
Cortical Visual Impairment in
Cortical Visual Impairment in
You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- Voice Handicap Index 2015Document1 pageVoice Handicap Index 2015Dwi juliana DewiNo ratings yet
- Bus and Coach Station Design GuideDocument35 pagesBus and Coach Station Design GuidemeshNo ratings yet
- BMJ n1212 FullDocument10 pagesBMJ n1212 FullRosela ObandoNo ratings yet
- Jurnal CMVDocument4 pagesJurnal CMVmuarifNo ratings yet
- Halaman DepanDocument6 pagesHalaman DepanzakiNo ratings yet
- Evidence 3) Congenital Infection Causes Neurologic and Hematologic Damage andDocument5 pagesEvidence 3) Congenital Infection Causes Neurologic and Hematologic Damage andandamar0290No ratings yet
- Prevalence of Anti-Cytomegalovirus Anticorps in Children at The Chantal Biya Foundation Mother Child Centre, CameroonDocument6 pagesPrevalence of Anti-Cytomegalovirus Anticorps in Children at The Chantal Biya Foundation Mother Child Centre, CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fowler 1999Document5 pagesFowler 1999OkymailNo ratings yet
- 1-s2.0-S0196439923000259-CMVDocument8 pages1-s2.0-S0196439923000259-CMVaurimeryNo ratings yet
- 2016 Article 310Document6 pages2016 Article 310Gracie ShemaNo ratings yet
- Ophthalmic Physiologic Optic - 2020 - Brandt - Impaired Visual Acuity Caused by Uncorrected Refractive Errors and AmblyopiaDocument11 pagesOphthalmic Physiologic Optic - 2020 - Brandt - Impaired Visual Acuity Caused by Uncorrected Refractive Errors and Amblyopia2017079621No ratings yet
- Congenital Cytomegalovirus Infection Clinical Features and DiagnosisDocument21 pagesCongenital Cytomegalovirus Infection Clinical Features and Diagnosisgomitas21No ratings yet
- Saujanya Vadoothker, MD, Laura Andrews, MD, Bennie H. Jeng, MD, and Moran Roni Levin, MDDocument5 pagesSaujanya Vadoothker, MD, Laura Andrews, MD, Bennie H. Jeng, MD, and Moran Roni Levin, MDakmilNo ratings yet
- TORCH InfectionsDocument37 pagesTORCH InfectionsEylin Halim Rahardjo100% (1)
- Articol 14.05Document7 pagesArticol 14.05Ilina Lavinia IoanaNo ratings yet
- Jurnal Fixxxx 1Document14 pagesJurnal Fixxxx 1heryanggunNo ratings yet
- Acta Paediatrica - 2020 - Lüsebrink - Retrospectively Diagnosing Congenital Cytomegalovirus Infections in SymptomaticDocument6 pagesActa Paediatrica - 2020 - Lüsebrink - Retrospectively Diagnosing Congenital Cytomegalovirus Infections in Symptomaticdossantoselaine212No ratings yet
- Effects of Paediatric HIV Infection On Childhood VasculatureDocument7 pagesEffects of Paediatric HIV Infection On Childhood VasculaturemuhammadNo ratings yet
- Prevention of Congenital Cytomegalovirus Infection With Vaccines State of The ArtDocument11 pagesPrevention of Congenital Cytomegalovirus Infection With Vaccines State of The Artmadimadi11No ratings yet
- JurnalDocument2 pagesJurnalzakiNo ratings yet
- Journal 3Document6 pagesJournal 3riskab123No ratings yet
- Infecciones Neonatale IDocument13 pagesInfecciones Neonatale IFidel RamonNo ratings yet
- Congenital CMV Infection in Symptomatic Infants in Delhi and Surrounding AreasDocument3 pagesCongenital CMV Infection in Symptomatic Infants in Delhi and Surrounding AreasMinerva StanciuNo ratings yet
- Wa0024Document18 pagesWa0024Marlin 08No ratings yet
- Congenital Cytomegalovirus Infection: Current Strategies and Future PerspectivesDocument17 pagesCongenital Cytomegalovirus Infection: Current Strategies and Future PerspectivesAfif AriyanwarNo ratings yet
- Management of Sickle Cell Disease in Children: Review ArticleDocument8 pagesManagement of Sickle Cell Disease in Children: Review ArticleH. MD EbrNo ratings yet
