Download as pdf or txt
You might also like
- DocuNotes Clinical Pocket Guide To Effective ChartingDocument203 pagesDocuNotes Clinical Pocket Guide To Effective ChartingShirlyn Ares Navarro96% (47)
- Certified Medical Office Administrative Assistant Study GuideFrom EverandCertified Medical Office Administrative Assistant Study GuideNo ratings yet
- The Online Poker Starting Guide (Frank Miller) PDFDocument39 pagesThe Online Poker Starting Guide (Frank Miller) PDFDe_VinciNo ratings yet
- H06D Assignment 8Document4 pagesH06D Assignment 8Good ChannelNo ratings yet
- 17 Tips To Improve Your Nursing DocumentationDocument26 pages17 Tips To Improve Your Nursing DocumentationAgustin Lutfiana100% (2)
- Relevance of Nursing Documentation and Its Legal ImplicationsDocument8 pagesRelevance of Nursing Documentation and Its Legal ImplicationsGeorge AyiteyNo ratings yet
- Chapter 26Document46 pagesChapter 26meeeenonNo ratings yet
- Chapter 26: Documentation and Informatics Mistakes in Documentation That Commonly Results in MalpracticeDocument9 pagesChapter 26: Documentation and Informatics Mistakes in Documentation That Commonly Results in MalpracticejoanneNo ratings yet
- Medical Records, Insurance, and ContractsDocument24 pagesMedical Records, Insurance, and ContractsBernard Kwaku OkaiNo ratings yet
- Ethical CompetenceDocument28 pagesEthical CompetenceRysanNo ratings yet
- Nursing TherapyDocument121 pagesNursing TherapyIra AarisNo ratings yet
- Nursing Therapy's NotesDocument121 pagesNursing Therapy's NotesVerline Santiong V. JoanNo ratings yet
- Medical Records, Patient Care, and Medical EducationDocument12 pagesMedical Records, Patient Care, and Medical EducationcarolinaNo ratings yet
- Documentation Course MaterialDocument15 pagesDocumentation Course MaterialSheNo ratings yet
- Nursing Process QuestionsDocument12 pagesNursing Process QuestionsSritama Ghosh100% (1)
- J.Baxton 450 1Document7 pagesJ.Baxton 450 1osunbor houseNo ratings yet
- Building A Cooperative Patient/doctor RelationshipDocument4 pagesBuilding A Cooperative Patient/doctor RelationshipskjfdsahjkdfsaNo ratings yet
- Ha WK2Document9 pagesHa WK2MARY ROSE FAJUTINANo ratings yet
- Medical Records: Making and Retaining Them: What Is A Medical Record?Document6 pagesMedical Records: Making and Retaining Them: What Is A Medical Record?mfadly maulanaNo ratings yet
- Medical RecordDocument14 pagesMedical RecordZakwan AhmadNo ratings yet
- Documentation and ReportingDocument4 pagesDocumentation and Reportingsnv rishiNo ratings yet
- Lesson 2:: Medical ANDDocument38 pagesLesson 2:: Medical ANDKAH' CHISMISSNo ratings yet
- All Document Reader 1715231408716Document11 pagesAll Document Reader 1715231408716jebungeidNo ratings yet
- A Day in The Life of A Health Information SpecialistDocument4 pagesA Day in The Life of A Health Information Specialist050Nok Aam RamadhaniatiNo ratings yet
- NursingDocument12 pagesNursingkasandrajarayseh04No ratings yet
- Understanding Patient Expectations: Toward A Better Physician Office ExperienceDocument2 pagesUnderstanding Patient Expectations: Toward A Better Physician Office Experienceapi-94302037No ratings yet
- Code of EhicsDocument36 pagesCode of Ehicsrussellnicoabendanabendan1234No ratings yet
- The Legalities of Nursing DocumentationDocument6 pagesThe Legalities of Nursing DocumentationCandace FlowersNo ratings yet
- HCE EsssayDocument3 pagesHCE EsssayAeivan Mae SombrioNo ratings yet
- Bioethics - Elmer - Module 3Document2 pagesBioethics - Elmer - Module 3KaguraNo ratings yet
- Nursing RecordsDocument20 pagesNursing Recordstessy mathewNo ratings yet
