
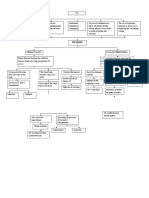
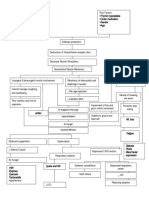
Hypovolemic Shock Pathophysiology: Large Volume Third Spacing Occurs In: Large Volume Third Spacing Occurs in
Hypovolemic Shock Pathophysiology: Large Volume Third Spacing Occurs In: Large Volume Third Spacing Occurs in
You might also like
- Secret Magic Spells of The Romany GypsiesDocument28 pagesSecret Magic Spells of The Romany Gypsiesakenaton4089% (66)
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease Pathophysiologynursing concept maps40% (5)
- I.Mechanical Remarks: Maintenance Checklist For Fan Coil UnitDocument6 pagesI.Mechanical Remarks: Maintenance Checklist For Fan Coil Unitguilmar lopez100% (1)
- Final Myocardial Infarction Pathophysiology PDFDocument3 pagesFinal Myocardial Infarction Pathophysiology PDFDave JoshuaNo ratings yet
- Angina Pectoris PathophysiologyDocument2 pagesAngina Pectoris Pathophysiologydana88% (8)
- The Case of The Missing TimeDocument14 pagesThe Case of The Missing TimeSharingan MangekyouNo ratings yet
- Afib NCPDocument3 pagesAfib NCPGen RodriguezNo ratings yet
- Congestive Heart Failure Pathophysiology Schematic DiagramDocument3 pagesCongestive Heart Failure Pathophysiology Schematic DiagramJasleen KaurNo ratings yet
- Qtsoi Concept MapDocument5 pagesQtsoi Concept MapGenella BabantoNo ratings yet
- Concept Map HypovolemiaDocument3 pagesConcept Map HypovolemiaAllyssa Mackinnon67% (3)
- Pathophysiology of CHF Secondary To RHDDocument89 pagesPathophysiology of CHF Secondary To RHDMira MariantiNo ratings yet
- O SHOCKDocument2 pagesO SHOCKkhurvy999No ratings yet
- ShockDocument29 pagesShockKoRnflakes100% (4)
- PathophysiologyDocument34 pagesPathophysiologyeunams_1195% (20)
- Hemodynamic Disorders Thromboembolic Disease and ShockDocument13 pagesHemodynamic Disorders Thromboembolic Disease and ShockAbu HuraraNo ratings yet
- Neonatal DocingDocument15 pagesNeonatal Docingchar21092000No ratings yet
- NCP ShockDocument5 pagesNCP ShockJanina Patricia BuddleNo ratings yet
- Chapter 7shockDocument62 pagesChapter 7shockEdward XiamNo ratings yet
- Pathophysiology-LCHFDocument2 pagesPathophysiology-LCHFNicole Villanueva, BSN - Level 3ANo ratings yet
- Disorders of Water-Salt Metabolism: Prof. Oleksandr AtamanDocument35 pagesDisorders of Water-Salt Metabolism: Prof. Oleksandr AtamanZAKIA KHALID ALINo ratings yet
- Acute Coronary Syndrome PathophysiologyDocument3 pagesAcute Coronary Syndrome PathophysiologyJocelle Joy OrellanedaNo ratings yet
- NCP-congenital Heat DefectDocument5 pagesNCP-congenital Heat DefectFavor ColaNo ratings yet
- Acute Kidney Injury Secondary To Congestive Heart Failure PathophysiologyDocument1 pageAcute Kidney Injury Secondary To Congestive Heart Failure PathophysiologyKEn PilapilNo ratings yet
- Last Lesson, We Have Studied The Features and The Mechanism of Microcirculatory Ischemic Hypoxia During Shock - Now ContinueDocument27 pagesLast Lesson, We Have Studied The Features and The Mechanism of Microcirculatory Ischemic Hypoxia During Shock - Now Continueapi-19916399No ratings yet
- Holy Angel University Angeles City: School of Nursing and Allied Medical SciencesDocument8 pagesHoly Angel University Angeles City: School of Nursing and Allied Medical SciencesMonica BorjaNo ratings yet
- ShockDocument30 pagesShockLập Trương Minh QuốcNo ratings yet
- An Assignment On Surgery subject:-SHOCK (Definition, Classification and Pathophysiology of Shock)Document8 pagesAn Assignment On Surgery subject:-SHOCK (Definition, Classification and Pathophysiology of Shock)manish soniNo ratings yet
