Download as pdf or txt
You might also like
- BORB Birmingham Object Recognition BatteryDocument5 pagesBORB Birmingham Object Recognition BatteryAnaaaerobios0% (1)
- PalmTherapy Program Your Mind by Moshe ZwangDocument751 pagesPalmTherapy Program Your Mind by Moshe Zwangjules6294100% (7)
- Final-Exam Neurosurgery - 3-VersionDocument6 pagesFinal-Exam Neurosurgery - 3-VersionMAMA LALANo ratings yet
- Hubungan Antara Pengetahuan Dan Sikap DG PHBS PD PelajarDocument5 pagesHubungan Antara Pengetahuan Dan Sikap DG PHBS PD PelajarMyrabukitbatasNo ratings yet
- School Teacher's Knowledge, Attitude and Practices Regarding Oral Health in Ballabhgarh Block, FaridabadDocument5 pagesSchool Teacher's Knowledge, Attitude and Practices Regarding Oral Health in Ballabhgarh Block, FaridabadatikramadhaniNo ratings yet
- Final-Exam Neurosurgery - 2-VersionDocument6 pagesFinal-Exam Neurosurgery - 2-VersionMAMA LALA100% (1)
- Final-Exam Neurosurgery - 2-VersionDocument6 pagesFinal-Exam Neurosurgery - 2-VersionMAMA LALA100% (1)
- Mid QuestionsDocument4 pagesMid QuestionsMAMA LALANo ratings yet
- Ce (Ek) F (Ak) PF1 (Ekak) Pfa (Ak) PF2 (Pag)Document6 pagesCe (Ek) F (Ak) PF1 (Ekak) Pfa (Ak) PF2 (Pag)Naji Z. ArandiNo ratings yet
- Jcs 8 105Document6 pagesJcs 8 105nadia syestiNo ratings yet
- The Relationship Between ChildrenDocument14 pagesThe Relationship Between ChildrentirahamdillahNo ratings yet
- Oral Health Knowledge, Attitude, Practices and Oral Health Status Among School Teachers in and Around Lucknow, UP'Document6 pagesOral Health Knowledge, Attitude, Practices and Oral Health Status Among School Teachers in and Around Lucknow, UP'IOSRjournalNo ratings yet
- tmp1F38 TMPDocument6 pagestmp1F38 TMPFrontiersNo ratings yet
- The Relationship Between Children 'S Oral Health-Related Behaviors and Their Caregiver 'S Social SupportDocument10 pagesThe Relationship Between Children 'S Oral Health-Related Behaviors and Their Caregiver 'S Social SupportInce TienNo ratings yet
- Assessment of Knowledge Regarding Oral Hygiene Among Parents of Pre-School Children Attending Pediatric Out Patient Department in Dhulikhel HospitalDocument6 pagesAssessment of Knowledge Regarding Oral Hygiene Among Parents of Pre-School Children Attending Pediatric Out Patient Department in Dhulikhel HospitalSri HariNo ratings yet
- SJDS 34112 120Document9 pagesSJDS 34112 120Eswari PerisamyNo ratings yet
- Nursing Interventions For Malnourished Children and Their Parents JournalDocument8 pagesNursing Interventions For Malnourished Children and Their Parents JournalroulyrosdianiNo ratings yet
- BMC Oralhealth 1Document24 pagesBMC Oralhealth 1Eliza DNNo ratings yet
- Research ArticleDocument8 pagesResearch ArticleDennis MejiaNo ratings yet
- Oral Health LiteracyDocument7 pagesOral Health Literacyhairun hairunNo ratings yet
- 2016RAHELEHDocument8 pages2016RAHELEHDennis MejiaNo ratings yet
- Intention and Oral Health Behavior Perspective of Islamic Traditional Boarding School Students Based On Theory of Planned BehaviorDocument8 pagesIntention and Oral Health Behavior Perspective of Islamic Traditional Boarding School Students Based On Theory of Planned BehaviorIlham Maulana Naufal NugratamaNo ratings yet
- Heber David Lopez ColmanDocument3 pagesHeber David Lopez ColmanHeber LopezNo ratings yet
- Sample ThesisDocument46 pagesSample ThesisRaj Subedi100% (1)
- Assessment of Knowledge Attitude and Practice of Oral Habits Among Health Care ProfessionalsDocument8 pagesAssessment of Knowledge Attitude and Practice of Oral Habits Among Health Care ProfessionalsKrishna KadamNo ratings yet
- Cmmty DXDocument125 pagesCmmty DXReine Chiara B. ConchaNo ratings yet
- Devina 1 StshorttermDocument4 pagesDevina 1 StshorttermAamirNo ratings yet
- The Impact of Oral Health Education On The Oral Health Literacy and Oral Hygiene Status of Literate Elderly, Person in Ileife NigeriaDocument62 pagesThe Impact of Oral Health Education On The Oral Health Literacy and Oral Hygiene Status of Literate Elderly, Person in Ileife Nigeriajamessabraham2No ratings yet
