Download as pdf or txt
You might also like
- Positive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaDocument10 pagesPositive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaElfina NataliaNo ratings yet
- HiTEMP TrialDocument8 pagesHiTEMP TrialJorge BarriosNo ratings yet
- Jurnal Tugas Juga 2016 (Ceftriaxone, Ertapenem and Levofloxacin)Document6 pagesJurnal Tugas Juga 2016 (Ceftriaxone, Ertapenem and Levofloxacin)Aulia RahmahhNo ratings yet
- Allou 2018Document7 pagesAllou 2018jq4rhbh2pzNo ratings yet
- 06 2010 Jun Central-Venous-CatheterDocument6 pages06 2010 Jun Central-Venous-CatheterFrancisco VigenorNo ratings yet
- Major HAI TypesDocument73 pagesMajor HAI Typeschotu7272jhaNo ratings yet
- Jurnal VentilasiDocument10 pagesJurnal Ventilasiarif21492No ratings yet
- Brevundimonas Vesicularis Bacteremia Resistant To Trimethoprim-Sulfamethoxazole and Ceftazidime in A Tertiary Hospital in Southern TaiwanDocument5 pagesBrevundimonas Vesicularis Bacteremia Resistant To Trimethoprim-Sulfamethoxazole and Ceftazidime in A Tertiary Hospital in Southern TaiwanSihome ThodireNo ratings yet
- Catheter-Associated Urinary Tract Infection in A Surgical Intensive Care UnitDocument6 pagesCatheter-Associated Urinary Tract Infection in A Surgical Intensive Care UnitYuko Dwi ApriantoNo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- Control of Hospital Acquired Infections in The ICU: A Service PerspectiveDocument5 pagesControl of Hospital Acquired Infections in The ICU: A Service PerspectiveAndriyanto HermawanNo ratings yet
- Association Between Prophylactic Antibiotic Use For Transarterial Chemoembolization and Occurrence of Liver Abscess - A Retrospective Cohort StudyDocument6 pagesAssociation Between Prophylactic Antibiotic Use For Transarterial Chemoembolization and Occurrence of Liver Abscess - A Retrospective Cohort StudyCory Artika ManurungNo ratings yet
- Intravesical Gentamicin For Recurrent Urinary Tract Infection in Patients WithDocument6 pagesIntravesical Gentamicin For Recurrent Urinary Tract Infection in Patients WithChristianne Fernandes Valente TakedaNo ratings yet
- Jurnal Kritis ICU Bundle Vap PneumoniaDocument6 pagesJurnal Kritis ICU Bundle Vap PneumoniaAdzkia PintaNo ratings yet
- Intrathecal Antibiotic Administration Procedure (Paediatrics)Document9 pagesIntrathecal Antibiotic Administration Procedure (Paediatrics)Abu Azzam Al-HadiNo ratings yet
- Eviden Base PPT (Latest)Document34 pagesEviden Base PPT (Latest)ZulaikaAJNo ratings yet
- Prolonged Viral Shedding in A Lymphoma Patient WitDocument2 pagesProlonged Viral Shedding in A Lymphoma Patient WitDwi Rachma Cahyati 06No ratings yet
- Manuscript - Umbilical Cord Mesenchymal Stromal Cells As Critical COVID-19 Adjuvant Therapy - A Randomized Controlled TrialDocument9 pagesManuscript - Umbilical Cord Mesenchymal Stromal Cells As Critical COVID-19 Adjuvant Therapy - A Randomized Controlled TrialZara AkbariNo ratings yet
- Impact of Time To Antibiotic Therapy On Clinical Outcome I 2021 Clinical MicDocument7 pagesImpact of Time To Antibiotic Therapy On Clinical Outcome I 2021 Clinical MicSusanyi ErvinNo ratings yet
- JCDR 10 SC06Document6 pagesJCDR 10 SC06YANNo ratings yet
- Outcome and Clinical Characteristics of Nosocomial Infection in Adult Patients Undergoing Extracorporeal Membrane OxygenationDocument11 pagesOutcome and Clinical Characteristics of Nosocomial Infection in Adult Patients Undergoing Extracorporeal Membrane OxygenationGilberto Díaz PérezNo ratings yet
- Ppi Di Ruang Perawatan IntensiveDocument56 pagesPpi Di Ruang Perawatan IntensiveapeepowNo ratings yet
