Download as pdf or txt
You might also like
- Health Informatics: Practical Guide, Seventh EditionFrom EverandHealth Informatics: Practical Guide, Seventh EditionRating: 5 out of 5 stars5/5 (1)
- Longest's Health Policymaking in the United States, Seventh EditionFrom EverandLongest's Health Policymaking in the United States, Seventh EditionNo ratings yet
- Information Technology for Healthcare Managers, Ninth editionFrom EverandInformation Technology for Healthcare Managers, Ninth editionNo ratings yet
- Health Policymaking in the United States, Sixth EditionFrom EverandHealth Policymaking in the United States, Sixth EditionRating: 2 out of 5 stars2/5 (1)
- Information Systems for Healthcare Management, Eighth EditionFrom EverandInformation Systems for Healthcare Management, Eighth EditionRating: 5 out of 5 stars5/5 (1)
- The Canadian Health Information Management LifecycleFrom EverandThe Canadian Health Information Management LifecycleRating: 4 out of 5 stars4/5 (1)
- Dfy Email: Subject: Manage Your Social Media in 30 MinsDocument1 pageDfy Email: Subject: Manage Your Social Media in 30 MinsDave Nick56% (9)
- Health Informatics: Practical GuideFrom EverandHealth Informatics: Practical GuideWilliam HershNo ratings yet
- Sample California Complaint To Stop Foreclosure Sale by TrusteeDocument3 pagesSample California Complaint To Stop Foreclosure Sale by TrusteeStan Burman100% (5)
- EHR Module 6 PDFDocument4 pagesEHR Module 6 PDFJulie KiselevNo ratings yet
- Ehr Project Proposal Apa KarenDocument10 pagesEhr Project Proposal Apa Karenapi-397532577100% (2)
- Clinical Documentation Improvement (CDI) TrainingDocument6 pagesClinical Documentation Improvement (CDI) Trainingmaricel bismani0% (1)
- Big Data in Healthcare: Statistical Analysis of the Electronic Health RecordFrom EverandBig Data in Healthcare: Statistical Analysis of the Electronic Health RecordNo ratings yet
- A Problem of Display Codes Case StudyDocument7 pagesA Problem of Display Codes Case StudyJam EsNo ratings yet
- Introduction To Master Patient IndexDocument9 pagesIntroduction To Master Patient IndexNishant SharmaNo ratings yet
- Design and Implementation of Electronic Medical Diagnosis System1Document50 pagesDesign and Implementation of Electronic Medical Diagnosis System1Shaguolo O. JosephNo ratings yet
- CAHIMS Handbook - 2019Document24 pagesCAHIMS Handbook - 2019Hema Sai SharmaNo ratings yet
- EHR Planning Your EHR ImplementationDocument44 pagesEHR Planning Your EHR Implementationzbrownlee150% (2)
- Master Patient Index FormDocument2 pagesMaster Patient Index Formapi-355199088No ratings yet
- Conference Proceedings - Vol3 - Short Paper - Final PDFDocument336 pagesConference Proceedings - Vol3 - Short Paper - Final PDFAdriana MuñozNo ratings yet
- Health informatics: Improving patient careFrom EverandHealth informatics: Improving patient careBCS, The Chartered Institute for ITRating: 3 out of 5 stars3/5 (1)
- Medical Records AutomationDocument6 pagesMedical Records Automationluv2golf67No ratings yet
- Guide to Healthcare Information Protection and Privacy for ExecutivesFrom EverandGuide to Healthcare Information Protection and Privacy for ExecutivesNo ratings yet
- Handbook of Biomedical InformaticsDocument748 pagesHandbook of Biomedical Informaticsnelofar100% (4)
- Healthcare and TechnologyDocument14 pagesHealthcare and Technologytrobi017No ratings yet
- A few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentFrom EverandA few minutes to improve Risk documentation Accuracy even when you know nothing about Medicare Risk AdjustmentNo ratings yet
- Tiger Report - Informatics CompetenciesDocument34 pagesTiger Report - Informatics CompetenciesJustus K Gatheru100% (1)
- Master Patient IndexDocument6 pagesMaster Patient IndexAhmed YousefNo ratings yet
- HL7Document13 pagesHL7sony100% (3)
- Electronic Medical Record/Electronic Health Record System: Problem Based LearningDocument13 pagesElectronic Medical Record/Electronic Health Record System: Problem Based LearningTonmoy Banerjee100% (1)
- Electronic Health Records: A Guide For Clinicians and AdministratorsDocument17 pagesElectronic Health Records: A Guide For Clinicians and AdministratorsLIS_141No ratings yet