- NohlpsbfurnDocument17 pagesNohlpsbfurnTri Setya NNo ratings yet
- Effect of Cytomegalovirus Retinitis On The Risk of Visual Acuity Loss Among Patients With AIDSDocument4 pagesEffect of Cytomegalovirus Retinitis On The Risk of Visual Acuity Loss Among Patients With AIDSsiti maryam isnaeniNo ratings yet
- 2014 Article 42Document10 pages2014 Article 42Mike StoneNo ratings yet
- Jurnal MataDocument8 pagesJurnal MatamarinarizkiNo ratings yet
- TSWJ2012 109624 PDFDocument6 pagesTSWJ2012 109624 PDFErika CordeiroNo ratings yet
- CMV Review 2021Document9 pagesCMV Review 2021Iralda ValenciaNo ratings yet
- Hearing Loss in Children With Asymptomatic Congenital Cytomegalovirus InfectionDocument10 pagesHearing Loss in Children With Asymptomatic Congenital Cytomegalovirus InfectionAsniar RNo ratings yet
- Congenital Cytomegalovirus-HistoryDocument6 pagesCongenital Cytomegalovirus-Historydossantoselaine212No ratings yet
- Neoplasia de Vulva, Marzo 2022Document6 pagesNeoplasia de Vulva, Marzo 2022rafael martinezNo ratings yet
- CMV 3Document11 pagesCMV 3Birgitta IvanaNo ratings yet
- Research in Developmental DisabilitiesDocument9 pagesResearch in Developmental DisabilitiesCarina Adriana BeerenfengerNo ratings yet
- Cortical Visual Impairment: Susan M. Carden and William V. GoodDocument8 pagesCortical Visual Impairment: Susan M. Carden and William V. GoodAmal AlmutiriNo ratings yet
- 7Document4 pages7IRA ODETTE GATUSNo ratings yet
- HHS Public Access: Sturge-Weber SyndromeDocument12 pagesHHS Public Access: Sturge-Weber SyndromeHanii HunnNo ratings yet
- Tseng Et Al 2022 Severe Maternal Morbidity in Pregnancies Complicated by Fetal Congenital Heart DiseaseDocument10 pagesTseng Et Al 2022 Severe Maternal Morbidity in Pregnancies Complicated by Fetal Congenital Heart DiseaseUMAE GINENo ratings yet
- Visual Loss in Uveitis of ChildhoodDocument29 pagesVisual Loss in Uveitis of ChildhoodRizky AgustriaNo ratings yet
- Jogh 12 12003Document10 pagesJogh 12 12003mzpc8rpf78No ratings yet
- Hydro Cep HalDocument6 pagesHydro Cep HalVALMIRNo ratings yet
- Lancet DeliriumDocument10 pagesLancet Deliriumyennifer hoyos mendezNo ratings yet
- Congenital Cytomegalovirus Infection Management and OutcomeDocument20 pagesCongenital Cytomegalovirus Infection Management and Outcomegomitas21No ratings yet
- Therapeutic Approach To The Management of Pediatric Demyelinating Disease: Multiple Sclerosis and Acute Disseminated EncephalomyelitisDocument12 pagesTherapeutic Approach To The Management of Pediatric Demyelinating Disease: Multiple Sclerosis and Acute Disseminated EncephalomyelitiscarlaNo ratings yet
- Mangione Et Al-2011-Ultrasound in Obstetrics & GynecologyDocument6 pagesMangione Et Al-2011-Ultrasound in Obstetrics & GynecologyAnggita Rizki KusumaNo ratings yet
- Cesarean Delivery and Risk of Infant Leukemia: A Report From The Children's Oncology GroupDocument7 pagesCesarean Delivery and Risk of Infant Leukemia: A Report From The Children's Oncology GroupKarina Braga RibeiroNo ratings yet
- Knowledge of Cytomegalovirus and Available Prevention Strategies in Pregnancy A Cross-Sectional Study in PortugalDocument8 pagesKnowledge of Cytomegalovirus and Available Prevention Strategies in Pregnancy A Cross-Sectional Study in PortugalLissaberti AmaliahNo ratings yet
- Investigating The Child With Intellectual Disability: Review ArticleDocument5 pagesInvestigating The Child With Intellectual Disability: Review ArticleCristinaNo ratings yet
- Inflammatory: Bowel DiseaseDocument14 pagesInflammatory: Bowel Diseaseusmani_nida1No ratings yet