- Edema Dan PerdarahanDocument13 pagesEdema Dan PerdarahanKost Vila SakinahNo ratings yet
- IM-Heart Failure Concept MapDocument16 pagesIM-Heart Failure Concept MapTrisNo ratings yet
- Penetrating Abdominal Trauma (Stab Wound)Document1 pagePenetrating Abdominal Trauma (Stab Wound)P BNo ratings yet
- Jas AssignmentDocument3 pagesJas AssignmentjasperNo ratings yet
- Hypovolemic Shock PathoDocument10 pagesHypovolemic Shock PathoLorebell100% (1)
- Subdural Woc IchaDocument1 pageSubdural Woc IchaNajla KhairunnisaNo ratings yet
- Congestive Heart Failure (CHF) : Causes DiagnosisDocument6 pagesCongestive Heart Failure (CHF) : Causes DiagnosisSOPHIA LOISE TEJANO FULACHENo ratings yet
- Feedback Mechanisms Stimulus Receptor Control Center Effector ResponseDocument1 pageFeedback Mechanisms Stimulus Receptor Control Center Effector ResponsekimNo ratings yet
- All Cardio DiseasesDocument8 pagesAll Cardio Diseaseshiba sharjeelNo ratings yet
- Biology 1 EditedDocument336 pagesBiology 1 EditedEmperor GooseNo ratings yet
- Pathophysiolgoy Coronary Artery DiseaseDocument3 pagesPathophysiolgoy Coronary Artery DiseaseNursesLabs.comNo ratings yet
- Circulatory ShockDocument4 pagesCirculatory ShockDasha VeeNo ratings yet
- Shock Etiology Signs Treatment: Cardiogenic (Pump Failure)Document2 pagesShock Etiology Signs Treatment: Cardiogenic (Pump Failure)paulNo ratings yet
- PCOL CV - Lecture Notes 3 PCOL CV - Lecture Notes 3: Pharmacy (San Pedro College) Pharmacy (San Pedro College)Document9 pagesPCOL CV - Lecture Notes 3 PCOL CV - Lecture Notes 3: Pharmacy (San Pedro College) Pharmacy (San Pedro College)Mhiel Bhon RamzNo ratings yet
- Hemodynamic DisordersDocument10 pagesHemodynamic DisordersUshuaia Ira Marie L. GallaronNo ratings yet
- 2.7 WOC of Intra DyalisisDocument2 pages2.7 WOC of Intra Dyalisisvictor zhefaNo ratings yet
- Week 7 Fluid Volume Imbalances: SoluteDocument8 pagesWeek 7 Fluid Volume Imbalances: SoluteMaica LectanaNo ratings yet
- X.0Y Control of Peripheral Circulation: OutlineDocument4 pagesX.0Y Control of Peripheral Circulation: OutlineAya ARNo ratings yet
- Fluids and Electrolytes IV FluidsDocument1 pageFluids and Electrolytes IV Fluidsnursing concept mapsNo ratings yet
- Hypovolemic Shock: Risk FactorDocument4 pagesHypovolemic Shock: Risk Factorsami khanNo ratings yet
- Multisystem ProblemsDocument90 pagesMultisystem ProblemsAlexander Blanche PajelaNo ratings yet
- Blood PressureDocument27 pagesBlood PressureSreedeep TejaNo ratings yet
- Pathophysiology FilnaleDocument1 pagePathophysiology FilnaleJehmima Gloriani0% (1)
- 019 - Cardiovascular Pathology) Types of Shock - Hypovolemic, Cardiogenic, & Obstructive ShockDocument6 pages019 - Cardiovascular Pathology) Types of Shock - Hypovolemic, Cardiogenic, & Obstructive ShockAmalia PutriNo ratings yet
- Precipitating Factors:: Myocardial Cell Death (NecrosisDocument2 pagesPrecipitating Factors:: Myocardial Cell Death (NecrosisLean Ashly MacarubboNo ratings yet
- Shock NotesDocument4 pagesShock NotesKenneth UbaldeNo ratings yet
- ch30 NotesDocument15 pagesch30 NotesMonica JubaneNo ratings yet
- Cardiovascular SystemDocument20 pagesCardiovascular SystemFisco DessereiNo ratings yet
- Leg Swelling Fluid Balance: Urine Insensible Fluid LossDocument9 pagesLeg Swelling Fluid Balance: Urine Insensible Fluid LossDarwithaNo ratings yet
- Icu 4Document7 pagesIcu 4GemilleDaphneAndradaNo ratings yet
