Download as pdf or txt
You might also like
- 12a Diabetic Emergencies DKA Case StudiesDocument13 pages12a Diabetic Emergencies DKA Case StudiesAnonymous yTdBi7100% (1)
- Place 4Document2 pagesPlace 4LiliAra AlvarezNo ratings yet
- QRS 4-2Document1,057 pagesQRS 4-2Sree Harsha Gunneri100% (1)
- DkaDocument32 pagesDkanatheNo ratings yet
- The Neonatal Intensive Care Unit-2Document28 pagesThe Neonatal Intensive Care Unit-2api-457873289No ratings yet
- Clin Management Dka or Hhs Web AlgorithmDocument6 pagesClin Management Dka or Hhs Web AlgorithmChoirotun HisanNo ratings yet
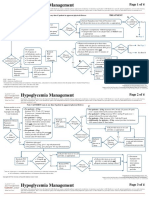
- Hypoglycemia Management: Page 1 of 4Document4 pagesHypoglycemia Management: Page 1 of 4sidharth sauravNo ratings yet
- Kalium Durule Drug StudyDocument2 pagesKalium Durule Drug StudymichelleNo ratings yet
- Grand Rounds Diabetic Ketoacidosis DiseaseDocument52 pagesGrand Rounds Diabetic Ketoacidosis Diseaseapi-740259455No ratings yet
- DKA Protocol With Calculation SheetDocument7 pagesDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNo ratings yet
- Pediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not DiagnosedDocument2 pagesPediatric Diabetic Ketoacidosis (DKA) Algorithm (Page 1-ED) : DKA Diagnosed DKA Not Diagnosedrolland_arrizaNo ratings yet
- Clin Management Hypoglycemia Web AlgorithmDocument4 pagesClin Management Hypoglycemia Web AlgorithmannaNo ratings yet
- Algoritm Acute PancreatitisDocument4 pagesAlgoritm Acute PancreatitisNovi Dwi YantiNo ratings yet
- DKA Guidelines Version 4.0 28 Dec 2016FINALDocument4 pagesDKA Guidelines Version 4.0 28 Dec 2016FINALbenNo ratings yet
- Adult: Diabetic Emergencies: Care Protocol and ChartDocument4 pagesAdult: Diabetic Emergencies: Care Protocol and ChartvladhdNo ratings yet
- Diabetic Care in Acute Febrile IllnessDocument27 pagesDiabetic Care in Acute Febrile IllnessDr-Ajay TripathiNo ratings yet
- DKA NICE GuidelinesDocument6 pagesDKA NICE GuidelinestheonlinegeekhubNo ratings yet
- Diabetic Ketoacidosis: DR Fatima Zahra Associate Professor, Endocrinologist Medicine FRPMCDocument15 pagesDiabetic Ketoacidosis: DR Fatima Zahra Associate Professor, Endocrinologist Medicine FRPMCLaraib KanwalNo ratings yet
- Flow Chart For Diabetic Ketoacidosis in Adults Management ofDocument1 pageFlow Chart For Diabetic Ketoacidosis in Adults Management ofsheryl maeNo ratings yet
- Diabetes MellitusDocument44 pagesDiabetes MellitusHazel CabadduNo ratings yet
- British Guide Algoritmo CetoacidosisDocument2 pagesBritish Guide Algoritmo CetoacidosisMon GuevaraNo ratings yet
- JBDS 02 Single Page Pathway Amended June 2021Document2 pagesJBDS 02 Single Page Pathway Amended June 2021Oliverio MéndezNo ratings yet
- Bsped Dka Guidelines 2020Document23 pagesBsped Dka Guidelines 2020drsaleemNo ratings yet
- Chronic Kidney DiseaseDocument17 pagesChronic Kidney DiseaseJuanchi INNo ratings yet
- Reno Cardio Protection With Canagliflozin - Endo PerspectiveDocument33 pagesReno Cardio Protection With Canagliflozin - Endo PerspectivedrsantoshkalelearningNo ratings yet
- De Guzman, Cameron Josh B. APRIL 26, 2021 2BSN-B RLENCM109Document4 pagesDe Guzman, Cameron Josh B. APRIL 26, 2021 2BSN-B RLENCM109Cameron De GuzmanNo ratings yet
- De Guzman NCP GDMDocument4 pagesDe Guzman NCP GDMCameron De GuzmanNo ratings yet
- Go KCLDocument7 pagesGo KCLSAMANTHA T. MODESTONo ratings yet
- EndocrineDocument10 pagesEndocrineSanjie EufracioNo ratings yet
- Drug Study Form 2Document4 pagesDrug Study Form 2luiNo ratings yet
