Download as pdf or txt
You might also like
- Biology Investigatory Project: Topic - DiabetesDocument19 pagesBiology Investigatory Project: Topic - Diabetesaditya gollakota83% (40)
- Qip Fall PreventionDocument10 pagesQip Fall PreventionNandakishore Rajkumar100% (1)
- File 146 - Stupid-UsmleDocument14 pagesFile 146 - Stupid-UsmlePrarthana100% (4)
- Maternal Neonatal Facts Made Incredibly Quick! 2nd EdDocument112 pagesMaternal Neonatal Facts Made Incredibly Quick! 2nd Edmarione2489% (9)
- Rekomendasi Pemberian Covid-19Document35 pagesRekomendasi Pemberian Covid-19ekaNo ratings yet
- Statistic Id917148 Leading Health Problems Worldwide 2022Document8 pagesStatistic Id917148 Leading Health Problems Worldwide 2022Saksham BavejaNo ratings yet
- Prof. Lesmana - The 4th Liv GI Fair PGC On Hepatitis C Evolution of DAA (Direct Acting Antiviral AgentDocument26 pagesProf. Lesmana - The 4th Liv GI Fair PGC On Hepatitis C Evolution of DAA (Direct Acting Antiviral AgentWenny NgawingNo ratings yet
- OHSU COVID-19 Forecast Nov. 24, 2021Document43 pagesOHSU COVID-19 Forecast Nov. 24, 2021KGW NewsNo ratings yet
- OHSU COVID Forecast: Edition: 12/17/2021Document46 pagesOHSU COVID Forecast: Edition: 12/17/2021Sinclair Broadcast Group - EugeneNo ratings yet
- Hypertension Covid 19 PDFDocument5 pagesHypertension Covid 19 PDFfauzanemir3No ratings yet
- 23176-Article Text-90958-2-10-20201228Document9 pages23176-Article Text-90958-2-10-20201228Maria Carrasco ColonioNo ratings yet
- Ohio Poll ResultsDocument13 pagesOhio Poll ResultsSpectrum NewsNo ratings yet
- Materi Webinar Operations Perspective (9 April)Document14 pagesMateri Webinar Operations Perspective (9 April)armabar 30No ratings yet
- Thromboembolic Disease During Tuberculosis: A Series of 47 CasesDocument6 pagesThromboembolic Disease During Tuberculosis: A Series of 47 CasesIJAR JOURNALNo ratings yet
- Dead Recovered Confirmed Tested Hotline: Situation Report NoDocument12 pagesDead Recovered Confirmed Tested Hotline: Situation Report NoSusan ArafatNo ratings yet
- Situasi Global PD3I 7 Feb 2022Document21 pagesSituasi Global PD3I 7 Feb 2022FAIZ FANINo ratings yet
- Exclusive Spectrum News/Ipsos Poll Takes Floridians' Pulse On Trump, COVID-19 ResponseDocument13 pagesExclusive Spectrum News/Ipsos Poll Takes Floridians' Pulse On Trump, COVID-19 ResponseSpectrum NewsNo ratings yet
- Final - Extending The Use of SGLT2i On DKD DR YennyDocument33 pagesFinal - Extending The Use of SGLT2i On DKD DR Yennyxiongmao2389No ratings yet
- Ko-Infeksi Hepatitis HIV Pencegahan Dan Penanggulangannya - UNODC Okt 2010Document85 pagesKo-Infeksi Hepatitis HIV Pencegahan Dan Penanggulangannya - UNODC Okt 2010ingridNo ratings yet
- Public Poll Findings and MethodologyDocument13 pagesPublic Poll Findings and MethodologySpectrum NewsNo ratings yet
- UntitledDocument14 pagesUntitledJavier PintoNo ratings yet
- Situation Report No.: Dead Recovered Confirmed Tested IsolatedDocument12 pagesSituation Report No.: Dead Recovered Confirmed Tested Isolateddinar aimcNo ratings yet