- All PathoDocument2 pagesAll PathoroseasNo ratings yet
- PART VI. Hemodynamic DisordersDocument11 pagesPART VI. Hemodynamic DisordersGideon YeboahNo ratings yet
- 15 Blood Flow Control Edit NOquesDocument34 pages15 Blood Flow Control Edit NOquesugjdk djfgNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument3 pagesN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- (KWIST) Preliminary Exam 27/30 Bl-Ge-6102-Lec-1923T The Contemporary WorldDocument22 pages(KWIST) Preliminary Exam 27/30 Bl-Ge-6102-Lec-1923T The Contemporary WorldMardie ArcesNo ratings yet
- Quiz 3, Quiz 4, Midterm Bl-Ge-6115-Lec-1923T Art AppreciationDocument29 pagesQuiz 3, Quiz 4, Midterm Bl-Ge-6115-Lec-1923T Art AppreciationMardie ArcesNo ratings yet
- Post Test On Food and Water Borne DiseasesDocument4 pagesPost Test On Food and Water Borne DiseasesMardie ArcesNo ratings yet
- Bulaybulay (Qualitative Research Critique)Document3 pagesBulaybulay (Qualitative Research Critique)Mardie ArcesNo ratings yet
- Kidney F Post TestDocument4 pagesKidney F Post TestMardie ArcesNo ratings yet
- What Is Diarrhea?: Contaminated Food Flu Norovirus RotavirusDocument3 pagesWhat Is Diarrhea?: Contaminated Food Flu Norovirus RotavirusMardie ArcesNo ratings yet
- Post Test Upper Gi BleedingDocument4 pagesPost Test Upper Gi BleedingMardie ArcesNo ratings yet
- Bulaybulay - Ca ScenarioDocument5 pagesBulaybulay - Ca ScenarioMardie ArcesNo ratings yet
- The Problem and Its ScopeDocument3 pagesThe Problem and Its ScopeMardie ArcesNo ratings yet
- Directions: Please Use The Following Scale To Answer The Questions Below: (1) Not at All (2) To A Small ExtentDocument1 pageDirections: Please Use The Following Scale To Answer The Questions Below: (1) Not at All (2) To A Small ExtentMardie ArcesNo ratings yet
- IO FormDocument1 pageIO FormMardie ArcesNo ratings yet
- Bulaybulay (Leadership Ass.)Document4 pagesBulaybulay (Leadership Ass.)Mardie ArcesNo ratings yet
- College of Nursing College of Nursing College of Nursing College of NursingDocument8 pagesCollege of Nursing College of Nursing College of Nursing College of NursingMardie ArcesNo ratings yet
- Bandaging Procedure Checklist: Steps Satisfactory UN Satisfactory Remarks PurposeDocument2 pagesBandaging Procedure Checklist: Steps Satisfactory UN Satisfactory Remarks PurposeMardie Arces100% (5)
- Mardie ArcesDocument23 pagesMardie ArcesMardie ArcesNo ratings yet
- ArcesDocument1 pageArcesMardie ArcesNo ratings yet
- Different Forms of Tobacco: Cigarettes Cigars, Little Cigars, CigarillosDocument6 pagesDifferent Forms of Tobacco: Cigarettes Cigars, Little Cigars, CigarillosMardie ArcesNo ratings yet
- EmmmDocument1 pageEmmmMardie ArcesNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument1 pageN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- THISDocument5 pagesTHISMardie ArcesNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument3 pagesN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- I. Family Structures and Characteristics Age Educational AttainmentDocument3 pagesI. Family Structures and Characteristics Age Educational AttainmentMardie ArcesNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument2 pagesN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- Excuse LetterDocument1 pageExcuse LetterMardie ArcesNo ratings yet
- Arces (Elective 141-Lectures)Document18 pagesArces (Elective 141-Lectures)Mardie ArcesNo ratings yet