- Targeting Zero Catheter-Related Bloodstream Infections in Pediatric Intensive Care Unit: A Retrospective Matched Case-Control StudyDocument6 pagesTargeting Zero Catheter-Related Bloodstream Infections in Pediatric Intensive Care Unit: A Retrospective Matched Case-Control StudyJhonny MarquezNo ratings yet
- Effectiveness and Safety of Cefazolin Versus Cloxacillin in Endocarditis Due ToDocument9 pagesEffectiveness and Safety of Cefazolin Versus Cloxacillin in Endocarditis Due Toanna531No ratings yet
- NIH Public Access: Author ManuscriptDocument9 pagesNIH Public Access: Author ManuscriptCaro ArduzoNo ratings yet
- 1 s2.0 S2214751921001584 MainDocument7 pages1 s2.0 S2214751921001584 MainfitriNo ratings yet
- Jti 32 3 150Document7 pagesJti 32 3 150ameliaNo ratings yet
- Chichra Et Al 2023 Managing The Chronically Ventilated CriticallyDocument12 pagesChichra Et Al 2023 Managing The Chronically Ventilated CriticallyCarolina LassoNo ratings yet
- Hubungan Perawatan Catheter Vena Central (CVC) Terhadap Terjadinya Infeksi Aliran Darah Primer (Iadp)Document9 pagesHubungan Perawatan Catheter Vena Central (CVC) Terhadap Terjadinya Infeksi Aliran Darah Primer (Iadp)Leriani NaibahoNo ratings yet
- Clinical Nutrition: Micha Ł Ławinski, Krystyna Majewska, Łukasz Gradowski, Iwona Fo Łtyn, Pierre SingerDocument5 pagesClinical Nutrition: Micha Ł Ławinski, Krystyna Majewska, Łukasz Gradowski, Iwona Fo Łtyn, Pierre SingerBby AdelinaNo ratings yet
- Annual Epidemiological Report For 2019-Associated-Infections-Intensive-Care-Units-Annual-Epidemiological-Report-2019Document14 pagesAnnual Epidemiological Report For 2019-Associated-Infections-Intensive-Care-Units-Annual-Epidemiological-Report-2019Edson MarquesNo ratings yet
- Infectious Diseases I: Eric W. Mueller, Pharm.D., FCCP, FCCMDocument52 pagesInfectious Diseases I: Eric W. Mueller, Pharm.D., FCCP, FCCMNhanLiNo ratings yet
- Nebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaDocument4 pagesNebulized Colistin in The Treatment of Pneumonia Due To Multidrug-Resistant Acinetobacter Baumannii and Pseudomonas AeruginosaPhan Tấn TàiNo ratings yet
- BJBMS 14 227Document7 pagesBJBMS 14 227enesNo ratings yet
- Lancet Emed Covid Stemcell ArticleDocument9 pagesLancet Emed Covid Stemcell ArticleShanmuga SundaramNo ratings yet
- Central Line Associated Bloodstream Infection in Adult Intensive Care Unit PopulationDocument29 pagesCentral Line Associated Bloodstream Infection in Adult Intensive Care Unit PopulationMargarida ReisNo ratings yet
- Kerangka Acuan PPIDocument66 pagesKerangka Acuan PPIdedyNo ratings yet
- Artigo 2 InglesDocument6 pagesArtigo 2 InglesbeatrizxavierNo ratings yet
- The Clinical Impact of Ventilator-Associated Events - Zhu2015Document8 pagesThe Clinical Impact of Ventilator-Associated Events - Zhu2015Maxi BoniniNo ratings yet
- Management of Septic Shock in An Intermediate Care UnitDocument20 pagesManagement of Septic Shock in An Intermediate Care UnitJHNo ratings yet
- Karapanou 2020Document7 pagesKarapanou 2020pelayananmedisNo ratings yet
- Bactibilia in ColecystitisDocument6 pagesBactibilia in Colecystitiscarlos.alberto.palacios.serratNo ratings yet
- Implementation of A Non-Invasive Oxygenation Support Strategy During The COVID-19 Pandemic in An Ephemeral Respiratory Intermediate Care UnitDocument3 pagesImplementation of A Non-Invasive Oxygenation Support Strategy During The COVID-19 Pandemic in An Ephemeral Respiratory Intermediate Care UnitJHNo ratings yet
- PJI NEJMoa2020198Document11 pagesPJI NEJMoa2020198dwi.and1989No ratings yet
- Usage of Antibiotics in ICU (English)Document13 pagesUsage of Antibiotics in ICU (English)V15CERA FK UNANDNo ratings yet