- Dead Recovered Confirmed Tested Isolated: Situation Report NoDocument10 pagesDead Recovered Confirmed Tested Isolated: Situation Report NoAbu UsamaNo ratings yet
- A Study On People'S Mental Health Conditions During COVID-19Document16 pagesA Study On People'S Mental Health Conditions During COVID-19Ansu NitNo ratings yet
- COVID-19: Novel Coronavirus and IVC Current Guidelines and Clinical TrialsDocument9 pagesCOVID-19: Novel Coronavirus and IVC Current Guidelines and Clinical Trialsbella labibahNo ratings yet
- Clinical Use and Positioning of Rapid Antigen Test in COVID-19 - DR Tonang Ardyanto. SP - PK, PHDDocument21 pagesClinical Use and Positioning of Rapid Antigen Test in COVID-19 - DR Tonang Ardyanto. SP - PK, PHDRiaak ImNo ratings yet
- Full Spectrum of COVID-19 Severity Still Being DepictedDocument1 pageFull Spectrum of COVID-19 Severity Still Being DepictedpoopNo ratings yet
- Ipsos Global Health Service Monitor 2022 VDEFDocument32 pagesIpsos Global Health Service Monitor 2022 VDEFalvin susetyoNo ratings yet
- Midland Memorial COVID-19 ReportDocument1 pageMidland Memorial COVID-19 ReportMidland Reporter-TelegramNo ratings yet
- Plagiarism ReportDocument47 pagesPlagiarism ReportRiya YadavNo ratings yet
- Sharing Webinar Lamudi & FB - CompressedDocument26 pagesSharing Webinar Lamudi & FB - CompressedPasukan EliteNo ratings yet
- EHS Presentation June4-1Document30 pagesEHS Presentation June4-1chidieberemmezi9No ratings yet
- Which Lessons Shall We Learn From The 2019 Novel Coronavirus Outbreak?Document5 pagesWhich Lessons Shall We Learn From The 2019 Novel Coronavirus Outbreak?TeoMartinNo ratings yet
- Pakistan: No Data Available No Data AvailableDocument1 pagePakistan: No Data Available No Data AvailableArooj EhsanNo ratings yet
- Hepatitis BDocument13 pagesHepatitis BFemi luwitaNo ratings yet
- Maternal Health: Family Revolves Around MotherDocument16 pagesMaternal Health: Family Revolves Around MotherFatima IqbalNo ratings yet
- Fy20 + Fy21Td Med Path Data: Casey McgrathDocument4 pagesFy20 + Fy21Td Med Path Data: Casey McgrathChadNo ratings yet
- 3,607 Florida Schools Have Report COVID-19 Cases: Students Teachers Staff Elementary Middle High OtherDocument4 pages3,607 Florida Schools Have Report COVID-19 Cases: Students Teachers Staff Elementary Middle High OtherAdam PoulisseNo ratings yet
- Dr. Finny Fitri Yani - COVID-19 - Great - Imitator-1Document39 pagesDr. Finny Fitri Yani - COVID-19 - Great - Imitator-1budi darmantaNo ratings yet
- CKD and CovidDocument5 pagesCKD and CovidLouije MombzNo ratings yet
- Situation Report No.: Tested Confirmed Recovered Dead IsolatedDocument13 pagesSituation Report No.: Tested Confirmed Recovered Dead IsolatedDinar HassanNo ratings yet
- Critical CareDocument29 pagesCritical CareThalia LopesNo ratings yet
- Dashboard of Public Health Indicators: Newly Reported Cases Today Confirmed CasesDocument19 pagesDashboard of Public Health Indicators: Newly Reported Cases Today Confirmed CasesLyleChristineNo ratings yet
