
Mentor Application - Mentoring Children of Prisoners
Mentor Application - Mentoring Children of Prisoners
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Investiture Ceremony For TwinklersDocument2 pagesInvestiture Ceremony For TwinklersOhfallynMae Dela Cruz Quiroz100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Stanley Fine V GallanoDocument2 pagesStanley Fine V GallanoflippchickNo ratings yet
- The Cambridge History of Iran The Saljuq PDFDocument733 pagesThe Cambridge History of Iran The Saljuq PDFKhanzad Barzinjy100% (1)
- Hannibal Country Club September NewsletterDocument2 pagesHannibal Country Club September NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club June NewsletterDocument2 pagesHannibal Country Club June NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club August NewsletterDocument2 pagesHannibal Country Club August NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club November NewsletterDocument2 pagesHannibal Country Club November NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club February NewsletterDocument2 pagesHannibal Country Club February NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club September NewsletterDocument2 pagesHannibal Country Club September NewsletterpooleadvertisingNo ratings yet
- Head Start Annual ReportDocument35 pagesHead Start Annual ReportpooleadvertisingNo ratings yet
- Hannibal Country Club July 2011 NewsletterDocument2 pagesHannibal Country Club July 2011 NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club May 2011 NewsletterDocument2 pagesHannibal Country Club May 2011 NewsletterpooleadvertisingNo ratings yet
- Head Start Needs AssessmentDocument74 pagesHead Start Needs AssessmentpooleadvertisingNo ratings yet
- F&M Bank Winter 2009 NewsletterDocument4 pagesF&M Bank Winter 2009 NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club Newsletter - Sept. 2010Document4 pagesHannibal Country Club Newsletter - Sept. 2010pooleadvertisingNo ratings yet
- F&M Bank - Horizons Calendar 2010Document1 pageF&M Bank - Horizons Calendar 2010pooleadvertisingNo ratings yet
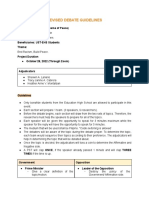
- Revised Debate Guidelines AP Week 2022 1Document3 pagesRevised Debate Guidelines AP Week 2022 1JUSTICE100% (1)
- Ebele Was Expecting A Baby With Her Boyfriend of Ten YearsDocument4 pagesEbele Was Expecting A Baby With Her Boyfriend of Ten YearsAria XoNo ratings yet
- Sophal Ear TranscriptDocument2 pagesSophal Ear TranscriptDiogo MulderNo ratings yet
- Ib Acio Ii 2013Document4 pagesIb Acio Ii 2013SAKETSHOURAVNo ratings yet
- Thyestes NotesDocument2 pagesThyestes NotesauctmetuNo ratings yet
- MH Rmi Review 20Document52 pagesMH Rmi Review 20VMRONo ratings yet
- Deiviocitatic I (Ui',Ublic of Vigt Nam Indcpcndcncc - L:rccdottt - L IappincssDocument6 pagesDeiviocitatic I (Ui',Ublic of Vigt Nam Indcpcndcncc - L:rccdottt - L IappincssPrabir Kumar ChatterjeeNo ratings yet
- 20th Harvard BluebookDocument6 pages20th Harvard BluebookPrasad Hegde100% (1)
- Rules of Procedure DLF Mun 2022Document6 pagesRules of Procedure DLF Mun 2022Arvind GoelNo ratings yet
- A Christmas Plea For Jailed Attorney Richard I Fine To U.S. Supreme Court Justice KennedyDocument4 pagesA Christmas Plea For Jailed Attorney Richard I Fine To U.S. Supreme Court Justice KennedyLeslie DuttonNo ratings yet
- 75 Great Books - Miles MathisDocument12 pages75 Great Books - Miles MathisBillLudley5No ratings yet
- Interchange of Affirmative and Negative Sentences ExercisesDocument3 pagesInterchange of Affirmative and Negative Sentences ExercisesChandan Saha100% (1)