- Chapter 6 The Skin and The Integumentary SystemDocument2 pagesChapter 6 The Skin and The Integumentary SystemMardie ArcesNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument2 pagesN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- AssignmentDocument6 pagesAssignmentMardie ArcesNo ratings yet
- The Nervous System Is Anorgan Systemcontaining Anetworkof Specializedcells CalledneuronsthatDocument2 pagesThe Nervous System Is Anorgan Systemcontaining Anetworkof Specializedcells CalledneuronsthatMardie ArcesNo ratings yet
- Environmental, Social, and Economic Costs of Recycled Plastic BiocompositesDocument21 pagesEnvironmental, Social, and Economic Costs of Recycled Plastic BiocompositesPasan SubasingheNo ratings yet
- SK CatalougeDocument16 pagesSK CatalougeDevvratNo ratings yet
- Tiruvannamalai and RajinikanthDocument2 pagesTiruvannamalai and RajinikanthashokhaNo ratings yet
- Monash Sustainability Institute - Annual Activity Report 2013Document76 pagesMonash Sustainability Institute - Annual Activity Report 2013Monash Sustainability InstituteNo ratings yet
- Fdpc8016S: Powertrench Power Clip 25V Asymmetric Dual N-Channel MosfetDocument12 pagesFdpc8016S: Powertrench Power Clip 25V Asymmetric Dual N-Channel MosfetRDNo ratings yet
- Grover WasherDocument51 pagesGrover WasherFourHorsemenNo ratings yet
- Towards An Integrated Photonics-Based RadarDocument4 pagesTowards An Integrated Photonics-Based RadarSuzanne MeloNo ratings yet
- Prakash Jhunjhunwala & Co LLP: Chartered AccountantsDocument9 pagesPrakash Jhunjhunwala & Co LLP: Chartered AccountantsKinshuk SinghNo ratings yet
- Horizontal Jaw RelationsDocument90 pagesHorizontal Jaw RelationsKeerthiga TamilarasanNo ratings yet
- PARAS, Mark Heinrich B. - Exercise 3 - Lecture Biochemistry CHEM 40 BSN 1EDocument4 pagesPARAS, Mark Heinrich B. - Exercise 3 - Lecture Biochemistry CHEM 40 BSN 1EMark Heinrich B. ParasNo ratings yet
- Intrauterine Growth RestrictionDocument7 pagesIntrauterine Growth RestrictionNurfazlinaNo ratings yet
- Preliminary Design Document: GE401-Innovative Product Design & Development IDocument15 pagesPreliminary Design Document: GE401-Innovative Product Design & Development IvfoodNo ratings yet
- Stick Cylinder - EspecificationsDocument4 pagesStick Cylinder - EspecificationsFredy Alvarez CespedesNo ratings yet
- Soal USP BIG LMDocument56 pagesSoal USP BIG LMMoh. Aska FailandriNo ratings yet
- Onkyo H500MDocument2 pagesOnkyo H500Mmttw010No ratings yet
- Tabela SMDDocument80 pagesTabela SMDUdenir Jeus de moraisNo ratings yet
- Test BenchDocument16 pagesTest BenchAdriana VeronicaNo ratings yet
- Application of Passive Solar SystemDocument38 pagesApplication of Passive Solar SystemRam Krishna SinghNo ratings yet
- DimpuDocument27 pagesDimpuDippu SihombingNo ratings yet
- LunchDocument29 pagesLunchOmar KhatabNo ratings yet
- Silage Pile Sizing Documentation 5 12 2016 3Document9 pagesSilage Pile Sizing Documentation 5 12 2016 3Zaqueu Ferreira RodriguesNo ratings yet
- 20mm-Thick Cement Plastering in Cement MortarDocument8 pages20mm-Thick Cement Plastering in Cement MortarDeenNo ratings yet
- THE Lymphatic System & Body DefensesDocument39 pagesTHE Lymphatic System & Body DefensesSaiful AmriNo ratings yet
- Red Oxide Primer (ENG)Document3 pagesRed Oxide Primer (ENG)Evan BadakNo ratings yet
- Sesiones de Technical EnglishDocument90 pagesSesiones de Technical EnglishBill Klinthon Chiara100% (1)
- Week 4 - Stadelman-Cohen & Hillman (2014)Document22 pagesWeek 4 - Stadelman-Cohen & Hillman (2014)kehanNo ratings yet