- Implementing The Nursing Care PlanDocument33 pagesImplementing The Nursing Care PlanCarlo Paul Castro SanaNo ratings yet
- Everything You Need To Know To Be An Organized and Successful PatientFrom EverandEverything You Need To Know To Be An Organized and Successful PatientNo ratings yet
- Nursing Process Study Guide Packet 1 Exam 1Document13 pagesNursing Process Study Guide Packet 1 Exam 1Emily StoicovyNo ratings yet
- Hcs120r2 Week 3 Terms WorksheetDocument3 pagesHcs120r2 Week 3 Terms WorksheetCarsha RidleyNo ratings yet
- Unit 1 Documentation-and-ReportingDocument39 pagesUnit 1 Documentation-and-ReportingMs.V. Mahesha Asst. Prof.No ratings yet
- Nursing Process-Part 1Document31 pagesNursing Process-Part 1abigael cheptanuiNo ratings yet
- Good Medical Practice (NZ)Document38 pagesGood Medical Practice (NZ)Tawfeeq AuqbiNo ratings yet
- HM101 Final ExamDocument6 pagesHM101 Final ExamRachael CrossgroveNo ratings yet
- Return To Top: AssessmentDocument5 pagesReturn To Top: AssessmentDatu Puti MangelenNo ratings yet
- Bioethic Module 3Document3 pagesBioethic Module 3Danica CorpuzNo ratings yet
- Legal Implications Document A Schneider PDFDocument52 pagesLegal Implications Document A Schneider PDFAmrod Inglorion100% (2)
- 7 Legal Tips For Safe Nursing PracticesDocument7 pages7 Legal Tips For Safe Nursing PracticesAlex LeplerNo ratings yet
- HA Intro Part 2Document21 pagesHA Intro Part 2alyanadayrit100% (1)
- (Nursing English) DIYAH AHADYATUNNISADocument10 pages(Nursing English) DIYAH AHADYATUNNISAdiyah hansuNo ratings yet
- Medical ProceduresDocument33 pagesMedical ProceduresAlistair ElliseNo ratings yet
- Wash ST Privacy StatementDocument5 pagesWash ST Privacy Statementapi-408949005No ratings yet
- Ota Go 614506Document4 pagesOta Go 614506gus_lionsNo ratings yet
- Hospital GuideDocument5 pagesHospital Guideeka puspitaNo ratings yet
- Challenges Faced in My Weekly Clinical ExperienceDocument4 pagesChallenges Faced in My Weekly Clinical Experiencefredrickm kamau2017No ratings yet
- Nursing ProcessDocument52 pagesNursing ProcessDzon LornaNo ratings yet
- Chapter 1 - Introduction To Health Record ManagementDocument18 pagesChapter 1 - Introduction To Health Record ManagementLalita A/P AnbarasenNo ratings yet
- Activity 84087Document19 pagesActivity 84087Johncarlo GenestonNo ratings yet
- Shelf Prep: Guide To The Internal Medicine ClerkshipDocument2 pagesShelf Prep: Guide To The Internal Medicine ClerkshipRuth SanmooganNo ratings yet
- 1 Benchmark - Documentation of ProtocolsDocument10 pages1 Benchmark - Documentation of Protocolsjoseph mainaNo ratings yet
- Never Go to the Hospital Alone: And Other Insider Secrets for Getting Mistake-Free Health Care from Your Doctor and HospitalFrom EverandNever Go to the Hospital Alone: And Other Insider Secrets for Getting Mistake-Free Health Care from Your Doctor and HospitalNo ratings yet
- The Slim Book of Health Pearls: The Complete Medical ExaminationFrom EverandThe Slim Book of Health Pearls: The Complete Medical ExaminationNo ratings yet
- Med School 101 for Patients: A Patient’S Guide to Creating an Exceptional Doctor VisitFrom EverandMed School 101 for Patients: A Patient’S Guide to Creating an Exceptional Doctor VisitNo ratings yet
- Finding Help & Support: Whatyou Need To KnowDocument5 pagesFinding Help & Support: Whatyou Need To KnowDarren TranNo ratings yet
- Social Media: Whatyou Need To KnowDocument7 pagesSocial Media: Whatyou Need To KnowDarren TranNo ratings yet
- Bullying: Whatyou Need To KnowDocument7 pagesBullying: Whatyou Need To KnowDarren TranNo ratings yet
