Download as pdf or txt
You might also like
- Chapter 16: Fluid, Electrolyte, and Acid-Base Imbalances Harding: Lewis's Medical-Surgical Nursing, 11th EditionDocument13 pagesChapter 16: Fluid, Electrolyte, and Acid-Base Imbalances Harding: Lewis's Medical-Surgical Nursing, 11th EditionKrishna RamaNo ratings yet
- Chiropractic - Management - of - Pubic - Symphysis - Shear - in Overactive BladderDocument10 pagesChiropractic - Management - of - Pubic - Symphysis - Shear - in Overactive BladderDenise MathreNo ratings yet
- IJETR022854Document7 pagesIJETR022854erpublicationNo ratings yet
- Caldwell2013review Nocturnal EnuresisDocument6 pagesCaldwell2013review Nocturnal EnuresisBogdan Neamtu100% (1)
- Epilepsy 3 PDFDocument14 pagesEpilepsy 3 PDFfikaNo ratings yet
- Chiropractic Management of Pubic Symphysis Shear Dysfunction in A Patient With Overactive BladderDocument9 pagesChiropractic Management of Pubic Symphysis Shear Dysfunction in A Patient With Overactive BladderTameemNo ratings yet
- Urogenital Symptoms in Neurologic Patients.14Document20 pagesUrogenital Symptoms in Neurologic Patients.14Fawad JanNo ratings yet
- Relapse in Anorexia NervosaDocument12 pagesRelapse in Anorexia Nervosacharoline gracetiani nataliaNo ratings yet
- Article 1576845020 PDFDocument5 pagesArticle 1576845020 PDFFatima Habib JajjaNo ratings yet
- Clinical Pharmacy TherapeuticDocument9 pagesClinical Pharmacy TherapeuticApple StarNo ratings yet
- An International Continence Society (ICS) Report On The Terminology For Adult Neurogenic Lower Urinary Tract Dysfunction (ANLUTD)Document10 pagesAn International Continence Society (ICS) Report On The Terminology For Adult Neurogenic Lower Urinary Tract Dysfunction (ANLUTD)g7ccbb2pw9No ratings yet
- Neonatal Seizures: Incidence, Etiologies, Clinical Features and EEG Findings in The Neonatal Intensive Care UnitDocument5 pagesNeonatal Seizures: Incidence, Etiologies, Clinical Features and EEG Findings in The Neonatal Intensive Care UnitDoraemon BiruNo ratings yet
- WJN 5 224 PDFDocument10 pagesWJN 5 224 PDFTisna WennyNo ratings yet
- Ann Neonatol J 2021 - Effect of Phototherapy On Cardiac Functions in Neonates With Hyperbilirrubinemia. A Prospective Cross-Sectional StudyDocument19 pagesAnn Neonatol J 2021 - Effect of Phototherapy On Cardiac Functions in Neonates With Hyperbilirrubinemia. A Prospective Cross-Sectional StudyCharlie CharcapeNo ratings yet
- Segar 2021Document9 pagesSegar 2021I SakinNo ratings yet
- Seminars in Fetal and Neonatal MedicineDocument9 pagesSeminars in Fetal and Neonatal MedicineI SakinNo ratings yet
- Vejiga Neurogenica PDFDocument9 pagesVejiga Neurogenica PDFAMENDBENo ratings yet
- Consultation in Neurourology: A Practical Evidence-Based GuideFrom EverandConsultation in Neurourology: A Practical Evidence-Based GuideNo ratings yet
- Vagus Nerve Stimulation in The Treatment of Drug Resistant Epilepsy in 29 Children 2016 European Journal of Paediatric NeurologyDocument6 pagesVagus Nerve Stimulation in The Treatment of Drug Resistant Epilepsy in 29 Children 2016 European Journal of Paediatric NeurologyZeptalanNo ratings yet
- Noradrenalina en PrematurosDocument7 pagesNoradrenalina en PrematurosnzunaNo ratings yet
- Epilepsy in Children With Shunted HydrocephalusDocument16 pagesEpilepsy in Children With Shunted HydrocephalusPauleen Trisha SamparaniNo ratings yet
- Obstructive Sleep Apnea in Adults 10.1056@NEJMcp1816152Document8 pagesObstructive Sleep Apnea in Adults 10.1056@NEJMcp1816152Samuel Fraga SalvadorNo ratings yet