- Chapter 7 Types of Food and Beverage ServiceDocument23 pagesChapter 7 Types of Food and Beverage ServiceJessicaNo ratings yet
















































































































Download as docx, pdf, or txt
You might also like
- Secret Magic Spells of The Romany GypsiesDocument28 pagesSecret Magic Spells of The Romany Gypsiesakenaton4089% (66)
- Coronary Artery Disease PathophysiologyDocument3 pagesCoronary Artery Disease Pathophysiologynursing concept maps40% (5)
- I.Mechanical Remarks: Maintenance Checklist For Fan Coil UnitDocument6 pagesI.Mechanical Remarks: Maintenance Checklist For Fan Coil Unitguilmar lopez100% (1)
- Final Myocardial Infarction Pathophysiology PDFDocument3 pagesFinal Myocardial Infarction Pathophysiology PDFDave JoshuaNo ratings yet
- Angina Pectoris PathophysiologyDocument2 pagesAngina Pectoris Pathophysiologydana88% (8)
- The Case of The Missing TimeDocument14 pagesThe Case of The Missing TimeSharingan MangekyouNo ratings yet
- Afib NCPDocument3 pagesAfib NCPGen RodriguezNo ratings yet
- Congestive Heart Failure Pathophysiology Schematic DiagramDocument3 pagesCongestive Heart Failure Pathophysiology Schematic DiagramJasleen KaurNo ratings yet
- Qtsoi Concept MapDocument5 pagesQtsoi Concept MapGenella BabantoNo ratings yet
- Concept Map HypovolemiaDocument3 pagesConcept Map HypovolemiaAllyssa Mackinnon67% (3)
- Pathophysiology of CHF Secondary To RHDDocument89 pagesPathophysiology of CHF Secondary To RHDMira MariantiNo ratings yet
- O SHOCKDocument2 pagesO SHOCKkhurvy999No ratings yet
- ShockDocument29 pagesShockKoRnflakes100% (4)
- PathophysiologyDocument34 pagesPathophysiologyeunams_1195% (20)
- Hemodynamic Disorders Thromboembolic Disease and ShockDocument13 pagesHemodynamic Disorders Thromboembolic Disease and ShockAbu HuraraNo ratings yet
- Neonatal DocingDocument15 pagesNeonatal Docingchar21092000No ratings yet
- NCP ShockDocument5 pagesNCP ShockJanina Patricia BuddleNo ratings yet
- Chapter 7shockDocument62 pagesChapter 7shockEdward XiamNo ratings yet
- Pathophysiology-LCHFDocument2 pagesPathophysiology-LCHFNicole Villanueva, BSN - Level 3ANo ratings yet
- Disorders of Water-Salt Metabolism: Prof. Oleksandr AtamanDocument35 pagesDisorders of Water-Salt Metabolism: Prof. Oleksandr AtamanZAKIA KHALID ALINo ratings yet
- Acute Coronary Syndrome PathophysiologyDocument3 pagesAcute Coronary Syndrome PathophysiologyJocelle Joy OrellanedaNo ratings yet
- NCP-congenital Heat DefectDocument5 pagesNCP-congenital Heat DefectFavor ColaNo ratings yet
- Acute Kidney Injury Secondary To Congestive Heart Failure PathophysiologyDocument1 pageAcute Kidney Injury Secondary To Congestive Heart Failure PathophysiologyKEn PilapilNo ratings yet
- Last Lesson, We Have Studied The Features and The Mechanism of Microcirculatory Ischemic Hypoxia During Shock - Now ContinueDocument27 pagesLast Lesson, We Have Studied The Features and The Mechanism of Microcirculatory Ischemic Hypoxia During Shock - Now Continueapi-19916399No ratings yet
- Holy Angel University Angeles City: School of Nursing and Allied Medical SciencesDocument8 pagesHoly Angel University Angeles City: School of Nursing and Allied Medical SciencesMonica BorjaNo ratings yet
- ShockDocument30 pagesShockLập Trương Minh QuốcNo ratings yet
- An Assignment On Surgery subject:-SHOCK (Definition, Classification and Pathophysiology of Shock)Document8 pagesAn Assignment On Surgery subject:-SHOCK (Definition, Classification and Pathophysiology of Shock)manish soniNo ratings yet