- Citomegalovirus Perdida Auditiva en Niños 2Document9 pagesCitomegalovirus Perdida Auditiva en Niños 2Valentina HurtadoNo ratings yet
- Prevalence and Causes of Visual Impairment in PatiDocument6 pagesPrevalence and Causes of Visual Impairment in Pati2017079621No ratings yet
- Khouri 2015Document17 pagesKhouri 2015Potencia SalasNo ratings yet
- Profile and Outcome of Congenital Heart Disease in Buea South West Region of Cameroon A Cross Sectional StudyDocument6 pagesProfile and Outcome of Congenital Heart Disease in Buea South West Region of Cameroon A Cross Sectional StudyAthenaeum Scientific PublishersNo ratings yet
- Clinical Manifestations of Congenital Rubella Syndrome at The Korle-Bu Teaching Hospital, GhanaDocument6 pagesClinical Manifestations of Congenital Rubella Syndrome at The Korle-Bu Teaching Hospital, GhanaAndhika Wahyu AnggaraNo ratings yet
- Congenital Malformations in The Newborn Population: A Population Study and Analysis of The Effect of Sex and PrematurityDocument6 pagesCongenital Malformations in The Newborn Population: A Population Study and Analysis of The Effect of Sex and PrematuritydentsavvyNo ratings yet
- Rubeola Caso ClinicoDocument3 pagesRubeola Caso Clinicomaria martinezNo ratings yet
- Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera UtaraDocument33 pagesInfectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera UtaramaruliasnaNo ratings yet
- Kraaijenga 2016Document7 pagesKraaijenga 2016Dwi juliana DewiNo ratings yet
- Sal Men 2016Document9 pagesSal Men 2016Dwi juliana DewiNo ratings yet
- Lary 23467Document8 pagesLary 23467Dwi juliana DewiNo ratings yet
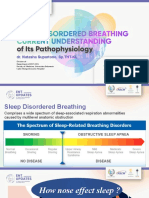
- Sesi 1 - Dr. Natasha SP - THT-KL - SDB Current Understanding of Its PathophysiologyDocument20 pagesSesi 1 - Dr. Natasha SP - THT-KL - SDB Current Understanding of Its PathophysiologyDwi juliana DewiNo ratings yet
- TON Agung Final (Autosaved)Document28 pagesTON Agung Final (Autosaved)Dwi juliana DewiNo ratings yet
- Effect of Upper Airway Surgery On Heart Rate Variability in Patients With Obstructive Sleep Apnoea SyndromeDocument6 pagesEffect of Upper Airway Surgery On Heart Rate Variability in Patients With Obstructive Sleep Apnoea SyndromeDwi juliana DewiNo ratings yet
- Parasympathetic Overactivity in Patients With Nasal Septum DeformitiesDocument5 pagesParasympathetic Overactivity in Patients With Nasal Septum DeformitiesDwi juliana DewiNo ratings yet
- Consent For Publication of Figure Image And/or Case InformationDocument1 pageConsent For Publication of Figure Image And/or Case InformationDwi juliana DewiNo ratings yet
- The Nasocardiac Reflex: 1988. 43, PagesDocument2 pagesThe Nasocardiac Reflex: 1988. 43, PagesDwi juliana DewiNo ratings yet
- Original Articles: X Deafness and Mental ToDocument7 pagesOriginal Articles: X Deafness and Mental ToDwi juliana DewiNo ratings yet
- Comorbidities and Their RelatiDocument5 pagesComorbidities and Their RelatiDwi juliana DewiNo ratings yet
- New Doc 2018-02-07 14.49.01-20180207144929 PDFDocument1 pageNew Doc 2018-02-07 14.49.01-20180207144929 PDFDwi juliana DewiNo ratings yet
- Inclusive Tnteu Unit 1Document73 pagesInclusive Tnteu Unit 1PriyaNo ratings yet
- Padlet F59h76nufzlw9riyDocument12 pagesPadlet F59h76nufzlw9riyapi-510318961No ratings yet
- Sowell Book List 4-2-2014Document9 pagesSowell Book List 4-2-2014ClaytonSilvaNo ratings yet
- 2.2.2.how To Do The Eye Health Clinical Audit PDFDocument50 pages2.2.2.how To Do The Eye Health Clinical Audit PDFCynthia Jaramillo MachucaNo ratings yet
- CATARACT Surgery Season Month Wise Reported Figure in IndiaDocument5 pagesCATARACT Surgery Season Month Wise Reported Figure in IndiafriendsofindiaNo ratings yet