- Inline Supplementary Material 1Document3 pagesInline Supplementary Material 1theffNo ratings yet
- Varicella SR 2019 FINALDocument1 pageVaricella SR 2019 FINALcdsaludNo ratings yet
- Afghanistan: 2016 TOTAL POPULATION: 34 656 000 2016 TOTAL DEATHS: 248 000Document1 pageAfghanistan: 2016 TOTAL POPULATION: 34 656 000 2016 TOTAL DEATHS: 248 000Re ZaNo ratings yet
- COVID-19: Total Tests Confirmed Cured Dead IsolationDocument10 pagesCOVID-19: Total Tests Confirmed Cured Dead IsolationmogembooNo ratings yet
- Geriatric Medicine and GerontologyDocument7 pagesGeriatric Medicine and GerontologyNoor FadlanNo ratings yet
- Mar en PDFDocument1 pageMar en PDFمحمد الزرهونيNo ratings yet
- HTN Slide Deck NewDocument27 pagesHTN Slide Deck NewChristy BerryNo ratings yet
- Consumer Buying ProcessDocument6 pagesConsumer Buying ProcessSandip NandyNo ratings yet
- Role of Finerenone As New Pillar in CKD Management in T2D Patients - GPMPDocument29 pagesRole of Finerenone As New Pillar in CKD Management in T2D Patients - GPMPTaufiqurrokhman RofiiNo ratings yet
- Leger Report - National Healthcare SurveyDocument36 pagesLeger Report - National Healthcare SurveyCityNewsTorontoNo ratings yet
- Case Control - Angga AdnyanaDocument9 pagesCase Control - Angga AdnyanaLalu FarosNo ratings yet
- HPV Evaluation of Head and Neck Cancer Awareness and Screening Status in Jeddah, Saudi ArabiaDocument5 pagesHPV Evaluation of Head and Neck Cancer Awareness and Screening Status in Jeddah, Saudi ArabiakarinagitakNo ratings yet
- Jordan NCD FactsheetDocument1 pageJordan NCD FactsheetmonzcoNo ratings yet
- Study of Clinical Profile, Risk-Factors and Management of Post Partum Haemorrhage in A Tertiary Care CentreDocument5 pagesStudy of Clinical Profile, Risk-Factors and Management of Post Partum Haemorrhage in A Tertiary Care CentreIJAR JOURNALNo ratings yet
- Ederhy Cardio OncologieDocument126 pagesEderhy Cardio OncologieRoxana MateiNo ratings yet
- ADVANCE-On EASD Study Rationale and DesignDocument26 pagesADVANCE-On EASD Study Rationale and Designmariatul fithriasariNo ratings yet
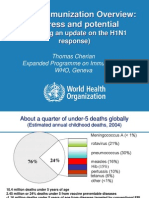
- Global Immunization Overview: Progress and PotentialDocument36 pagesGlobal Immunization Overview: Progress and PotentialPrabir Kumar ChatterjeeNo ratings yet
- Chinese Guideline of Diagnosis and Treatment of COVID-19: Bin Cao, MDDocument30 pagesChinese Guideline of Diagnosis and Treatment of COVID-19: Bin Cao, MDKatherine DelgadoNo ratings yet
- Massachusetts Department of Public Health COVID-19 DashboardDocument24 pagesMassachusetts Department of Public Health COVID-19 DashboardRami Abou-SabeNo ratings yet
- ACRP Certification Handbook 2024 V1Document18 pagesACRP Certification Handbook 2024 V1PrarthanaNo ratings yet
- Bio Sketch Deepu SudhakaranDocument1 pageBio Sketch Deepu SudhakaranPrarthanaNo ratings yet
- USMLE Review High Yield 2020Document1 pageUSMLE Review High Yield 2020PrarthanaNo ratings yet
- 2020 AnnualReport Research10Document43 pages2020 AnnualReport Research10PrarthanaNo ratings yet