- Shortlited Candidates MTS 22March&1April 1 April 2022Document265 pagesShortlited Candidates MTS 22March&1April 1 April 2022Snighda SenNo ratings yet
- List of Colleges - Khulna CityDocument3 pagesList of Colleges - Khulna CityAfsan MalikNo ratings yet
- 2017 Static GK Capsule by AffairsCloud - V4 PDFDocument109 pages2017 Static GK Capsule by AffairsCloud - V4 PDFpragatiNo ratings yet
- CPCDocument24 pagesCPCAbhinavParasharNo ratings yet
- Trauma, Resilience, and Health PromotionDocument255 pagesTrauma, Resilience, and Health PromotionMunteanu GabyNo ratings yet
- English Challenge (Key)Document5 pagesEnglish Challenge (Key)Thảo GiangNo ratings yet
- The Pokémon Company - Early Settlement Status ReportDocument6 pagesThe Pokémon Company - Early Settlement Status ReportGameInformerMikeNo ratings yet
- Edward Bennett William's Close ArgumentDocument61 pagesEdward Bennett William's Close Argumentorestesbrownson100% (1)
- Noon OptimistDocument1 pageNoon Optimistapi-320724230No ratings yet
- HAL History PDFDocument17 pagesHAL History PDFPoornima SNo ratings yet
- The Future of NATODocument45 pagesThe Future of NATOCouncil on Foreign Relations100% (1)
- BLOOD WARS (TM) Tactics For Two: The Official Two-Player Rules SupplementDocument5 pagesBLOOD WARS (TM) Tactics For Two: The Official Two-Player Rules Supplementplanescraft100% (1)
- Headspace Gage InstructionsDocument2 pagesHeadspace Gage InstructionsryNo ratings yet
- List of "S" Series Civil Standard Forms: Sr. No. Form No. Description of FormDocument4 pagesList of "S" Series Civil Standard Forms: Sr. No. Form No. Description of FormMarwat101No ratings yet
- The Novels of Jose RizalDocument5 pagesThe Novels of Jose RizalJules Emmanuel Nuyad MalaborNo ratings yet

















































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5834)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (824)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (405)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Investiture Ceremony For TwinklersDocument2 pagesInvestiture Ceremony For TwinklersOhfallynMae Dela Cruz Quiroz100% (3)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Stanley Fine V GallanoDocument2 pagesStanley Fine V GallanoflippchickNo ratings yet
- The Cambridge History of Iran The Saljuq PDFDocument733 pagesThe Cambridge History of Iran The Saljuq PDFKhanzad Barzinjy100% (1)
- Hannibal Country Club September NewsletterDocument2 pagesHannibal Country Club September NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club June NewsletterDocument2 pagesHannibal Country Club June NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club August NewsletterDocument2 pagesHannibal Country Club August NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club November NewsletterDocument2 pagesHannibal Country Club November NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club February NewsletterDocument2 pagesHannibal Country Club February NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club September NewsletterDocument2 pagesHannibal Country Club September NewsletterpooleadvertisingNo ratings yet
- Head Start Annual ReportDocument35 pagesHead Start Annual ReportpooleadvertisingNo ratings yet
- Hannibal Country Club July 2011 NewsletterDocument2 pagesHannibal Country Club July 2011 NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club May 2011 NewsletterDocument2 pagesHannibal Country Club May 2011 NewsletterpooleadvertisingNo ratings yet
- Head Start Needs AssessmentDocument74 pagesHead Start Needs AssessmentpooleadvertisingNo ratings yet