- Articulo OdontopediatriaDocument8 pagesArticulo OdontopediatriaEvelyn RiveraNo ratings yet
- Factors Affecting ParentDocument15 pagesFactors Affecting ParentAlfanIndraNo ratings yet
- Rajiv Gandhi University of Health Sciences Karnataka, Bangalore Annexure - IDocument11 pagesRajiv Gandhi University of Health Sciences Karnataka, Bangalore Annexure - IMatthew RiveraNo ratings yet
- Healthy Teens Counseling ApproachDocument6 pagesHealthy Teens Counseling ApproachDebbie CharlotteNo ratings yet
- 13 SummaryDocument21 pages13 Summaryamit.dasNo ratings yet
- An Investigation On The Effect of Gastric Cancer Education Based On Health Belief Model On Knowledge, Attitude and Nutritional Practice of HousewivesDocument12 pagesAn Investigation On The Effect of Gastric Cancer Education Based On Health Belief Model On Knowledge, Attitude and Nutritional Practice of Housewivesnotrie kristineNo ratings yet
- 2 Oral Care in All YearsDocument10 pages2 Oral Care in All Yearsneetika guptaNo ratings yet
- Orh IDJ KAP Adults ChinaDocument11 pagesOrh IDJ KAP Adults ChinamutiaNo ratings yet
- A Survey On Oral Health Attitude, Awareness and Behaviour of Dental StudentsDocument5 pagesA Survey On Oral Health Attitude, Awareness and Behaviour of Dental StudentsazizahNo ratings yet
- Self-Assessment of Psychological and Mechanical Factors Affecting Oral Hygiene Among Indian College-Going Students: A Model-Guided StudyDocument9 pagesSelf-Assessment of Psychological and Mechanical Factors Affecting Oral Hygiene Among Indian College-Going Students: A Model-Guided StudyAamirNo ratings yet
- Knowledge, Attitude and Practice of Oral Health Promoting Factors Among Caretakers of Children Attending Day-Care Centers in Kubang Kerian, Malaysian A Preliminary StudyDocument2 pagesKnowledge, Attitude and Practice of Oral Health Promoting Factors Among Caretakers of Children Attending Day-Care Centers in Kubang Kerian, Malaysian A Preliminary StudyUniversity Malaya's Dental Sciences ResearchNo ratings yet
- Articulo 2 YogaDocument23 pagesArticulo 2 Yogasjhg13No ratings yet
- Sex Education in TeenagersDocument20 pagesSex Education in TeenagersAman RajNo ratings yet
- Oral Health ChineseDocument9 pagesOral Health ChineseNeagu EmaNo ratings yet
- Oral Health EducationDocument7 pagesOral Health EducationfeNo ratings yet
- Relationship Between Perception of Oral Health, Clinical Conditions and Socio-Behavioral Factors of Mother-ChildDocument9 pagesRelationship Between Perception of Oral Health, Clinical Conditions and Socio-Behavioral Factors of Mother-ChildhalidadwiNo ratings yet
- SummaryDocument2 pagesSummaryRirien Triana SuhaeliNo ratings yet
- Bennadi2014 PDFDocument5 pagesBennadi2014 PDFNita Sofia RakhmawatiNo ratings yet
- SisayDocument9 pagesSisaysisayNo ratings yet
- Research IndividualDocument7 pagesResearch IndividualqilahninaNo ratings yet
- 27Document11 pages27Amit TamboliNo ratings yet
- Oral Health Status Among Children Between The Ages of 12 and 15 Attending Government and Private School Systems in Bareilly CityDocument11 pagesOral Health Status Among Children Between The Ages of 12 and 15 Attending Government and Private School Systems in Bareilly CityAthenaeum Scientific PublishersNo ratings yet
- A Study of The Prevalence of Self-Medication Practice Among University Students in Southwestern NigeriaDocument7 pagesA Study of The Prevalence of Self-Medication Practice Among University Students in Southwestern NigeriaGVNo ratings yet
- Scientific Articles: 1. Dalius Petrauskas, Janina Petkeviciene, Jurate Klumbiene, Jolanta SiudikieneDocument8 pagesScientific Articles: 1. Dalius Petrauskas, Janina Petkeviciene, Jurate Klumbiene, Jolanta SiudikieneChandra Sekhar ThatimatlaNo ratings yet