- Disabilities Act 1995Document19 pagesDisabilities Act 1995Aditya BasuNo ratings yet
- Definition of Blindness As Defined by National Program For Control of Blindness (NPCB)Document2 pagesDefinition of Blindness As Defined by National Program For Control of Blindness (NPCB)Kartik SinghNo ratings yet
- Caring For People With DisabilitiesDocument45 pagesCaring For People With DisabilitiesStephen NyakundiNo ratings yet
- Cataract Case Mix StudyDocument19 pagesCataract Case Mix StudyHarry PribadiNo ratings yet
- Voice Based Email IJCA2020Document6 pagesVoice Based Email IJCA2020Amreen KhanNo ratings yet
- Barrier Free ArchitectureDocument14 pagesBarrier Free Architecturewog jimNo ratings yet
- YoloV4 Based Object Detection For Blind StickDocument5 pagesYoloV4 Based Object Detection For Blind StickInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Date-589e9a299e6e55 68915918 PDFDocument2 pagesDate-589e9a299e6e55 68915918 PDFnathan3wright8No ratings yet
- Aa 11Document6 pagesAa 11Muhammad Sheharyar MohsinNo ratings yet
- Health Literacy in Older Adults With and Without Low VisionDocument8 pagesHealth Literacy in Older Adults With and Without Low VisionPierre A. RodulfoNo ratings yet
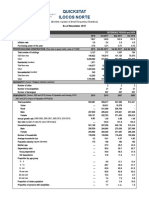
- Quickstat Ilocos Norte: (Monthly Update of Most Requested Statistics)Document4 pagesQuickstat Ilocos Norte: (Monthly Update of Most Requested Statistics)redNo ratings yet
- Group No.08: Group Members Regula Dominick Daniel Urio Gido Focus Julius Saitore Vuai Denge Fred Luhangano John AkyooDocument31 pagesGroup No.08: Group Members Regula Dominick Daniel Urio Gido Focus Julius Saitore Vuai Denge Fred Luhangano John AkyooralphNo ratings yet
- An Insight Into Assistive Technology For The Visually Impaired and Blind People State-Of-The-Art and Future TrendDocument24 pagesAn Insight Into Assistive Technology For The Visually Impaired and Blind People State-Of-The-Art and Future Trendanaaliceasantos31No ratings yet
- BSC (N) Iii Year Child Health Nursing: Unit Vi - Management of Behavioural and Social Problems in ChildrenDocument79 pagesBSC (N) Iii Year Child Health Nursing: Unit Vi - Management of Behavioural and Social Problems in ChildrenERIC ANGEL100% (1)
- An Appeal To The Senses: The Development of The Braille System in Nineteenth-Century FranceDocument5 pagesAn Appeal To The Senses: The Development of The Braille System in Nineteenth-Century FranceGrlaeNo ratings yet
- Chapter 3 SoftDocument15 pagesChapter 3 SoftBethanie Mendiola BaseNo ratings yet
- CATKing CRITICAL REASONING QuestionsDocument72 pagesCATKing CRITICAL REASONING QuestionsArindam ChatterjeeNo ratings yet
- 2022 Elem 133945Document61 pages2022 Elem 133945calma3961No ratings yet
- InterRAI Community Health Assessment (CHA)Document10 pagesInterRAI Community Health Assessment (CHA)Mike F MartelliNo ratings yet
- Periocular Hyaluronic Acid Fillers: Applications, Implications, ComplicationsDocument6 pagesPeriocular Hyaluronic Acid Fillers: Applications, Implications, ComplicationsLuis Fernando WeffortNo ratings yet
- Semis DCF Part 1 2 Final-RevisedDocument46 pagesSemis DCF Part 1 2 Final-RevisedVahidNo ratings yet
- Low Vision FileDocument1 pageLow Vision FileEugene KusiNo ratings yet
- Occ MindoroDocument269 pagesOcc MindoroElleason Joshua G. FranciscoNo ratings yet
- Vineeth - Curriculum VitaDocument8 pagesVineeth - Curriculum VitaVineeth NBNo ratings yet





































































































Download as pdf or txt
You might also like
- USMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyFrom EverandUSMLE Step 3 Lecture Notes 2021-2022: Pediatrics, Obstetrics/Gynecology, Surgery, Epidemiology/Biostatistics, Patient SafetyRating: 5 out of 5 stars5/5 (2)
- Clinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3From EverandClinical Management Review 2023-2024: Volume 2: USMLE Step 3 and COMLEX-USA Level 3No ratings yet
- Voice Handicap Index 2015Document1 pageVoice Handicap Index 2015Dwi juliana DewiNo ratings yet
- Bus and Coach Station Design GuideDocument35 pagesBus and Coach Station Design GuidemeshNo ratings yet
- BMJ n1212 FullDocument10 pagesBMJ n1212 FullRosela ObandoNo ratings yet
- Jurnal CMVDocument4 pagesJurnal CMVmuarifNo ratings yet
- Halaman DepanDocument6 pagesHalaman DepanzakiNo ratings yet
- Evidence 3) Congenital Infection Causes Neurologic and Hematologic Damage andDocument5 pagesEvidence 3) Congenital Infection Causes Neurologic and Hematologic Damage andandamar0290No ratings yet
- Prevalence of Anti-Cytomegalovirus Anticorps in Children at The Chantal Biya Foundation Mother Child Centre, CameroonDocument6 pagesPrevalence of Anti-Cytomegalovirus Anticorps in Children at The Chantal Biya Foundation Mother Child Centre, CameroonInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Fowler 1999Document5 pagesFowler 1999OkymailNo ratings yet
- 1-s2.0-S0196439923000259-CMVDocument8 pages1-s2.0-S0196439923000259-CMVaurimeryNo ratings yet
- 2016 Article 310Document6 pages2016 Article 310Gracie ShemaNo ratings yet
- Ophthalmic Physiologic Optic - 2020 - Brandt - Impaired Visual Acuity Caused by Uncorrected Refractive Errors and AmblyopiaDocument11 pagesOphthalmic Physiologic Optic - 2020 - Brandt - Impaired Visual Acuity Caused by Uncorrected Refractive Errors and Amblyopia2017079621No ratings yet
- Congenital Cytomegalovirus Infection Clinical Features and DiagnosisDocument21 pagesCongenital Cytomegalovirus Infection Clinical Features and Diagnosisgomitas21No ratings yet
- Saujanya Vadoothker, MD, Laura Andrews, MD, Bennie H. Jeng, MD, and Moran Roni Levin, MDDocument5 pagesSaujanya Vadoothker, MD, Laura Andrews, MD, Bennie H. Jeng, MD, and Moran Roni Levin, MDakmilNo ratings yet
- TORCH InfectionsDocument37 pagesTORCH InfectionsEylin Halim Rahardjo100% (1)
- Articol 14.05Document7 pagesArticol 14.05Ilina Lavinia IoanaNo ratings yet
- Jurnal Fixxxx 1Document14 pagesJurnal Fixxxx 1heryanggunNo ratings yet
- Acta Paediatrica - 2020 - Lüsebrink - Retrospectively Diagnosing Congenital Cytomegalovirus Infections in SymptomaticDocument6 pagesActa Paediatrica - 2020 - Lüsebrink - Retrospectively Diagnosing Congenital Cytomegalovirus Infections in Symptomaticdossantoselaine212No ratings yet
- Effects of Paediatric HIV Infection On Childhood VasculatureDocument7 pagesEffects of Paediatric HIV Infection On Childhood VasculaturemuhammadNo ratings yet
- Prevention of Congenital Cytomegalovirus Infection With Vaccines State of The ArtDocument11 pagesPrevention of Congenital Cytomegalovirus Infection With Vaccines State of The Artmadimadi11No ratings yet
- JurnalDocument2 pagesJurnalzakiNo ratings yet
- Journal 3Document6 pagesJournal 3riskab123No ratings yet
- Infecciones Neonatale IDocument13 pagesInfecciones Neonatale IFidel RamonNo ratings yet
- Congenital CMV Infection in Symptomatic Infants in Delhi and Surrounding AreasDocument3 pagesCongenital CMV Infection in Symptomatic Infants in Delhi and Surrounding AreasMinerva StanciuNo ratings yet
- Wa0024Document18 pagesWa0024Marlin 08No ratings yet
- Congenital Cytomegalovirus Infection: Current Strategies and Future PerspectivesDocument17 pagesCongenital Cytomegalovirus Infection: Current Strategies and Future PerspectivesAfif AriyanwarNo ratings yet