- Central Venous Catheter-Associated Bloodstream Infections in A Pediatric Intensive Care Unit: Effect of The Location of Catheter InsertionDocument5 pagesCentral Venous Catheter-Associated Bloodstream Infections in A Pediatric Intensive Care Unit: Effect of The Location of Catheter InsertionLeroy ColeNo ratings yet
- Antibiotics 10 00608Document10 pagesAntibiotics 10 00608Marketable StudioNo ratings yet
- 1 s2.0 S2589537023000573 MainDocument11 pages1 s2.0 S2589537023000573 MainSadia MacavilcaNo ratings yet
- Meningitis Guias Americanas 2004Document18 pagesMeningitis Guias Americanas 2004Luis Diego López ManjarresNo ratings yet
- HC610-00-UK BALLARD Mini-BAL SelectedEvidenceBooklet COPY-05459 2021Document20 pagesHC610-00-UK BALLARD Mini-BAL SelectedEvidenceBooklet COPY-05459 2021Popescu ValiNo ratings yet
- Bacterial Meningitis Guidelines IDSADocument18 pagesBacterial Meningitis Guidelines IDSAAldito GlasgowNo ratings yet
- PICC-associated Bloodstream Infections PrevalenceDocument10 pagesPICC-associated Bloodstream Infections PrevalenceAne MartinezNo ratings yet
- RCT AppraisalDocument4 pagesRCT AppraisalmahnumaNo ratings yet
- Guideline Update For The Management of Intravascular Catheter-Related InfectionsDocument47 pagesGuideline Update For The Management of Intravascular Catheter-Related InfectionsTài NguyễnNo ratings yet
- Multiplex PCR Severe PneumoniaDocument13 pagesMultiplex PCR Severe PneumoniaSrinivas PingaliNo ratings yet
- Revista Brasileira DE AnestesiologiaDocument7 pagesRevista Brasileira DE AnestesiologiaPutriRahayuMoidadyNo ratings yet
- Inhalatory and Intravenous Colistin in Treating Ventilator-Associated Pneumonia Due To Acinetobacter Species: Should We Combine Them?Document8 pagesInhalatory and Intravenous Colistin in Treating Ventilator-Associated Pneumonia Due To Acinetobacter Species: Should We Combine Them?Hendy SetiadyNo ratings yet
- 0221 Community-Acquired-PneumoniaDocument29 pages0221 Community-Acquired-PneumoniaDiego YanezNo ratings yet
- 1 s2.0 S1201971223000255 MainDocument12 pages1 s2.0 S1201971223000255 MainArie RahadiNo ratings yet
- The Conceptualisation of Weather As A Career MetaphorDocument14 pagesThe Conceptualisation of Weather As A Career MetaphorLizet SantacruzNo ratings yet
- Make It Hot. How Food Temperature (Mis) Guides Product Judgments.Document22 pagesMake It Hot. How Food Temperature (Mis) Guides Product Judgments.Lizet SantacruzNo ratings yet
- The Christianisation of Western Baetica. Architecture, Power and Religion in A Late Antique LandscapeDocument4 pagesThe Christianisation of Western Baetica. Architecture, Power and Religion in A Late Antique LandscapeLizet SantacruzNo ratings yet
- New Decade, New Directions. Advancing The Study of Southeast Asian ReligionsDocument29 pagesNew Decade, New Directions. Advancing The Study of Southeast Asian ReligionsLizet SantacruzNo ratings yet
- Problems of Axiomatizing ReligionDocument16 pagesProblems of Axiomatizing ReligionLizet SantacruzNo ratings yet
- Climate Change and The Criminal Justice System.Document50 pagesClimate Change and The Criminal Justice System.Lizet SantacruzNo ratings yet
- Aprendizaje Significativo de Ausubel y Segregación EducativaDocument20 pagesAprendizaje Significativo de Ausubel y Segregación EducativaLizet SantacruzNo ratings yet
- Full Ebook of Textbook of Tuberculosis and Nontuberculousis Mycobacterial Diseases 3Rd Edition K Surendra Sharma Online PDF All ChapterDocument70 pagesFull Ebook of Textbook of Tuberculosis and Nontuberculousis Mycobacterial Diseases 3Rd Edition K Surendra Sharma Online PDF All Chaptersteventimmerman197670100% (5)
- Epilepsi Paska StrokeDocument5 pagesEpilepsi Paska StrokerifaiNo ratings yet