- Biochemistry: Serum Creatinine Serum Sodium Serum PotassiumDocument4 pagesBiochemistry: Serum Creatinine Serum Sodium Serum PotassiumPrarthanaNo ratings yet
- Students' Section: ADMISSION STATUS & DETAILS - I MBBS 2011-12 BATCH "L" BATCH (2011-12)Document3 pagesStudents' Section: ADMISSION STATUS & DETAILS - I MBBS 2011-12 BATCH "L" BATCH (2011-12)PrarthanaNo ratings yet
- U2002 PDFDocument4 pagesU2002 PDFPrarthanaNo ratings yet
- Embryology: Lung DevelopmentDocument91 pagesEmbryology: Lung DevelopmentPrarthanaNo ratings yet
- Students' Section: ADMISSION STATUS & DETAILS - I MBBS 2008-09 BATCHDocument3 pagesStudents' Section: ADMISSION STATUS & DETAILS - I MBBS 2008-09 BATCHPrarthanaNo ratings yet
- U2003 PDFDocument3 pagesU2003 PDFPrarthanaNo ratings yet
- General Pathology: Growth AdaptationsDocument93 pagesGeneral Pathology: Growth AdaptationsPrarthanaNo ratings yet
- Students' Section: ADMISSION STATUS & DETAILS - I MBBS 2006-07 BATCHDocument3 pagesStudents' Section: ADMISSION STATUS & DETAILS - I MBBS 2006-07 BATCHPrarthanaNo ratings yet
- U2000 PDFDocument3 pagesU2000 PDFPrarthanaNo ratings yet
- admission To I M.B.B.S - "H" Batch (2007-08)Document2 pagesadmission To I M.B.B.S - "H" Batch (2007-08)PrarthanaNo ratings yet
- Students' Section: ADMISSION STATUS & DETAILS - I MBBS 2009-10 BATCHDocument3 pagesStudents' Section: ADMISSION STATUS & DETAILS - I MBBS 2009-10 BATCHPrarthanaNo ratings yet
- Roll No Name: Students' Section: ADMISSION STATUS & DETAILS - I MBBS 2013-14 BATCH "N" BATCH (2013-14)Document3 pagesRoll No Name: Students' Section: ADMISSION STATUS & DETAILS - I MBBS 2013-14 BATCH "N" BATCH (2013-14)PrarthanaNo ratings yet
- admission To I M.B.B.S - "E" Batch (2004-05)Document2 pagesadmission To I M.B.B.S - "E" Batch (2004-05)PrarthanaNo ratings yet
- admission To I M.B.B.S - "B" Batch (2001-02)Document3 pagesadmission To I M.B.B.S - "B" Batch (2001-02)PrarthanaNo ratings yet
- Students' Section: ADMISSION STATUS & DETAILS - I MBBS 2012-13 BATCH "M" BATCH (2012-13Document4 pagesStudents' Section: ADMISSION STATUS & DETAILS - I MBBS 2012-13 BATCH "M" BATCH (2012-13PrarthanaNo ratings yet
- CU Shah Medical College, Surendra NagarDocument8 pagesCU Shah Medical College, Surendra NagarPrarthanaNo ratings yet
- Students' Section: ADMISSION STATUS & DETAILS - I MBBS 2014-15 BATCH "O" BATCH (2014-15)Document3 pagesStudents' Section: ADMISSION STATUS & DETAILS - I MBBS 2014-15 BATCH "O" BATCH (2014-15)PrarthanaNo ratings yet
- C. U. Shah Medical College, Surendranagar - I MBBS: 2017-18Document3 pagesC. U. Shah Medical College, Surendranagar - I MBBS: 2017-18PrarthanaNo ratings yet
- C. U. Shah Medical College - P. G. Admissions 2018-19Document8 pagesC. U. Shah Medical College - P. G. Admissions 2018-19PrarthanaNo ratings yet
- Levofloxacin - Wikipedia, The Free EncyclopediaDocument19 pagesLevofloxacin - Wikipedia, The Free EncyclopediaAnkan PalNo ratings yet
- Heat StressDocument2 pagesHeat StressKceey CruzNo ratings yet
- IPT For DepressionDocument13 pagesIPT For Depressionlc49No ratings yet