- Acute Diarrhea and Shock in The EDDocument5 pagesAcute Diarrhea and Shock in The EDmohamed fahmyNo ratings yet
- Assessment: Hyperglycemia, Metabolic Acidosis and Ketonemia - . As Flatbush Diabetes' - (1, 4)Document1 pageAssessment: Hyperglycemia, Metabolic Acidosis and Ketonemia - . As Flatbush Diabetes' - (1, 4)Zunaira AliNo ratings yet
- Mald DKADocument23 pagesMald DKARangel AngelNo ratings yet
- Bsped Dka Guideline 2020Document24 pagesBsped Dka Guideline 2020Valentina Jiménez CárdenasNo ratings yet
- Guidelines and Protocols Of: Diabetes EmergenciesDocument36 pagesGuidelines and Protocols Of: Diabetes Emergenciesyassen hassanNo ratings yet
- Case Based Learning Renal and EndocrineDocument38 pagesCase Based Learning Renal and EndocrineSyeren VenesiaNo ratings yet
- Rearranged By:: 4 Criteria For DKA DXDocument3 pagesRearranged By:: 4 Criteria For DKA DXMuslimNo ratings yet
- 6.03 PcolDocument7 pages6.03 Pcolcruz.cm.sNo ratings yet
- DrugDocument16 pagesDrugtrofacir100% (3)
- CPG Diabetic NephropathyDocument23 pagesCPG Diabetic NephropathyapalaginihNo ratings yet
- DKA MainDocument35 pagesDKA MainKiran GNo ratings yet
- Diabetic Emergencies: Sa'ad Lahri Registrar Dept of Emergency MedicineDocument68 pagesDiabetic Emergencies: Sa'ad Lahri Registrar Dept of Emergency MedicineAs ShahirahNo ratings yet
- Diabetic Emergencies: Sa'ad Lahri Registrar Dept of Emergency MedicineDocument68 pagesDiabetic Emergencies: Sa'ad Lahri Registrar Dept of Emergency MedicineAs ShahirahNo ratings yet
- BWH Hyperglycemia GuidelinesDocument7 pagesBWH Hyperglycemia Guidelinespmahesh107100% (1)
- Nursing Care PlanDocument4 pagesNursing Care PlanDienizs Labini Tadena100% (1)
- MGT of D KetoacidosisDocument5 pagesMGT of D Ketoacidosisshabatat2002No ratings yet
- Diabetic Ketoacidosis Illness ScriptDocument3 pagesDiabetic Ketoacidosis Illness ScriptCarmelaNo ratings yet
- Canine Diabetic Ketoacidosis: Diagnostic Tree /ENDOCRINOLOGYDocument3 pagesCanine Diabetic Ketoacidosis: Diagnostic Tree /ENDOCRINOLOGYPetrisor GheorghiuNo ratings yet
- Dr. Mohamed Ali Hamedh - DKA - 2023Document25 pagesDr. Mohamed Ali Hamedh - DKA - 2023ÁýáFáŕőúgNo ratings yet
- (UHL CHILDREN) Diabetic Ketoacidosis (DKA) PDFDocument12 pages(UHL CHILDREN) Diabetic Ketoacidosis (DKA) PDFRizki Ismi Arsyad IINo ratings yet
- Joint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterDocument1 pageJoint British Diabetes Societies Inpatient Care Group - The Management of Diabetic Ketoacidosis in Adults - Pathway PosterAllison Nadine MarchandNo ratings yet
- สำเนา draft1 - DKA 1Document42 pagesสำเนา draft1 - DKA 1teddypor100% (1)
- NCP DM and HCVDDocument3 pagesNCP DM and HCVDMAYBELINE OBAOB100% (1)
- HyypoglycemiaDocument31 pagesHyypoglycemiaTan Thay HuiNo ratings yet
- Dka GuidelinesDocument24 pagesDka GuidelinesVeena GawaliNo ratings yet
- Cetoacidosis DiabeticaDocument4 pagesCetoacidosis DiabeticaLuis Armando López SosaNo ratings yet
- Diabetic Ketoacidosis PathwayDocument22 pagesDiabetic Ketoacidosis PathwaySri Nath100% (1)
- Diabetes - Routine OPD ManagementDocument3 pagesDiabetes - Routine OPD ManagementKASADHA PATRICKNo ratings yet
- 003 DkaDocument9 pages003 DkaMohammedNo ratings yet
- G HieDocument34 pagesG HieBia BarridoNo ratings yet
- Diabetes in Hospital: A Practical Approach for Healthcare ProfessionalsFrom EverandDiabetes in Hospital: A Practical Approach for Healthcare ProfessionalsNo ratings yet