- MCQ Dermatology (Dr. Asaf K.)Document31 pagesMCQ Dermatology (Dr. Asaf K.)Dinesh JadhavNo ratings yet
- Ordiales PSG 2nd DraftDocument4 pagesOrdiales PSG 2nd DraftpearlNo ratings yet
- Health 9 Q2 WK3Document5 pagesHealth 9 Q2 WK3Rojegarmil LagoNo ratings yet
- GEE301-Activity 2 Human Sexuality InfographicsDocument1 pageGEE301-Activity 2 Human Sexuality InfographicsVohn Archie EdjanNo ratings yet
- Notice: La ( K@ Fnukad@Document2 pagesNotice: La ( K@ Fnukad@JyotiVinay SethNo ratings yet
- Plan of Care Implementation Third Module ExamDocument6 pagesPlan of Care Implementation Third Module ExamVasuNo ratings yet
- Intra PartumDocument332 pagesIntra PartumOcha ManisNo ratings yet
- Academic Stress and Grade 12 Notre Dame of Cotabato STEM Students' Academic PerformanceDocument43 pagesAcademic Stress and Grade 12 Notre Dame of Cotabato STEM Students' Academic PerformanceJacob RoalesNo ratings yet
- K To 12 CurriculumDocument75 pagesK To 12 Curriculumrevertlyn86% (7)
- A Qualitative Study of The Psychological Impact of Unemployment o PDFDocument65 pagesA Qualitative Study of The Psychological Impact of Unemployment o PDFHan Ya Da100% (1)
- Learning Continuity Plans For Alternative Learning System 2Document10 pagesLearning Continuity Plans For Alternative Learning System 2Rachel Sismaet PadillaNo ratings yet
- Classroom Culture and Climate:: Plan For Managing The Learning EnvironmentDocument18 pagesClassroom Culture and Climate:: Plan For Managing The Learning Environmentapi-663673275No ratings yet
- Six Sigma Project WorkDocument34 pagesSix Sigma Project WorkDrpallavi NanavatiNo ratings yet
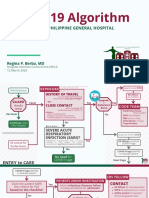
- COVID-19 Algorithm: For The Philippine General HospitalDocument10 pagesCOVID-19 Algorithm: For The Philippine General HospitalJay VeeNo ratings yet
- Unit 5 Factors Affecting The Health Care SystemDocument29 pagesUnit 5 Factors Affecting The Health Care SystemDana kristenNo ratings yet
- Positive Psychology - ThrivingDocument18 pagesPositive Psychology - ThrivingStephen CochraneNo ratings yet
- Pathology of Nutritional DisordersDocument15 pagesPathology of Nutritional DisordersbumfromjerseyNo ratings yet
- Preparing For A Birth: How To Use The GuideDocument42 pagesPreparing For A Birth: How To Use The GuideZimm RrrrNo ratings yet
- Family With An Infant (Group 3)Document12 pagesFamily With An Infant (Group 3)Jessa Mae OhaoNo ratings yet
- Theoretical Framework - Negative Effect of SmokingDocument1 pageTheoretical Framework - Negative Effect of SmokingStevezkie Onii-chanNo ratings yet
- ICT2300 Work Immersion (ALL STRAND) Graded Items For College Success WEWODocument10 pagesICT2300 Work Immersion (ALL STRAND) Graded Items For College Success WEWOAndrea NombreNo ratings yet
- NCP EdDocument5 pagesNCP EdChristine Claire CaguimbayNo ratings yet
- Eosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportDocument5 pagesEosinophilic Granulomatosis With Polyangiitis and Bowel Perforation: Case ReportSabrina JonesNo ratings yet
- Mahkota Dewa Plus: Siti Nadhirah Binti MD Shamsull BahriDocument12 pagesMahkota Dewa Plus: Siti Nadhirah Binti MD Shamsull BahriDhyra ShamsullNo ratings yet
- Uti Data SheetDocument14 pagesUti Data SheetStudio 12No ratings yet
- 6-2 HealthDocument2 pages6-2 HealthEdu DulnethNo ratings yet
- Pharmacology For The Primary Care Provider 4th Edition Edmunds Test BankDocument35 pagesPharmacology For The Primary Care Provider 4th Edition Edmunds Test Bankalomancyheriot.o7m4100% (31)
- IQVIA Institute Biosimilar Shared Savings Programs in Europe 12-22 ForwebDocument44 pagesIQVIA Institute Biosimilar Shared Savings Programs in Europe 12-22 Forwebخالد العشريNo ratings yet