- Edema Dan PerdarahanDocument13 pagesEdema Dan PerdarahanKost Vila SakinahNo ratings yet
- IM-Heart Failure Concept MapDocument16 pagesIM-Heart Failure Concept MapTrisNo ratings yet
- Penetrating Abdominal Trauma (Stab Wound)Document1 pagePenetrating Abdominal Trauma (Stab Wound)P BNo ratings yet
- Jas AssignmentDocument3 pagesJas AssignmentjasperNo ratings yet
- Hypovolemic Shock PathoDocument10 pagesHypovolemic Shock PathoLorebell100% (1)
- Subdural Woc IchaDocument1 pageSubdural Woc IchaNajla KhairunnisaNo ratings yet
- Congestive Heart Failure (CHF) : Causes DiagnosisDocument6 pagesCongestive Heart Failure (CHF) : Causes DiagnosisSOPHIA LOISE TEJANO FULACHENo ratings yet
- Feedback Mechanisms Stimulus Receptor Control Center Effector ResponseDocument1 pageFeedback Mechanisms Stimulus Receptor Control Center Effector ResponsekimNo ratings yet
- All Cardio DiseasesDocument8 pagesAll Cardio Diseaseshiba sharjeelNo ratings yet
- Biology 1 EditedDocument336 pagesBiology 1 EditedEmperor GooseNo ratings yet
- Pathophysiolgoy Coronary Artery DiseaseDocument3 pagesPathophysiolgoy Coronary Artery DiseaseNursesLabs.comNo ratings yet
- Circulatory ShockDocument4 pagesCirculatory ShockDasha VeeNo ratings yet
- Shock Etiology Signs Treatment: Cardiogenic (Pump Failure)Document2 pagesShock Etiology Signs Treatment: Cardiogenic (Pump Failure)paulNo ratings yet
- PCOL CV - Lecture Notes 3 PCOL CV - Lecture Notes 3: Pharmacy (San Pedro College) Pharmacy (San Pedro College)Document9 pagesPCOL CV - Lecture Notes 3 PCOL CV - Lecture Notes 3: Pharmacy (San Pedro College) Pharmacy (San Pedro College)Mhiel Bhon RamzNo ratings yet
- Hemodynamic DisordersDocument10 pagesHemodynamic DisordersUshuaia Ira Marie L. GallaronNo ratings yet
- 2.7 WOC of Intra DyalisisDocument2 pages2.7 WOC of Intra Dyalisisvictor zhefaNo ratings yet
- Week 7 Fluid Volume Imbalances: SoluteDocument8 pagesWeek 7 Fluid Volume Imbalances: SoluteMaica LectanaNo ratings yet
- X.0Y Control of Peripheral Circulation: OutlineDocument4 pagesX.0Y Control of Peripheral Circulation: OutlineAya ARNo ratings yet
- Fluids and Electrolytes IV FluidsDocument1 pageFluids and Electrolytes IV Fluidsnursing concept mapsNo ratings yet
- Hypovolemic Shock: Risk FactorDocument4 pagesHypovolemic Shock: Risk Factorsami khanNo ratings yet
- Multisystem ProblemsDocument90 pagesMultisystem ProblemsAlexander Blanche PajelaNo ratings yet
- Blood PressureDocument27 pagesBlood PressureSreedeep TejaNo ratings yet
- Pathophysiology FilnaleDocument1 pagePathophysiology FilnaleJehmima Gloriani0% (1)
- 019 - Cardiovascular Pathology) Types of Shock - Hypovolemic, Cardiogenic, & Obstructive ShockDocument6 pages019 - Cardiovascular Pathology) Types of Shock - Hypovolemic, Cardiogenic, & Obstructive ShockAmalia PutriNo ratings yet
- Precipitating Factors:: Myocardial Cell Death (NecrosisDocument2 pagesPrecipitating Factors:: Myocardial Cell Death (NecrosisLean Ashly MacarubboNo ratings yet
- Shock NotesDocument4 pagesShock NotesKenneth UbaldeNo ratings yet
- ch30 NotesDocument15 pagesch30 NotesMonica JubaneNo ratings yet
- Cardiovascular SystemDocument20 pagesCardiovascular SystemFisco DessereiNo ratings yet
- Leg Swelling Fluid Balance: Urine Insensible Fluid LossDocument9 pagesLeg Swelling Fluid Balance: Urine Insensible Fluid LossDarwithaNo ratings yet
- Icu 4Document7 pagesIcu 4GemilleDaphneAndradaNo ratings yet
- All PathoDocument2 pagesAll PathoroseasNo ratings yet