- Betel Nut Chewing and The Risk of Chronic Kidney Disease: Evidence From A Meta AnalysisDocument8 pagesBetel Nut Chewing and The Risk of Chronic Kidney Disease: Evidence From A Meta AnalysisAaron Paul BernasNo ratings yet
- Medi 102 E32377Document10 pagesMedi 102 E32377Duda ShiraiwaNo ratings yet
- Adult Obstructive Sleep Apnea: January 2014Document13 pagesAdult Obstructive Sleep Apnea: January 2014giulio pinnolaNo ratings yet
- Hiperlazie Adrenala CongenitalaDocument11 pagesHiperlazie Adrenala CongenitalaClaudia IrimieNo ratings yet
- New Developments in Epilepsy ManagmentDocument6 pagesNew Developments in Epilepsy ManagmentSantiago Chávez BolañosNo ratings yet
- Fneur 13 823189Document11 pagesFneur 13 823189AlexandreNo ratings yet
- Seminar: Amy S Jordan, David G Mcsharry, Atul MalhotraDocument12 pagesSeminar: Amy S Jordan, David G Mcsharry, Atul MalhotraSerkan KüçüktürkNo ratings yet
- Apnea After Awake Regional and General Anesthesia in InfantsDocument17 pagesApnea After Awake Regional and General Anesthesia in InfantsmluthfidunandNo ratings yet
- Consequences of OSADocument11 pagesConsequences of OSAhammodihotmailcomNo ratings yet
- PIIS0085253817308104Document3 pagesPIIS0085253817308104Freddy Shanner Chávez VásquezNo ratings yet
- Neurogenic BladderDocument8 pagesNeurogenic BladderrafendyfendyNo ratings yet
- NIH Public Access: Author ManuscriptDocument12 pagesNIH Public Access: Author ManuscriptadipurnamiNo ratings yet
- 10 1016@j Ejogrb 2015 09 020Document5 pages10 1016@j Ejogrb 2015 09 020samuel tapia pardoNo ratings yet
- 1 s2.0 S2589986423000448 MainDocument5 pages1 s2.0 S2589986423000448 MainsoylahijadeunvampiroNo ratings yet
- Pathological Profile and Recovery Rate in Patients With Drug-Induced Acute Kidney Injury: A Retrospective Study From North-East IndiaDocument7 pagesPathological Profile and Recovery Rate in Patients With Drug-Induced Acute Kidney Injury: A Retrospective Study From North-East IndiaIJAR JOURNALNo ratings yet
- DT 200231564Document5 pagesDT 200231564sang ayuNo ratings yet
- Managing Nocturia The Multidisciplinary ApproachDocument7 pagesManaging Nocturia The Multidisciplinary ApproachrhezafirmNo ratings yet
- Acupuncture For Constipation in Patients With Stroke: Protocol of A Systematic Review and Meta-AnalysisDocument5 pagesAcupuncture For Constipation in Patients With Stroke: Protocol of A Systematic Review and Meta-AnalysisYUTRILIANo ratings yet
- A Review of Normal Values of Infant Sleep PolysomnographyDocument6 pagesA Review of Normal Values of Infant Sleep PolysomnographyGil CLNo ratings yet
- IJCRT2107516Document9 pagesIJCRT2107516Jasmine GumandoyNo ratings yet
- Diagnosis and Management of The Epilepsies in Adults and Children: Summary of Updated NICE GuidanceDocument8 pagesDiagnosis and Management of The Epilepsies in Adults and Children: Summary of Updated NICE GuidanceANDREWNo ratings yet
- No Laughing Matter: Subacute Degeneration of The Spinal Cord Due To Nitrous Oxide InhalationDocument7 pagesNo Laughing Matter: Subacute Degeneration of The Spinal Cord Due To Nitrous Oxide InhalationgshjfkNo ratings yet
- Biomarkers of PUJODocument21 pagesBiomarkers of PUJOLatif Ahmad DarNo ratings yet
- Key Answers Part 1 June 2019 PDFDocument15 pagesKey Answers Part 1 June 2019 PDFNimer Abdelhadi AliNo ratings yet
- Annotated VoclosporinDocument11 pagesAnnotated Voclosporinawkjhdjawdhfad wdjalwkdkwjdklwajdNo ratings yet