- PS PresentationDocument44 pagesPS PresentationSree LathaNo ratings yet
- Thesis ProposalDocument3 pagesThesis ProposalMemoryNehyebanNo ratings yet
- Eslam I PourDocument9 pagesEslam I PourzumyNo ratings yet
- JurnalDocument20 pagesJurnalRAFLESIA CESITANo ratings yet
- Dental Health Status and Oral Health Behavior Among University Students From Five ASEAN CountriesDocument11 pagesDental Health Status and Oral Health Behavior Among University Students From Five ASEAN CountriesAamirNo ratings yet
- Oral Hygiene Status, Knowledge, Perceptions and Practices Among School Settings in Rural South IndiaDocument9 pagesOral Hygiene Status, Knowledge, Perceptions and Practices Among School Settings in Rural South IndiaClaypella MaskNo ratings yet
- Knowledge, Attitude, and Practices of Anganwadi Workers Regarding Oral Health of Children in Virajpet TalukDocument6 pagesKnowledge, Attitude, and Practices of Anganwadi Workers Regarding Oral Health of Children in Virajpet TalukEka PratiwiNo ratings yet
- The Application of The Health Belief Model in Oral Health EducationDocument7 pagesThe Application of The Health Belief Model in Oral Health EducationemeraldwxyzNo ratings yet
- Balayan National High School: Awareness of Individuals On The Health Policies Group 4Document31 pagesBalayan National High School: Awareness of Individuals On The Health Policies Group 4Purple ShinesNo ratings yet
- Fadila Kemala Dwi Ramadhani Ruslan - Revisi Kbpji 2Document16 pagesFadila Kemala Dwi Ramadhani Ruslan - Revisi Kbpji 2Eugenia RussiavNo ratings yet
- DefenseDocument188 pagesDefenseFrancia Toledano82% (11)
- Article WJPR 1441008248Document11 pagesArticle WJPR 1441008248neetika guptaNo ratings yet
- Journal of Health EducationDocument10 pagesJournal of Health Educationfenska frianaNo ratings yet
- Relationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationFrom EverandRelationship Between Health Literacy Scores and Patient Use of the iPET for Patient EducationNo ratings yet
- Pharmacodynamics and PharmacokineticsDocument99 pagesPharmacodynamics and PharmacokineticsMAMA LALANo ratings yet
- Introduction To Statistics: Marina Topuridze MD, MSDocument41 pagesIntroduction To Statistics: Marina Topuridze MD, MSMAMA LALANo ratings yet
- Data Collection And: ManagementDocument76 pagesData Collection And: ManagementMAMA LALANo ratings yet
- History of Scientific Research: Marina TopuridzeDocument29 pagesHistory of Scientific Research: Marina TopuridzeMAMA LALANo ratings yet
- Analytic Research Methods: Marina Topuridze L. Sakvarelidze National Center For Disease Control & Public HealthDocument21 pagesAnalytic Research Methods: Marina Topuridze L. Sakvarelidze National Center For Disease Control & Public HealthMAMA LALANo ratings yet
- Descriptive Research Methods: Marina TopuridzeDocument27 pagesDescriptive Research Methods: Marina TopuridzeMAMA LALANo ratings yet
- Hand and Wrist InjuriesDocument25 pagesHand and Wrist InjuriesMAMA LALA100% (2)
- Research Ethics: Marina Topuridze MD, MSDocument28 pagesResearch Ethics: Marina Topuridze MD, MSMAMA LALANo ratings yet
- Forearm Traumatic Injuries Lecture 6Document16 pagesForearm Traumatic Injuries Lecture 6MAMA LALANo ratings yet
- Hiatal Hernia: BY Sojobi Akeem OladimejiDocument16 pagesHiatal Hernia: BY Sojobi Akeem OladimejiMAMA LALANo ratings yet
- Traumatology and Orthopedics Diagnostic Methods, ExaminationDocument2 pagesTraumatology and Orthopedics Diagnostic Methods, ExaminationMAMA LALANo ratings yet
- Forensic MedicineDocument3 pagesForensic MedicineMAMA LALANo ratings yet
- Test in General Therapy: Correct Answers)Document42 pagesTest in General Therapy: Correct Answers)MAMA LALANo ratings yet
- Hiatal HerniaDocument13 pagesHiatal HerniaMAMA LALANo ratings yet
- Ophthalmology 11Document40 pagesOphthalmology 11MAMA LALANo ratings yet
- Eyelids Diseases Lacrimal System DiseasesDocument45 pagesEyelids Diseases Lacrimal System DiseasesMAMA LALANo ratings yet