- PART VI. Hemodynamic DisordersDocument11 pagesPART VI. Hemodynamic DisordersGideon YeboahNo ratings yet
- 15 Blood Flow Control Edit NOquesDocument34 pages15 Blood Flow Control Edit NOquesugjdk djfgNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument3 pagesN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- (KWIST) Preliminary Exam 27/30 Bl-Ge-6102-Lec-1923T The Contemporary WorldDocument22 pages(KWIST) Preliminary Exam 27/30 Bl-Ge-6102-Lec-1923T The Contemporary WorldMardie ArcesNo ratings yet
- Quiz 3, Quiz 4, Midterm Bl-Ge-6115-Lec-1923T Art AppreciationDocument29 pagesQuiz 3, Quiz 4, Midterm Bl-Ge-6115-Lec-1923T Art AppreciationMardie ArcesNo ratings yet
- Post Test On Food and Water Borne DiseasesDocument4 pagesPost Test On Food and Water Borne DiseasesMardie ArcesNo ratings yet
- Bulaybulay (Qualitative Research Critique)Document3 pagesBulaybulay (Qualitative Research Critique)Mardie ArcesNo ratings yet
- Kidney F Post TestDocument4 pagesKidney F Post TestMardie ArcesNo ratings yet
- What Is Diarrhea?: Contaminated Food Flu Norovirus RotavirusDocument3 pagesWhat Is Diarrhea?: Contaminated Food Flu Norovirus RotavirusMardie ArcesNo ratings yet
- Post Test Upper Gi BleedingDocument4 pagesPost Test Upper Gi BleedingMardie ArcesNo ratings yet
- Bulaybulay - Ca ScenarioDocument5 pagesBulaybulay - Ca ScenarioMardie ArcesNo ratings yet
- The Problem and Its ScopeDocument3 pagesThe Problem and Its ScopeMardie ArcesNo ratings yet
- Directions: Please Use The Following Scale To Answer The Questions Below: (1) Not at All (2) To A Small ExtentDocument1 pageDirections: Please Use The Following Scale To Answer The Questions Below: (1) Not at All (2) To A Small ExtentMardie ArcesNo ratings yet
- IO FormDocument1 pageIO FormMardie ArcesNo ratings yet
- Bulaybulay (Leadership Ass.)Document4 pagesBulaybulay (Leadership Ass.)Mardie ArcesNo ratings yet
- College of Nursing College of Nursing College of Nursing College of NursingDocument8 pagesCollege of Nursing College of Nursing College of Nursing College of NursingMardie ArcesNo ratings yet
- Bandaging Procedure Checklist: Steps Satisfactory UN Satisfactory Remarks PurposeDocument2 pagesBandaging Procedure Checklist: Steps Satisfactory UN Satisfactory Remarks PurposeMardie Arces100% (5)
- Mardie ArcesDocument23 pagesMardie ArcesMardie ArcesNo ratings yet
- ArcesDocument1 pageArcesMardie ArcesNo ratings yet
- Different Forms of Tobacco: Cigarettes Cigars, Little Cigars, CigarillosDocument6 pagesDifferent Forms of Tobacco: Cigarettes Cigars, Little Cigars, CigarillosMardie ArcesNo ratings yet
- EmmmDocument1 pageEmmmMardie ArcesNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument1 pageN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- THISDocument5 pagesTHISMardie ArcesNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument3 pagesN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- I. Family Structures and Characteristics Age Educational AttainmentDocument3 pagesI. Family Structures and Characteristics Age Educational AttainmentMardie ArcesNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument2 pagesN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- Excuse LetterDocument1 pageExcuse LetterMardie ArcesNo ratings yet
- Arces (Elective 141-Lectures)Document18 pagesArces (Elective 141-Lectures)Mardie ArcesNo ratings yet
- Chapter 6 The Skin and The Integumentary SystemDocument2 pagesChapter 6 The Skin and The Integumentary SystemMardie ArcesNo ratings yet