- Management of Sickle Cell Disease in Children: Review ArticleDocument8 pagesManagement of Sickle Cell Disease in Children: Review ArticleH. MD EbrNo ratings yet
- NohlpsbfurnDocument17 pagesNohlpsbfurnTri Setya NNo ratings yet
- Effect of Cytomegalovirus Retinitis On The Risk of Visual Acuity Loss Among Patients With AIDSDocument4 pagesEffect of Cytomegalovirus Retinitis On The Risk of Visual Acuity Loss Among Patients With AIDSsiti maryam isnaeniNo ratings yet
- 2014 Article 42Document10 pages2014 Article 42Mike StoneNo ratings yet
- Jurnal MataDocument8 pagesJurnal MatamarinarizkiNo ratings yet
- TSWJ2012 109624 PDFDocument6 pagesTSWJ2012 109624 PDFErika CordeiroNo ratings yet
- CMV Review 2021Document9 pagesCMV Review 2021Iralda ValenciaNo ratings yet
- Hearing Loss in Children With Asymptomatic Congenital Cytomegalovirus InfectionDocument10 pagesHearing Loss in Children With Asymptomatic Congenital Cytomegalovirus InfectionAsniar RNo ratings yet
- Congenital Cytomegalovirus-HistoryDocument6 pagesCongenital Cytomegalovirus-Historydossantoselaine212No ratings yet
- Neoplasia de Vulva, Marzo 2022Document6 pagesNeoplasia de Vulva, Marzo 2022rafael martinezNo ratings yet
- CMV 3Document11 pagesCMV 3Birgitta IvanaNo ratings yet
- Research in Developmental DisabilitiesDocument9 pagesResearch in Developmental DisabilitiesCarina Adriana BeerenfengerNo ratings yet
- Cortical Visual Impairment: Susan M. Carden and William V. GoodDocument8 pagesCortical Visual Impairment: Susan M. Carden and William V. GoodAmal AlmutiriNo ratings yet
- 7Document4 pages7IRA ODETTE GATUSNo ratings yet
- HHS Public Access: Sturge-Weber SyndromeDocument12 pagesHHS Public Access: Sturge-Weber SyndromeHanii HunnNo ratings yet
- Tseng Et Al 2022 Severe Maternal Morbidity in Pregnancies Complicated by Fetal Congenital Heart DiseaseDocument10 pagesTseng Et Al 2022 Severe Maternal Morbidity in Pregnancies Complicated by Fetal Congenital Heart DiseaseUMAE GINENo ratings yet
- Visual Loss in Uveitis of ChildhoodDocument29 pagesVisual Loss in Uveitis of ChildhoodRizky AgustriaNo ratings yet
- Jogh 12 12003Document10 pagesJogh 12 12003mzpc8rpf78No ratings yet
- Hydro Cep HalDocument6 pagesHydro Cep HalVALMIRNo ratings yet
- Lancet DeliriumDocument10 pagesLancet Deliriumyennifer hoyos mendezNo ratings yet
- Congenital Cytomegalovirus Infection Management and OutcomeDocument20 pagesCongenital Cytomegalovirus Infection Management and Outcomegomitas21No ratings yet
- Therapeutic Approach To The Management of Pediatric Demyelinating Disease: Multiple Sclerosis and Acute Disseminated EncephalomyelitisDocument12 pagesTherapeutic Approach To The Management of Pediatric Demyelinating Disease: Multiple Sclerosis and Acute Disseminated EncephalomyelitiscarlaNo ratings yet
- Mangione Et Al-2011-Ultrasound in Obstetrics & GynecologyDocument6 pagesMangione Et Al-2011-Ultrasound in Obstetrics & GynecologyAnggita Rizki KusumaNo ratings yet
- Cesarean Delivery and Risk of Infant Leukemia: A Report From The Children's Oncology GroupDocument7 pagesCesarean Delivery and Risk of Infant Leukemia: A Report From The Children's Oncology GroupKarina Braga RibeiroNo ratings yet
- Knowledge of Cytomegalovirus and Available Prevention Strategies in Pregnancy A Cross-Sectional Study in PortugalDocument8 pagesKnowledge of Cytomegalovirus and Available Prevention Strategies in Pregnancy A Cross-Sectional Study in PortugalLissaberti AmaliahNo ratings yet
- Investigating The Child With Intellectual Disability: Review ArticleDocument5 pagesInvestigating The Child With Intellectual Disability: Review ArticleCristinaNo ratings yet