- The Aga Khan University Sample Aku Test Paper 2019 Post RN BSC Nursing Degree Programme Section I English Time Allowed: 1 HourDocument6 pagesThe Aga Khan University Sample Aku Test Paper 2019 Post RN BSC Nursing Degree Programme Section I English Time Allowed: 1 HourasdfNo ratings yet
- PEMF 8000 BrochureDocument14 pagesPEMF 8000 BrochureLuis CastellanosNo ratings yet
- Acupressure WorkshopDocument5 pagesAcupressure WorkshopDHIMAN CHAKRABORTYNo ratings yet
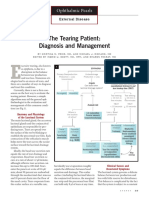
- The Tearing Patient: Diagnosis and Management: Ophthalmic PearlsDocument3 pagesThe Tearing Patient: Diagnosis and Management: Ophthalmic PearlsAnonymous otk8ohj9No ratings yet
- PM Case StudyDocument1 pagePM Case StudyTinersNo ratings yet
- Statins and DiabetesDocument9 pagesStatins and DiabetesJonathan TorresNo ratings yet
- Dr. Aris - Introduction of Anesthesiology DR - Aris, SpAnDocument60 pagesDr. Aris - Introduction of Anesthesiology DR - Aris, SpAnErlita FebriyantiNo ratings yet
- Coronary Slow FlowDocument7 pagesCoronary Slow FlowradiomedicNo ratings yet
- (MP 2004) (AIIMS May 2014) : H Ea LT H C Ar e in in Di A, H Ea LT H PL An Ni N G An D M AnDocument7 pages(MP 2004) (AIIMS May 2014) : H Ea LT H C Ar e in in Di A, H Ea LT H PL An Ni N G An D M AnDr-Sanjay SinghaniaNo ratings yet
- PharmTech NA May2020 US WMDocument64 pagesPharmTech NA May2020 US WMdrs_mdu48100% (1)
- Forensic Med EntomologyDocument304 pagesForensic Med EntomologyCharish DanaoNo ratings yet
- Importance of Prenatal CareDocument12 pagesImportance of Prenatal CarePinkymekala HasanparthyNo ratings yet
- Drugs in Development For Acute Kidney InjuryDocument11 pagesDrugs in Development For Acute Kidney InjurySoniamartilovaNo ratings yet
- Immunology NotesDocument14 pagesImmunology NotesJasmine Bernadette CubillaNo ratings yet
- Case Presentation On CKD With HTNDocument17 pagesCase Presentation On CKD With HTNmanoj sNo ratings yet
- ST GazetteDocument20 pagesST GazetteSt George's Healthcare NHS TrustNo ratings yet
- Manajemen Jalan Nafas Pada Pasien Dengan Tumor Mandibula: Laporan KasusDocument27 pagesManajemen Jalan Nafas Pada Pasien Dengan Tumor Mandibula: Laporan KasusMulia AndaraNo ratings yet
- Case DM Type II + Gangrene Diabeticum +anemiaDocument26 pagesCase DM Type II + Gangrene Diabeticum +anemiaAAn NaNo ratings yet
- PATENT Annexure-A Domestic FilingDocument24 pagesPATENT Annexure-A Domestic FilingMulayam Singh YadavNo ratings yet
- Acute and Chronic HepatitisDocument72 pagesAcute and Chronic HepatitisArun George100% (3)
- Bartholin's Gland Cyst MarsupializationDocument3 pagesBartholin's Gland Cyst MarsupializationIndra JayaNo ratings yet
- Noor Msallaty - 8 Pages of Research PaperDocument16 pagesNoor Msallaty - 8 Pages of Research Paperapi-445615356No ratings yet
- Oral Health: A Window To Your Overall HealthDocument2 pagesOral Health: A Window To Your Overall HealthMOKSHNo ratings yet
- Symptoms of COVID-19Document3 pagesSymptoms of COVID-19Xx XxNo ratings yet