- N OR S U: Egros Iental Tate NiversityDocument2 pagesN OR S U: Egros Iental Tate NiversityMardie ArcesNo ratings yet
- AssignmentDocument6 pagesAssignmentMardie ArcesNo ratings yet
- The Nervous System Is Anorgan Systemcontaining Anetworkof Specializedcells CalledneuronsthatDocument2 pagesThe Nervous System Is Anorgan Systemcontaining Anetworkof Specializedcells CalledneuronsthatMardie ArcesNo ratings yet
- Environmental, Social, and Economic Costs of Recycled Plastic BiocompositesDocument21 pagesEnvironmental, Social, and Economic Costs of Recycled Plastic BiocompositesPasan SubasingheNo ratings yet
- SK CatalougeDocument16 pagesSK CatalougeDevvratNo ratings yet
- Tiruvannamalai and RajinikanthDocument2 pagesTiruvannamalai and RajinikanthashokhaNo ratings yet
- Monash Sustainability Institute - Annual Activity Report 2013Document76 pagesMonash Sustainability Institute - Annual Activity Report 2013Monash Sustainability InstituteNo ratings yet
- Fdpc8016S: Powertrench Power Clip 25V Asymmetric Dual N-Channel MosfetDocument12 pagesFdpc8016S: Powertrench Power Clip 25V Asymmetric Dual N-Channel MosfetRDNo ratings yet
- Grover WasherDocument51 pagesGrover WasherFourHorsemenNo ratings yet
- Towards An Integrated Photonics-Based RadarDocument4 pagesTowards An Integrated Photonics-Based RadarSuzanne MeloNo ratings yet
- Prakash Jhunjhunwala & Co LLP: Chartered AccountantsDocument9 pagesPrakash Jhunjhunwala & Co LLP: Chartered AccountantsKinshuk SinghNo ratings yet
- Horizontal Jaw RelationsDocument90 pagesHorizontal Jaw RelationsKeerthiga TamilarasanNo ratings yet
- PARAS, Mark Heinrich B. - Exercise 3 - Lecture Biochemistry CHEM 40 BSN 1EDocument4 pagesPARAS, Mark Heinrich B. - Exercise 3 - Lecture Biochemistry CHEM 40 BSN 1EMark Heinrich B. ParasNo ratings yet
- Intrauterine Growth RestrictionDocument7 pagesIntrauterine Growth RestrictionNurfazlinaNo ratings yet
- Preliminary Design Document: GE401-Innovative Product Design & Development IDocument15 pagesPreliminary Design Document: GE401-Innovative Product Design & Development IvfoodNo ratings yet
- Stick Cylinder - EspecificationsDocument4 pagesStick Cylinder - EspecificationsFredy Alvarez CespedesNo ratings yet
- Soal USP BIG LMDocument56 pagesSoal USP BIG LMMoh. Aska FailandriNo ratings yet
- Onkyo H500MDocument2 pagesOnkyo H500Mmttw010No ratings yet
- Tabela SMDDocument80 pagesTabela SMDUdenir Jeus de moraisNo ratings yet
- Test BenchDocument16 pagesTest BenchAdriana VeronicaNo ratings yet
- Application of Passive Solar SystemDocument38 pagesApplication of Passive Solar SystemRam Krishna SinghNo ratings yet
- DimpuDocument27 pagesDimpuDippu SihombingNo ratings yet
- LunchDocument29 pagesLunchOmar KhatabNo ratings yet
- Silage Pile Sizing Documentation 5 12 2016 3Document9 pagesSilage Pile Sizing Documentation 5 12 2016 3Zaqueu Ferreira RodriguesNo ratings yet
- 20mm-Thick Cement Plastering in Cement MortarDocument8 pages20mm-Thick Cement Plastering in Cement MortarDeenNo ratings yet
- THE Lymphatic System & Body DefensesDocument39 pagesTHE Lymphatic System & Body DefensesSaiful AmriNo ratings yet
- Red Oxide Primer (ENG)Document3 pagesRed Oxide Primer (ENG)Evan BadakNo ratings yet
- Sesiones de Technical EnglishDocument90 pagesSesiones de Technical EnglishBill Klinthon Chiara100% (1)
- Week 4 - Stadelman-Cohen & Hillman (2014)Document22 pagesWeek 4 - Stadelman-Cohen & Hillman (2014)kehanNo ratings yet
- Chapter 7 Types of Food and Beverage ServiceDocument23 pagesChapter 7 Types of Food and Beverage ServiceJessicaNo ratings yet