Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5823)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Lean Mass DietDocument92 pagesThe Lean Mass Dietmortless83% (6)
- Unit 7: Procedures and PrecautionsDocument7 pagesUnit 7: Procedures and PrecautionsTrần Vũ LuânNo ratings yet
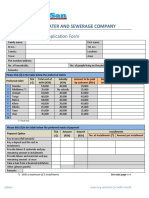
- Oloolaiser Water and Sewerage Company: Safisan Toilet Application FormDocument2 pagesOloolaiser Water and Sewerage Company: Safisan Toilet Application Formauguste singbeogoNo ratings yet
- Linking Socio Demographics of Meat Vendor ProcessorsDocument9 pagesLinking Socio Demographics of Meat Vendor ProcessorsStephanie AquinoNo ratings yet
- 20 Art Therapy Prompts For Kids - AOP HomeschoolingDocument2 pages20 Art Therapy Prompts For Kids - AOP HomeschoolingryantiNo ratings yet
- Week 8 Respiratory System Weekly Workbook 2022Document22 pagesWeek 8 Respiratory System Weekly Workbook 2022rishabhvasisht03No ratings yet
- Summative Test No. 2 in Physical Education - 6 Quarter - 1Document6 pagesSummative Test No. 2 in Physical Education - 6 Quarter - 1Ma. Carmela Balaoro100% (1)
- Sex EducationDocument2 pagesSex EducationsumitchaudharydungerNo ratings yet
- Amici Key CDIDocument21 pagesAmici Key CDIDennis FuerteNo ratings yet
- Safety Data Sheet: Section 1: Identification of The Substance/mixture and of The Company/undertakingDocument8 pagesSafety Data Sheet: Section 1: Identification of The Substance/mixture and of The Company/undertakingjoko setiawanNo ratings yet
- SKP STR FeraDocument32 pagesSKP STR FeraBintari Ancinonyx JubatusNo ratings yet
- Stroke BrochureDocument2 pagesStroke Brochurenananana123No ratings yet
- Group Screening Test Answer SheetDocument18 pagesGroup Screening Test Answer SheetKesserJohnSibongaNo ratings yet
- Factors Affecting The Academic Performance of A Working Student in The Local Government Unit of El Salvador CityDocument15 pagesFactors Affecting The Academic Performance of A Working Student in The Local Government Unit of El Salvador CityAsyed Silayan Zaportiza100% (2)
- Hi Tech Engineering SDN BHD Permit To Work System - Job Hazard AnalysisDocument3 pagesHi Tech Engineering SDN BHD Permit To Work System - Job Hazard AnalysisPHH9834No ratings yet
- Fire Safety Management Strategy in Nigeria Public BuildingsDocument9 pagesFire Safety Management Strategy in Nigeria Public BuildingsWaskita Paspro Seksi 4No ratings yet
- Forensic Identification (TJ)Document38 pagesForensic Identification (TJ)RezaNo ratings yet
- Urinary EliminationDocument7 pagesUrinary EliminationMarcus, RN100% (14)
- Design StudyDocument9 pagesDesign StudySylvia DamayantiNo ratings yet
- Confounding VariableDocument3 pagesConfounding VariableTefera AsresNo ratings yet
- Association Between Prematurity and Diagnosis of Neurodevelopment Disorder: A Case-Control StudyDocument8 pagesAssociation Between Prematurity and Diagnosis of Neurodevelopment Disorder: A Case-Control StudyMônica ScattolinNo ratings yet
- Ra 7431Document67 pagesRa 7431llvnee0No ratings yet
- Communication and Sexual Self Help: Erotica, Kink and The: Fifty Shades of Grey PhenomenonDocument23 pagesCommunication and Sexual Self Help: Erotica, Kink and The: Fifty Shades of Grey PhenomenoncherNo ratings yet
- Reiman Et Al 2017 Cannabis As A Substitute For Opioid Based Pain Medication Patient Self ReportDocument7 pagesReiman Et Al 2017 Cannabis As A Substitute For Opioid Based Pain Medication Patient Self ReportfelipepretelmktNo ratings yet
- PSC Reopening and Recovery Back To Work Checklist (Final - April 20, 2020)Document6 pagesPSC Reopening and Recovery Back To Work Checklist (Final - April 20, 2020)WWMT100% (1)
- PAI Score PiC PDFDocument7 pagesPAI Score PiC PDFNatalia Figueroa Bravo0% (1)
- Dissertation Thesis TamilDocument66 pagesDissertation Thesis TamilTamil Arasi SittaramaneNo ratings yet
- COVID Reference Book Nov 2020Document487 pagesCOVID Reference Book Nov 2020Codrin Darius IlanaNo ratings yet
- My Journal - 081410Document3 pagesMy Journal - 081410Argie abrisNo ratings yet
- Object:-Job Safety Analysis For PDB InstallationDocument1 pageObject:-Job Safety Analysis For PDB Installationpushpanath reddyNo ratings yet