- Inflammatory: Bowel DiseaseDocument14 pagesInflammatory: Bowel Diseaseusmani_nida1No ratings yet
- Citomegalovirus Perdida Auditiva en Niños 2Document9 pagesCitomegalovirus Perdida Auditiva en Niños 2Valentina HurtadoNo ratings yet
- Prevalence and Causes of Visual Impairment in PatiDocument6 pagesPrevalence and Causes of Visual Impairment in Pati2017079621No ratings yet
- Khouri 2015Document17 pagesKhouri 2015Potencia SalasNo ratings yet
- Profile and Outcome of Congenital Heart Disease in Buea South West Region of Cameroon A Cross Sectional StudyDocument6 pagesProfile and Outcome of Congenital Heart Disease in Buea South West Region of Cameroon A Cross Sectional StudyAthenaeum Scientific PublishersNo ratings yet
- Clinical Manifestations of Congenital Rubella Syndrome at The Korle-Bu Teaching Hospital, GhanaDocument6 pagesClinical Manifestations of Congenital Rubella Syndrome at The Korle-Bu Teaching Hospital, GhanaAndhika Wahyu AnggaraNo ratings yet
- Congenital Malformations in The Newborn Population: A Population Study and Analysis of The Effect of Sex and PrematurityDocument6 pagesCongenital Malformations in The Newborn Population: A Population Study and Analysis of The Effect of Sex and PrematuritydentsavvyNo ratings yet
- Rubeola Caso ClinicoDocument3 pagesRubeola Caso Clinicomaria martinezNo ratings yet
- Infectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera UtaraDocument33 pagesInfectious and Tropical Pediatric Division Department of Child Health Medical Faculty, University of Sumatera UtaramaruliasnaNo ratings yet
- Kraaijenga 2016Document7 pagesKraaijenga 2016Dwi juliana DewiNo ratings yet
- Sal Men 2016Document9 pagesSal Men 2016Dwi juliana DewiNo ratings yet
- Lary 23467Document8 pagesLary 23467Dwi juliana DewiNo ratings yet
- Sesi 1 - Dr. Natasha SP - THT-KL - SDB Current Understanding of Its PathophysiologyDocument20 pagesSesi 1 - Dr. Natasha SP - THT-KL - SDB Current Understanding of Its PathophysiologyDwi juliana DewiNo ratings yet
- TON Agung Final (Autosaved)Document28 pagesTON Agung Final (Autosaved)Dwi juliana DewiNo ratings yet
- Effect of Upper Airway Surgery On Heart Rate Variability in Patients With Obstructive Sleep Apnoea SyndromeDocument6 pagesEffect of Upper Airway Surgery On Heart Rate Variability in Patients With Obstructive Sleep Apnoea SyndromeDwi juliana DewiNo ratings yet
- Parasympathetic Overactivity in Patients With Nasal Septum DeformitiesDocument5 pagesParasympathetic Overactivity in Patients With Nasal Septum DeformitiesDwi juliana DewiNo ratings yet
- Consent For Publication of Figure Image And/or Case InformationDocument1 pageConsent For Publication of Figure Image And/or Case InformationDwi juliana DewiNo ratings yet
- The Nasocardiac Reflex: 1988. 43, PagesDocument2 pagesThe Nasocardiac Reflex: 1988. 43, PagesDwi juliana DewiNo ratings yet
- Original Articles: X Deafness and Mental ToDocument7 pagesOriginal Articles: X Deafness and Mental ToDwi juliana DewiNo ratings yet
- Comorbidities and Their RelatiDocument5 pagesComorbidities and Their RelatiDwi juliana DewiNo ratings yet
- New Doc 2018-02-07 14.49.01-20180207144929 PDFDocument1 pageNew Doc 2018-02-07 14.49.01-20180207144929 PDFDwi juliana DewiNo ratings yet
- Inclusive Tnteu Unit 1Document73 pagesInclusive Tnteu Unit 1PriyaNo ratings yet
- Padlet F59h76nufzlw9riyDocument12 pagesPadlet F59h76nufzlw9riyapi-510318961No ratings yet
- Sowell Book List 4-2-2014Document9 pagesSowell Book List 4-2-2014ClaytonSilvaNo ratings yet