- Dealing With Workplace Concerns: Whatyou Need To KnowDocument6 pagesDealing With Workplace Concerns: Whatyou Need To KnowDarren TranNo ratings yet
- Issues Facing Australia's Health Care System: Click To Edit Master Subtitle StyleDocument21 pagesIssues Facing Australia's Health Care System: Click To Edit Master Subtitle StyleDarren TranNo ratings yet
- Alyssa Locken Resume Jan 2021Document3 pagesAlyssa Locken Resume Jan 2021api-544203584No ratings yet
- Analysis and Design of AlgorithmsDocument15 pagesAnalysis and Design of AlgorithmsShivani SrivastavaNo ratings yet
- Chapter 7:project Cost ManagementDocument49 pagesChapter 7:project Cost ManagementM. Talha NadeemNo ratings yet
- Evolution of Cyberlaws in The Philippines (10 Mins.)Document14 pagesEvolution of Cyberlaws in The Philippines (10 Mins.)Narciso Reyes Jr.No ratings yet
- Quiz Ch. 6&7 Statistics & FractionsDocument2 pagesQuiz Ch. 6&7 Statistics & FractionsAkbar Suhendi TeacherNo ratings yet
- Exxon Mobil New Refinery TrendsDocument45 pagesExxon Mobil New Refinery TrendsWong Yee Sun100% (1)
- 2 Replacement AnalysisDocument10 pages2 Replacement AnalysisKrishna BirlaNo ratings yet
- ME 4226 Heat Exchanger Compiled WconclusionDocument26 pagesME 4226 Heat Exchanger Compiled Wconclusionhamish888No ratings yet
- ARM7 Based Smart ATM Access & Security System Using Fingerprint Recognition & GSM TechnologyDocument5 pagesARM7 Based Smart ATM Access & Security System Using Fingerprint Recognition & GSM TechnologyBhaskar Rao PNo ratings yet
- Medical Equipment: Www. .Co - KRDocument12 pagesMedical Equipment: Www. .Co - KRBahroel Al mukarram al hajariNo ratings yet
- CV TemplateDocument1 pageCV TemplateLiza Fitri SyarselaNo ratings yet
- Python ProgramsDocument12 pagesPython ProgramsvijayNo ratings yet
- Lis Pendens NoticeDocument2 pagesLis Pendens Noticemarc47No ratings yet
- Concrete Test-Hammer TestDocument1 pageConcrete Test-Hammer Testemut_mNo ratings yet
- Sta 9 1Document125 pagesSta 9 1Jayaprakash Polimetla100% (1)
- University of Cagayan Valley: College Freshmen Program (CFP)Document13 pagesUniversity of Cagayan Valley: College Freshmen Program (CFP)Turingan, Ranz Gabriel, D.No ratings yet
- Kidde Spec AEGIS 2010Document9 pagesKidde Spec AEGIS 2010Jorge InostrozaNo ratings yet
- Principles of Insurance GENERAL INSURANCE (Non Life)Document4 pagesPrinciples of Insurance GENERAL INSURANCE (Non Life)Nipun DhingraNo ratings yet
- FortiNAC-9 4 4-Release - NotesDocument73 pagesFortiNAC-9 4 4-Release - NotesHalil DemirNo ratings yet
- Walkathon Brochure - 2021 Trifold 2Document2 pagesWalkathon Brochure - 2021 Trifold 2api-208159640No ratings yet
- Indonesia Gas Development UtilizationDocument22 pagesIndonesia Gas Development Utilizationchimmy chinNo ratings yet
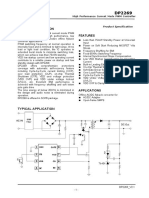
- DP2269Document7 pagesDP2269GABRIEL AMORIM ARAUJONo ratings yet
- Assessment of CG in The Phil PDFDocument34 pagesAssessment of CG in The Phil PDFJoyce Kay AzucenaNo ratings yet
- RXDC - My RayDocument2 pagesRXDC - My RayMedical DXBNo ratings yet
- 2021 10 YR SWM PLAN With Guideliness Drop OffDocument160 pages2021 10 YR SWM PLAN With Guideliness Drop OffALMA BELLA M. PRADONo ratings yet
- SWOT Analysis: University of TampereDocument5 pagesSWOT Analysis: University of TamperearunradNo ratings yet
- InterviewDocument15 pagesInterviewRMRE UETNo ratings yet
- Pest & Steep AnalysisDocument16 pagesPest & Steep Analysismamasita25No ratings yet
- Exercise Chapters 1-5 No SolutionDocument7 pagesExercise Chapters 1-5 No SolutionTrâm Lê Ngọc BảoNo ratings yet