- F&M Bank Winter 2009 NewsletterDocument4 pagesF&M Bank Winter 2009 NewsletterpooleadvertisingNo ratings yet
- Hannibal Country Club Newsletter - Sept. 2010Document4 pagesHannibal Country Club Newsletter - Sept. 2010pooleadvertisingNo ratings yet
- F&M Bank - Horizons Calendar 2010Document1 pageF&M Bank - Horizons Calendar 2010pooleadvertisingNo ratings yet
- Revised Debate Guidelines AP Week 2022 1Document3 pagesRevised Debate Guidelines AP Week 2022 1JUSTICE100% (1)
- Ebele Was Expecting A Baby With Her Boyfriend of Ten YearsDocument4 pagesEbele Was Expecting A Baby With Her Boyfriend of Ten YearsAria XoNo ratings yet
- Sophal Ear TranscriptDocument2 pagesSophal Ear TranscriptDiogo MulderNo ratings yet
- Ib Acio Ii 2013Document4 pagesIb Acio Ii 2013SAKETSHOURAVNo ratings yet
- Thyestes NotesDocument2 pagesThyestes NotesauctmetuNo ratings yet
- MH Rmi Review 20Document52 pagesMH Rmi Review 20VMRONo ratings yet
- Deiviocitatic I (Ui',Ublic of Vigt Nam Indcpcndcncc - L:rccdottt - L IappincssDocument6 pagesDeiviocitatic I (Ui',Ublic of Vigt Nam Indcpcndcncc - L:rccdottt - L IappincssPrabir Kumar ChatterjeeNo ratings yet
- 20th Harvard BluebookDocument6 pages20th Harvard BluebookPrasad Hegde100% (1)
- Rules of Procedure DLF Mun 2022Document6 pagesRules of Procedure DLF Mun 2022Arvind GoelNo ratings yet
- A Christmas Plea For Jailed Attorney Richard I Fine To U.S. Supreme Court Justice KennedyDocument4 pagesA Christmas Plea For Jailed Attorney Richard I Fine To U.S. Supreme Court Justice KennedyLeslie DuttonNo ratings yet
- 75 Great Books - Miles MathisDocument12 pages75 Great Books - Miles MathisBillLudley5No ratings yet
- Interchange of Affirmative and Negative Sentences ExercisesDocument3 pagesInterchange of Affirmative and Negative Sentences ExercisesChandan Saha100% (1)
- Shortlited Candidates MTS 22March&1April 1 April 2022Document265 pagesShortlited Candidates MTS 22March&1April 1 April 2022Snighda SenNo ratings yet
- List of Colleges - Khulna CityDocument3 pagesList of Colleges - Khulna CityAfsan MalikNo ratings yet
- 2017 Static GK Capsule by AffairsCloud - V4 PDFDocument109 pages2017 Static GK Capsule by AffairsCloud - V4 PDFpragatiNo ratings yet
- CPCDocument24 pagesCPCAbhinavParasharNo ratings yet
- Trauma, Resilience, and Health PromotionDocument255 pagesTrauma, Resilience, and Health PromotionMunteanu GabyNo ratings yet
- English Challenge (Key)Document5 pagesEnglish Challenge (Key)Thảo GiangNo ratings yet
- The Pokémon Company - Early Settlement Status ReportDocument6 pagesThe Pokémon Company - Early Settlement Status ReportGameInformerMikeNo ratings yet
- Edward Bennett William's Close ArgumentDocument61 pagesEdward Bennett William's Close Argumentorestesbrownson100% (1)
- Noon OptimistDocument1 pageNoon Optimistapi-320724230No ratings yet
- HAL History PDFDocument17 pagesHAL History PDFPoornima SNo ratings yet
- The Future of NATODocument45 pagesThe Future of NATOCouncil on Foreign Relations100% (1)
- BLOOD WARS (TM) Tactics For Two: The Official Two-Player Rules SupplementDocument5 pagesBLOOD WARS (TM) Tactics For Two: The Official Two-Player Rules Supplementplanescraft100% (1)
- Headspace Gage InstructionsDocument2 pagesHeadspace Gage InstructionsryNo ratings yet
- List of "S" Series Civil Standard Forms: Sr. No. Form No. Description of FormDocument4 pagesList of "S" Series Civil Standard Forms: Sr. No. Form No. Description of FormMarwat101No ratings yet
- The Novels of Jose RizalDocument5 pagesThe Novels of Jose RizalJules Emmanuel Nuyad MalaborNo ratings yet