9 pagesDecena, Cyrille Justine A. BSN-1A NCM 100 Lec - HomeworkCyrille DecenaNo ratings yet
- W1 Nursing ProcessDocument18 pagesW1 Nursing ProcessColeen Tan100% (1)
- Ho Complete Nursing Process 2024Document21 pagesHo Complete Nursing Process 2024Jasmine DamianNo ratings yet
- Nursing ProcessDocument5 pagesNursing Processanimesh pandaNo ratings yet
- The Nursing ProcessDocument17 pagesThe Nursing ProcessElla Lobenaria100% (1)
- Health AssessmentDocument3 pagesHealth AssessmentCres Padua QuinzonNo ratings yet
- Midwifery Skills Clinical Laboratory: The Midwives ProcessDocument26 pagesMidwifery Skills Clinical Laboratory: The Midwives ProcessNano KaNo ratings yet
- Health Care ProcessDocument104 pagesHealth Care ProcessKylaCruz100% (2)
- HA Lecture Week 1 REVIEW OF The NURSING PROCESSDocument6 pagesHA Lecture Week 1 REVIEW OF The NURSING PROCESSLore Anne Mhae SantosNo ratings yet
- TFN 3Document4 pagesTFN 3Kianna BatiancilaNo ratings yet
- Health Ass ReviewerDocument8 pagesHealth Ass ReviewerchristinejeancenabreNo ratings yet
- NCM 103 Midterm Review Material - 013138Document28 pagesNCM 103 Midterm Review Material - 013138kessiabon459No ratings yet
- Medical Health Clinic: a Social Care Guide Book 2: Social Care Housing and Hotels Conservatism PolicyFrom EverandMedical Health Clinic: a Social Care Guide Book 2: Social Care Housing and Hotels Conservatism PolicyNo ratings yet
- N036 NSTP Narrative Report Magpantay Melanie S.Document10 pagesN036 NSTP Narrative Report Magpantay Melanie S.Bianca Marithè RejanoNo ratings yet
- Rejano Drug-Study (Folic Acid)Document3 pagesRejano Drug-Study (Folic Acid)Bianca Marithè RejanoNo ratings yet
- n032 Rejano Bianca Marithe Activity 9Document2 pagesn032 Rejano Bianca Marithe Activity 9Bianca Marithè RejanoNo ratings yet
- N039-N040 Rejano Nursing Care PlanDocument3 pagesN039-N040 Rejano Nursing Care PlanBianca Marithè RejanoNo ratings yet
- College of Health Sciences: Urdaneta City UniversityDocument4 pagesCollege of Health Sciences: Urdaneta City UniversityBianca Marithè RejanoNo ratings yet
- Urdaneta City University: Bachelor of Science in NursingDocument1 pageUrdaneta City University: Bachelor of Science in NursingBianca Marithè RejanoNo ratings yet
- College of Health SciencesDocument2 pagesCollege of Health SciencesBianca Marithè RejanoNo ratings yet
- Drug Sudy Format MethyldopaDocument3 pagesDrug Sudy Format MethyldopaBianca Marithè RejanoNo ratings yet
- College of Health Sciences: Urdaneta City UniversityDocument4 pagesCollege of Health Sciences: Urdaneta City UniversityBianca Marithè RejanoNo ratings yet
- Drug Study Folic AcidDocument14 pagesDrug Study Folic AcidBianca Marithè Rejano0% (1)
- Assess Vital Signs For Baseline Data. Assess Vital Signs For Baseline Data. Directl y Affects NeuroreDocument14 pagesAssess Vital Signs For Baseline Data. Assess Vital Signs For Baseline Data. Directl y Affects NeuroreBianca Marithè RejanoNo ratings yet
- UNIT 1: Introduction: Topic OutlineDocument7 pagesUNIT 1: Introduction: Topic OutlineBianca Marithè RejanoNo ratings yet
- Rejano Case Scenario 2 - Drug StudyDocument3 pagesRejano Case Scenario 2 - Drug StudyBianca Marithè RejanoNo ratings yet
- Rejano Case Scenario 2 - Fdar ChartingDocument1 pageRejano Case Scenario 2 - Fdar ChartingBianca Marithè RejanoNo ratings yet
- Contemporary Social Dance 101Document32 pagesContemporary Social Dance 101Bianca Marithè Rejano0% (1)
- Contemporary Art: Contemporary Art Is The Art of Today, Produced in The Second Half of The 20thDocument3 pagesContemporary Art: Contemporary Art Is The Art of Today, Produced in The Second Half of The 20thBianca Marithè RejanoNo ratings yet
- Chapter 28 ImmobilityDocument2 pagesChapter 28 ImmobilityBianca Marithè RejanoNo ratings yet
- Contemporary ArtsDocument6 pagesContemporary ArtsBianca Marithè RejanoNo ratings yet
- Topic 2: Same-Sex Marriage What Is Same-Sex Marriage?Document4 pagesTopic 2: Same-Sex Marriage What Is Same-Sex Marriage?Bianca Marithè RejanoNo ratings yet
- Kant and Rights TheoristsDocument3 pagesKant and Rights TheoristsBianca Marithè Rejano100% (1)