- Prevalence of Chronic Kidney Disease in Nigeria Systematic - 052118Document8 pagesPrevalence of Chronic Kidney Disease in Nigeria Systematic - 052118Zainab Abubakar GwanduNo ratings yet
- Clinical Diagnostic Criteria For Dementia AssociatDocument20 pagesClinical Diagnostic Criteria For Dementia AssociatAnderson Cassol DozzaNo ratings yet
- Papers 2022Document9 pagesPapers 2022MDrakeNo ratings yet
- Classification Systems in Cerebral PalsyDocument11 pagesClassification Systems in Cerebral PalsyLizza Mora RNo ratings yet
- BMJ l4485 FullDocument16 pagesBMJ l4485 FullJennifer AlmeidaNo ratings yet
- 2019 - 08 - 05 Essential TremorDocument16 pages2019 - 08 - 05 Essential TremorstaseaditNo ratings yet
- The Laboratory Diagnosis of Feline Kidney DiseaseDocument7 pagesThe Laboratory Diagnosis of Feline Kidney DiseaseCabinet VeterinarNo ratings yet
- Fnins 16 968725Document12 pagesFnins 16 968725Felipe GonzálezNo ratings yet
- Clinical Trial of Fluid Infusion Rates For PediatricsDocument14 pagesClinical Trial of Fluid Infusion Rates For PediatricsPatricia Denise Tome MagisaNo ratings yet
- Literature Review Neonatal JaundiceDocument6 pagesLiterature Review Neonatal Jaundiceafdtvdcwf100% (1)
- AnnMovDisord2239-5235143 143231Document9 pagesAnnMovDisord2239-5235143 143231Raul de Sousa RamosNo ratings yet
- Onconephrology 2022 An Update.19Document14 pagesOnconephrology 2022 An Update.19Prakash GudsoorkarNo ratings yet
- Adrenal Disorders: Physiology, Pathophysiology and TreatmentFrom EverandAdrenal Disorders: Physiology, Pathophysiology and TreatmentAlice C. LevineNo ratings yet
- Nocturia: Etiology, Pathology, Risk Factors, Treatment and Emerging TherapiesFrom EverandNocturia: Etiology, Pathology, Risk Factors, Treatment and Emerging TherapiesNo ratings yet
- Explaining History of RomeDocument154 pagesExplaining History of RomeAli HusseinNo ratings yet
- Khalid Alfaki PedDocument21 pagesKhalid Alfaki PedAli HusseinNo ratings yet
- Result of Fmge (Screening Test), June 2021 SessionDocument121 pagesResult of Fmge (Screening Test), June 2021 SessionAli HusseinNo ratings yet
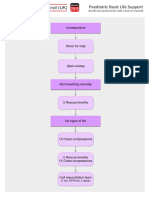
- Paediatric Basic Life Support: UnresponsiveDocument1 pagePaediatric Basic Life Support: UnresponsiveAli HusseinNo ratings yet
- Morning Pharma Dose Day 3Document2 pagesMorning Pharma Dose Day 3Ali HusseinNo ratings yet
- Morning Pharma Dose Day 4Document2 pagesMorning Pharma Dose Day 4Ali HusseinNo ratings yet
- June 2021 MCQ Psychiatry at DAMSDocument61 pagesJune 2021 MCQ Psychiatry at DAMSAli HusseinNo ratings yet
- Paediatric Choking Treatment-A3Document1 pagePaediatric Choking Treatment-A3Ali HusseinNo ratings yet
- Paediatric ALS A3Document1 pagePaediatric ALS A3Ali HusseinNo ratings yet
- Ocs P Screening GuidelinesDocument2 pagesOcs P Screening GuidelinesAli HusseinNo ratings yet
- How To Approach Any Cancer Patient: Levofloxacin)Document2 pagesHow To Approach Any Cancer Patient: Levofloxacin)Ali HusseinNo ratings yet
- Influenza Guideline 2015-16Document28 pagesInfluenza Guideline 2015-16Ali HusseinNo ratings yet
- CHN Pamer Psych Neuro CVD QuizDocument14 pagesCHN Pamer Psych Neuro CVD Quizmendozajanice0601No ratings yet
- Pangpangdeo Shanne Delle B. - Worksheet 5 ArdsDocument7 pagesPangpangdeo Shanne Delle B. - Worksheet 5 ArdsPANGPANGDEO Shanne Delle B.No ratings yet
- Pain PDFDocument10 pagesPain PDFJanaica JuanNo ratings yet