- Cirilo RDocument12 pagesCirilo RMark Earlmafrey SaguiboNo ratings yet
- Physical Therapist: Entry Level: Please NoteDocument3 pagesPhysical Therapist: Entry Level: Please NoteMafe DiazNo ratings yet
- HHS Public AccessDocument16 pagesHHS Public AccessintanNo ratings yet
- Chest TubeDocument21 pagesChest TubeClaudio Nicolas Retamal YevenesNo ratings yet
- Cases in Medical EthicsDocument8 pagesCases in Medical EthicsOmarNo ratings yet
- Brain Cancer Vaccine Succeeds at Prolonging Survival in Phase 3 TrialDocument1 pageBrain Cancer Vaccine Succeeds at Prolonging Survival in Phase 3 TrialGlen RosselliNo ratings yet
- Ini Cet 22ND July 2021Document8 pagesIni Cet 22ND July 2021gksah711No ratings yet
- Sas 8Document5 pagesSas 8Rodesa MigarNo ratings yet
- Hiv/Aids in Pregnancy: Hassan I.N, Mmed 4Document44 pagesHiv/Aids in Pregnancy: Hassan I.N, Mmed 4HAMIS MASOUDNo ratings yet
- Osmosis ScriptDocument130 pagesOsmosis ScriptJihanNo ratings yet
- Schizophrenia and Psychosis: Group 4 Presentation PharmacologyDocument4 pagesSchizophrenia and Psychosis: Group 4 Presentation PharmacologyVon Valentine MhuteNo ratings yet
- Mata Tenang Visus Turun MendadakDocument34 pagesMata Tenang Visus Turun MendadakTanani 102014007No ratings yet
- NCH Safe Pregnancy BrochureDocument6 pagesNCH Safe Pregnancy BrochurenehahNo ratings yet
- Duty Drug Study'sDocument7 pagesDuty Drug Study'sGrape JuiceNo ratings yet
- 180510-Jf-STARS Blackout Checklist FINALDocument6 pages180510-Jf-STARS Blackout Checklist FINALNithyaNo ratings yet
- Volatile Anaesthetic Myocardial Protection: A Review of The Current LiteratureDocument5 pagesVolatile Anaesthetic Myocardial Protection: A Review of The Current Literatureserena7205No ratings yet
- PHAR 115 Exam 1 Study GuideDocument25 pagesPHAR 115 Exam 1 Study GuideshimkotimNo ratings yet
- Indications For Common Rlung Formulas in Tibetan MedicineDocument8 pagesIndications For Common Rlung Formulas in Tibetan MedicineErikjampaNo ratings yet
- Sulfonamides-Sulfamethoxazole:trimethoprim (Bactrim) - InfenctionsDocument1 pageSulfonamides-Sulfamethoxazole:trimethoprim (Bactrim) - InfenctionsNatalia SpencerNo ratings yet
- Unitedhealthcare Parekh Tpa Pvt. LTDDocument2 pagesUnitedhealthcare Parekh Tpa Pvt. LTDSameer MandgeNo ratings yet
- Hernesniemi S 1001 and More Microneurosurgical VideosDocument193 pagesHernesniemi S 1001 and More Microneurosurgical VideosJoham ChoqueNo ratings yet
- AHA Scientific Statement: Resistant Hypertension: Detection, Evaluation, and ManagementDocument38 pagesAHA Scientific Statement: Resistant Hypertension: Detection, Evaluation, and ManagementPratik TripathiNo ratings yet
- A5 - MOH REGULATIONS - ANNEX 18 - EXTENDED CARE FACILITIES - Ar.enDocument98 pagesA5 - MOH REGULATIONS - ANNEX 18 - EXTENDED CARE FACILITIES - Ar.enAnthimos ChristofiNo ratings yet
- Postural DrainageDocument1 pagePostural Drainagezh4hft6pnzNo ratings yet
- Catch Up FridayDocument4 pagesCatch Up FridayMa. Phoebe AlleoNo ratings yet
- Jurding Saraf Koja - Manitol - Margaretha HDocument24 pagesJurding Saraf Koja - Manitol - Margaretha HMargaretha HimawanNo ratings yet
- Selected Topics: Toxicology: Propofol-Induced Seizure-Like PhenomenaDocument3 pagesSelected Topics: Toxicology: Propofol-Induced Seizure-Like PhenomenaRenan Toledo SandaloNo ratings yet
- Papanicolaou StainDocument2 pagesPapanicolaou StaindeblackaNo ratings yet
- Who Pneu Im Pgi ProtocolDocument2 pagesWho Pneu Im Pgi ProtocolRoxanneGailBigcasGoleroNo ratings yet