- Damage Control SurgeryDocument68 pagesDamage Control SurgeryMAMA LALANo ratings yet
- Hiv and Aids: ID Specialist Tamar KhuchuaDocument84 pagesHiv and Aids: ID Specialist Tamar KhuchuaMAMA LALANo ratings yet
- Chest TraumaDocument175 pagesChest TraumaMAMA LALANo ratings yet
- Articles of Association: VedtægterDocument107 pagesArticles of Association: Vedtægterrohit_wade1579No ratings yet
- Toxicon: Case ReportDocument6 pagesToxicon: Case ReportBrando SaenzNo ratings yet
- Occlusal Splints and Temporomandibular Disorders: Why, When, How?Document5 pagesOcclusal Splints and Temporomandibular Disorders: Why, When, How?blogger bloggerNo ratings yet
- Fam HNDocument6 pagesFam HNHafizuddin RazidNo ratings yet
- Prenatal Care: Dr. Ruby E Robiso, Fpogs Davao Medical School Foundation, IncDocument33 pagesPrenatal Care: Dr. Ruby E Robiso, Fpogs Davao Medical School Foundation, IncISFAHAN MASULOTNo ratings yet
- Introduction To Patient Centred Communication 20-21Document16 pagesIntroduction To Patient Centred Communication 20-21Ngetwa TzDe TheWirymanNo ratings yet
- Mental Health Nursing.: Lesson 1Document177 pagesMental Health Nursing.: Lesson 1Eng Steve WairuaNo ratings yet
- Blood Research and DisordersDocument5 pagesBlood Research and Disordersdr_joe23No ratings yet
- Sodium Bicarbonate HandoutDocument2 pagesSodium Bicarbonate HandoutChris WoodsNo ratings yet
- Assignment 1Document12 pagesAssignment 1IELTSNo ratings yet
- Ganser Syndrome: A Case Report From ThailandDocument4 pagesGanser Syndrome: A Case Report From ThailandYuyun Ayu ApriyantiNo ratings yet
- Cues Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals and Objectives Intervention Rationale EvaluationCarmina DinerosNo ratings yet
- Medical Triage: Code Tags and Triage TerminologyDocument5 pagesMedical Triage: Code Tags and Triage TerminologyAnna Mae SuminguitNo ratings yet
- Moving Stories - Chennai IEATSDocument14 pagesMoving Stories - Chennai IEATSAnshuma KshetrapalNo ratings yet
- Voucher No: 125244/2023 - 30/03/2023: Reference No. For The Hotel: 9153573473984 / 1484479948Document4 pagesVoucher No: 125244/2023 - 30/03/2023: Reference No. For The Hotel: 9153573473984 / 1484479948Григорий ПавловNo ratings yet
- Additional Interview QuestionsDocument3 pagesAdditional Interview Questionsapi-347153077No ratings yet
- Anthracnose Disease of Walnut - A ReviewDocument9 pagesAnthracnose Disease of Walnut - A ReviewIJEAB JournalNo ratings yet
- Individual Drug ResponseDocument18 pagesIndividual Drug ResponseIlham rianda100% (1)
- Taylor Wallach ResumenewDocument3 pagesTaylor Wallach Resumenewapi-543526848No ratings yet
- Save Lives, Save Limbs (Compressed)Document239 pagesSave Lives, Save Limbs (Compressed)Jon100% (2)
- International Public Safety Association InfoBrief TECC V TCCCDocument16 pagesInternational Public Safety Association InfoBrief TECC V TCCCepraetorianNo ratings yet
- Gap Analysis ISO 8836 2019Document27 pagesGap Analysis ISO 8836 2019suman50% (2)
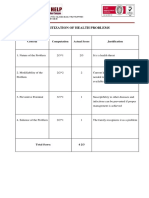
- Prioritization of Health Problems: ParenthoodDocument3 pagesPrioritization of Health Problems: ParenthoodMariana Mikaela AlagarNo ratings yet
- PharmacologyDocument84 pagesPharmacologyhenrydycoco100% (1)
- Endometrial Cancer LDocument26 pagesEndometrial Cancer Lapi-19916399No ratings yet
- Lactic Acid Fermentation of Human Excreta For Agr-Wageningen University and Research 401835Document225 pagesLactic Acid Fermentation of Human Excreta For Agr-Wageningen University and Research 401835Luis Enrique Ortega SalinasNo ratings yet
- 1St Body Measurement IndexDocument68 pages1St Body Measurement IndexHannahclaire DelacruzNo ratings yet
- Disciplines and Ideas in The Applied Social Sciences: Quarter1-Week 2-Module 5Document8 pagesDisciplines and Ideas in The Applied Social Sciences: Quarter1-Week 2-Module 5Lyka Mae Sembrero100% (3)