- Responsive Docs - CREW Versus Department of Justice (DOJ) : Regarding Investigation Records of Magliocchetti: 11/12/13 - Part 3Document172 pagesResponsive Docs - CREW Versus Department of Justice (DOJ) : Regarding Investigation Records of Magliocchetti: 11/12/13 - Part 3CREWNo ratings yet
- Autoimmune Diseases A Late Complication of Toxic Epidermal Necrolysis A Case ReportDocument4 pagesAutoimmune Diseases A Late Complication of Toxic Epidermal Necrolysis A Case ReportAthenaeum Scientific PublishersNo ratings yet
- Mushtaq Ahmad: Running Head: REFLECTIVE LOG 1Document5 pagesMushtaq Ahmad: Running Head: REFLECTIVE LOG 1Shafiq Ur RahmanNo ratings yet
- Inistitutional Assessement Knowledge Test For Comprhenssive NursingDocument5 pagesInistitutional Assessement Knowledge Test For Comprhenssive NursingBezawit bekele100% (1)
- Earlys Physical Dysfunction Practice Skills For The Occupational Therapy Assistant 4Th Edition Mary Elizabeth Patnaude Full ChapterDocument68 pagesEarlys Physical Dysfunction Practice Skills For The Occupational Therapy Assistant 4Th Edition Mary Elizabeth Patnaude Full Chapterhubert.drayton798100% (9)
- Pathogenesis of Trigeminal Neuralgia: Neural Regeneration Research June 2014Document2 pagesPathogenesis of Trigeminal Neuralgia: Neural Regeneration Research June 2014FKUPR 2017No ratings yet
- Nejmcps 2304844Document6 pagesNejmcps 2304844AntoineNo ratings yet
- Radiculopathy - WikipediaDocument7 pagesRadiculopathy - WikipediaDalonPetrelNo ratings yet
- NIAAA Alcohol OverdoseDocument3 pagesNIAAA Alcohol OverdoseFrancisco Porá TuzinkievichNo ratings yet
- Chronic Heart Failure (Gagal Jantung Kronik)Document15 pagesChronic Heart Failure (Gagal Jantung Kronik)Grup 9B Viscera tahun 2No ratings yet
- Gnaphalium Polycephalum. - THE GUIDING SYMPTOMS OF OUR MATERIA MEDICA by CONSTANDocument5 pagesGnaphalium Polycephalum. - THE GUIDING SYMPTOMS OF OUR MATERIA MEDICA by CONSTANHarrison DavidsonNo ratings yet
- Eye Bags ReliefDocument27 pagesEye Bags ReliefNatsu DragneelNo ratings yet
- Ent and OptalmologyDocument138 pagesEnt and OptalmologyFan Eli100% (3)
- Textbook Tintinallis Emergency Medicine Manual Rita K Cydulka Ebook All Chapter PDFDocument53 pagesTextbook Tintinallis Emergency Medicine Manual Rita K Cydulka Ebook All Chapter PDFdwain.sanders145100% (2)
- An Investigatory Project ProposalDocument13 pagesAn Investigatory Project ProposalJeg B. Israel Jr.No ratings yet
- Cop TicDocument64 pagesCop TicKraloth RavenheartNo ratings yet
- Fe Del Mundo NCP 2Document7 pagesFe Del Mundo NCP 2Jenness VillanuevaNo ratings yet
- Investigation of InfertilityDocument17 pagesInvestigation of InfertilityRamona GaluNo ratings yet
- Mental Health PDFDocument2 pagesMental Health PDFfirdaNo ratings yet
- Step 1 SampleDocument19 pagesStep 1 Samplerofaida mohammed100% (1)
- Psychiatry OSCE HistoriesDocument5 pagesPsychiatry OSCE HistoriesrangaNo ratings yet
- Bipolarity From Ancient To Modern Times: Conception, Birth and RebirthDocument17 pagesBipolarity From Ancient To Modern Times: Conception, Birth and RebirthMariano OutesNo ratings yet
- Grade 8 Health q3 m1Document17 pagesGrade 8 Health q3 m1Michie Maniego - GumanganNo ratings yet
- Colored Concept MapDocument2 pagesColored Concept Mapapi-544878035No ratings yet
- MRCP 1 May 2015 RecallDocument3 pagesMRCP 1 May 2015 RecallOphthalmology PLUSNo ratings yet
- Acute Coronary Syndrome PDFDocument8 pagesAcute Coronary Syndrome PDFVedranaJovanovicNo ratings yet