- 2.2.2.how To Do The Eye Health Clinical Audit PDFDocument50 pages2.2.2.how To Do The Eye Health Clinical Audit PDFCynthia Jaramillo MachucaNo ratings yet
- CATARACT Surgery Season Month Wise Reported Figure in IndiaDocument5 pagesCATARACT Surgery Season Month Wise Reported Figure in IndiafriendsofindiaNo ratings yet
- Disabilities Act 1995Document19 pagesDisabilities Act 1995Aditya BasuNo ratings yet
- Definition of Blindness As Defined by National Program For Control of Blindness (NPCB)Document2 pagesDefinition of Blindness As Defined by National Program For Control of Blindness (NPCB)Kartik SinghNo ratings yet
- Caring For People With DisabilitiesDocument45 pagesCaring For People With DisabilitiesStephen NyakundiNo ratings yet
- Cataract Case Mix StudyDocument19 pagesCataract Case Mix StudyHarry PribadiNo ratings yet
- Voice Based Email IJCA2020Document6 pagesVoice Based Email IJCA2020Amreen KhanNo ratings yet
- Barrier Free ArchitectureDocument14 pagesBarrier Free Architecturewog jimNo ratings yet
- YoloV4 Based Object Detection For Blind StickDocument5 pagesYoloV4 Based Object Detection For Blind StickInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Date-589e9a299e6e55 68915918 PDFDocument2 pagesDate-589e9a299e6e55 68915918 PDFnathan3wright8No ratings yet
- Aa 11Document6 pagesAa 11Muhammad Sheharyar MohsinNo ratings yet
- Health Literacy in Older Adults With and Without Low VisionDocument8 pagesHealth Literacy in Older Adults With and Without Low VisionPierre A. RodulfoNo ratings yet
- Quickstat Ilocos Norte: (Monthly Update of Most Requested Statistics)Document4 pagesQuickstat Ilocos Norte: (Monthly Update of Most Requested Statistics)redNo ratings yet
- Group No.08: Group Members Regula Dominick Daniel Urio Gido Focus Julius Saitore Vuai Denge Fred Luhangano John AkyooDocument31 pagesGroup No.08: Group Members Regula Dominick Daniel Urio Gido Focus Julius Saitore Vuai Denge Fred Luhangano John AkyooralphNo ratings yet
- An Insight Into Assistive Technology For The Visually Impaired and Blind People State-Of-The-Art and Future TrendDocument24 pagesAn Insight Into Assistive Technology For The Visually Impaired and Blind People State-Of-The-Art and Future Trendanaaliceasantos31No ratings yet
- BSC (N) Iii Year Child Health Nursing: Unit Vi - Management of Behavioural and Social Problems in ChildrenDocument79 pagesBSC (N) Iii Year Child Health Nursing: Unit Vi - Management of Behavioural and Social Problems in ChildrenERIC ANGEL100% (1)
- An Appeal To The Senses: The Development of The Braille System in Nineteenth-Century FranceDocument5 pagesAn Appeal To The Senses: The Development of The Braille System in Nineteenth-Century FranceGrlaeNo ratings yet
- Chapter 3 SoftDocument15 pagesChapter 3 SoftBethanie Mendiola BaseNo ratings yet
- CATKing CRITICAL REASONING QuestionsDocument72 pagesCATKing CRITICAL REASONING QuestionsArindam ChatterjeeNo ratings yet
- 2022 Elem 133945Document61 pages2022 Elem 133945calma3961No ratings yet
- InterRAI Community Health Assessment (CHA)Document10 pagesInterRAI Community Health Assessment (CHA)Mike F MartelliNo ratings yet
- Periocular Hyaluronic Acid Fillers: Applications, Implications, ComplicationsDocument6 pagesPeriocular Hyaluronic Acid Fillers: Applications, Implications, ComplicationsLuis Fernando WeffortNo ratings yet
- Semis DCF Part 1 2 Final-RevisedDocument46 pagesSemis DCF Part 1 2 Final-RevisedVahidNo ratings yet
- Low Vision FileDocument1 pageLow Vision FileEugene KusiNo ratings yet
- Occ MindoroDocument269 pagesOcc MindoroElleason Joshua G. FranciscoNo ratings yet
- Vineeth - Curriculum VitaDocument8 pagesVineeth - Curriculum VitaVineeth NBNo ratings yet