- HA Filler Injection and Skin Quality-Literature MiDocument9 pagesHA Filler Injection and Skin Quality-Literature MiEnt IMDCNo ratings yet
- BDSM As Trauma PlayDocument17 pagesBDSM As Trauma Playaeiman zazNo ratings yet
- (F21) FYDP Proposal FormDocument4 pages(F21) FYDP Proposal FormSaira FaisalNo ratings yet
- The Art of Giving Up - TDocument4 pagesThe Art of Giving Up - TНадя КонончукNo ratings yet
- PD Lesson 5 Coping With Stress in Middle and Late AdolescenceDocument16 pagesPD Lesson 5 Coping With Stress in Middle and Late AdolescenceEL FuentesNo ratings yet
- 【 I.K.G.A】: International Karate-Do Goju-Kai AssociationDocument1 page【 I.K.G.A】: International Karate-Do Goju-Kai AssociationRobert AlvezNo ratings yet
- Boostvocab1 12Document37 pagesBoostvocab1 12LêThừaKhangNo ratings yet
- Lace Flames The Kimberly Chronicles Book One Lainey Reese Full ChapterDocument51 pagesLace Flames The Kimberly Chronicles Book One Lainey Reese Full Chapterlinda.walsh847100% (10)
- UNIV144 Questions 2Document8 pagesUNIV144 Questions 2Clinton SmaugNo ratings yet
- Biopsychosocial Model in Depression Revisited: Mauro Garcia-Toro, Iratxe AguirreDocument9 pagesBiopsychosocial Model in Depression Revisited: Mauro Garcia-Toro, Iratxe AguirreayannaxemNo ratings yet
- Physical Exercise and Executive Functions in Preadolescent Children, Adolescents and Young Adults - A Meta-AnalysisDocument9 pagesPhysical Exercise and Executive Functions in Preadolescent Children, Adolescents and Young Adults - A Meta-AnalysisPedro J. Conesa CerveraNo ratings yet
- Family Life Stages - NewDocument22 pagesFamily Life Stages - NewAhmad Yazid HilmiNo ratings yet
- Detailed Lesson Plan in Physical Education Grade 4Document6 pagesDetailed Lesson Plan in Physical Education Grade 4Myca HernandezNo ratings yet
- Pediatrics Drugs-1Document3 pagesPediatrics Drugs-1seemahasheesh93No ratings yet
- Septic Shock: Current Management and New Therapeutic FrontiersDocument77 pagesSeptic Shock: Current Management and New Therapeutic Frontiersamal.fathullahNo ratings yet
- DessyDocument5 pagesDessyYenita sariNo ratings yet
- BCGL Ladies April Newsletter 2022Document7 pagesBCGL Ladies April Newsletter 2022api-324618538No ratings yet
- 19 - Pulv - SDSDocument11 pages19 - Pulv - SDSBoon ChewNo ratings yet
- Benefits of Living DonationDocument1 pageBenefits of Living DonationRanga RajanNo ratings yet
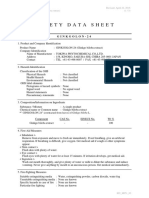
- MSDS GINKGOLON-24 (Ginkgo Biloba Ext)Document3 pagesMSDS GINKGOLON-24 (Ginkgo Biloba Ext)Selviani Dwi MuryantiNo ratings yet
- Pediatric Community Acquired PneumoniaDocument24 pagesPediatric Community Acquired PneumoniaJames Lagamayo JavierNo ratings yet
- ResumDocument11 pagesResummmmmder7No ratings yet
- Nama Kelompok (1) : 1. Al-Azmi 2. Andreas Santo Calvin Nainggolan 3. Andre Priono S 4. Fadilla Rizky 5. Hafist Ardana Verianto 6. M.Bagas Sadeva 7Document3 pagesNama Kelompok (1) : 1. Al-Azmi 2. Andreas Santo Calvin Nainggolan 3. Andre Priono S 4. Fadilla Rizky 5. Hafist Ardana Verianto 6. M.Bagas Sadeva 7Hafis ArdanaNo ratings yet
- Module 5 Notebook Individual Service PlanDocument44 pagesModule 5 Notebook Individual Service PlanAung Tun100% (1)
- Alternate Rapid Maxillary Expansion and Constriction (Alt-RAMEC) Protocol: A Comprehensive Literature ReviewDocument5 pagesAlternate Rapid Maxillary Expansion and Constriction (Alt-RAMEC) Protocol: A Comprehensive Literature ReviewGaby Cotrina LiñanNo ratings yet
- Kamilya Jamel Baljon, Muhammad Hibatullah Romli, Adibah Hanim Ismail, Lee Khuan, Boon How ChewDocument13 pagesKamilya Jamel Baljon, Muhammad Hibatullah Romli, Adibah Hanim Ismail, Lee Khuan, Boon How ChewOva Tri Pra Setia MayasarieNo ratings yet
- Unit 4 Vocab ComicDocument10 pagesUnit 4 Vocab ComicTrúc TrúcNo ratings yet
- Sansulin R Suspensi Injeksi 100 IU, ML - Rekombinan Insulin Manusia - DKI0708100443A1 - 2016Document2 pagesSansulin R Suspensi Injeksi 100 IU, ML - Rekombinan Insulin Manusia - DKI0708100443A1 - 2016Yessi VirginiaNo ratings yet