- AMIA 2015 Self Assessment MOC II Booklet FINALDocument300 pagesAMIA 2015 Self Assessment MOC II Booklet FINALالمعتزبالله جاب اللهNo ratings yet
- Interoperability and Universal Health Care in The PhilippinesDocument4 pagesInteroperability and Universal Health Care in The PhilippinesRvbrRubaNo ratings yet
- Health Information Technology 2014Document641 pagesHealth Information Technology 2014lisa100% (7)
- Electronic Medical Records Management SystemsDocument10 pagesElectronic Medical Records Management Systems44abc100% (1)
- Health Informatics & Legal Issues - DorisDocument59 pagesHealth Informatics & Legal Issues - DorisMonaNo ratings yet
- A simplified Nursing Informatics. A Modern Age Health Technology for Nurses and MidwivesFrom EverandA simplified Nursing Informatics. A Modern Age Health Technology for Nurses and MidwivesNo ratings yet
- Advanced Statistical Methods for Healthcare Research A Complete Guide - 2019 EditionFrom EverandAdvanced Statistical Methods for Healthcare Research A Complete Guide - 2019 EditionNo ratings yet
- 11.r Health InformaticsDocument107 pages11.r Health InformaticsSingla Ashish100% (1)
- An Introduction To LOINC: AMIA 2017 VersionDocument252 pagesAn Introduction To LOINC: AMIA 2017 VersionDaniel Vreeman100% (1)
- Review Paper On Artificial Intelligence in Medical & HealthcareDocument3 pagesReview Paper On Artificial Intelligence in Medical & HealthcareInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Raghupathi-Raghupathi2014 Article BigDataAnalyticsInHealthcarePr PDFDocument10 pagesRaghupathi-Raghupathi2014 Article BigDataAnalyticsInHealthcarePr PDFCristian ZapataNo ratings yet
- Handbook For Electronic Health Records Implementation WHODocument75 pagesHandbook For Electronic Health Records Implementation WHOlaggantigganNo ratings yet
- Analytics Landscape in Healthcare-1Document24 pagesAnalytics Landscape in Healthcare-1positiveworker88No ratings yet
- Health Care Data 101Document17 pagesHealth Care Data 101Tilak Dhar100% (1)
- Hl7 Interface EngineDocument7 pagesHl7 Interface EngineArpithaChamanNo ratings yet
- Computerized Patient Record SystemDocument198 pagesComputerized Patient Record SystemJa Nice100% (2)
- Data Visualization in Healthcare A Complete Guide - 2019 EditionFrom EverandData Visualization in Healthcare A Complete Guide - 2019 EditionNo ratings yet
- Healthcare Domain QuestionsDocument5 pagesHealthcare Domain QuestionsNikhil SatavNo ratings yet
- Electronic Health RecordDocument29 pagesElectronic Health Recordkabir100% (2)
- Healthcare Information System A Complete Guide - 2020 EditionFrom EverandHealthcare Information System A Complete Guide - 2020 EditionNo ratings yet
- Study 3 PDFDocument19 pagesStudy 3 PDFAldwin CantosNo ratings yet
- EHR DocumentationDocument7 pagesEHR DocumentationNursingNowNo ratings yet
- Guide Clinical Data Warehouse Ar 1563726Document3 pagesGuide Clinical Data Warehouse Ar 1563726chan-No ratings yet
- Electronic Health RecordsDocument12 pagesElectronic Health RecordsSahar AlmenwerNo ratings yet
- Medical Informatics: Dr.T.V.Rao MD Professor of MicrobiologyDocument49 pagesMedical Informatics: Dr.T.V.Rao MD Professor of Microbiologytummalapalli venkateswara raoNo ratings yet
- 543 M1 Workbook AssignmentDocument2 pages543 M1 Workbook AssignmentJulie KiselevNo ratings yet
- Security Governance Team Week 1 AssignemtnDocument4 pagesSecurity Governance Team Week 1 AssignemtnJulie KiselevNo ratings yet
- 1 Sterile Processing DepartmentDocument3 pages1 Sterile Processing DepartmentJulie KiselevNo ratings yet
- Business Proposal Project 541 Fall '19Document13 pagesBusiness Proposal Project 541 Fall '19Julie KiselevNo ratings yet
- Working Progress Body of EHRDocument9 pagesWorking Progress Body of EHRJulie KiselevNo ratings yet
- Etta Rose Digital Barcode SheetDocument1 pageEtta Rose Digital Barcode SheetJulie KiselevNo ratings yet
- Vendor Pricing TemplateDocument12 pagesVendor Pricing TemplateJulie KiselevNo ratings yet
- 501 Orientation-Julie+Khmelchenko+Document5 pages501 Orientation-Julie+Khmelchenko+Julie KiselevNo ratings yet
- Week 4 Assignment Group Emotional Intelligence - Julie KhmelchenkoDocument4 pagesWeek 4 Assignment Group Emotional Intelligence - Julie KhmelchenkoJulie KiselevNo ratings yet
- Week 5. EHR Implementation ChallengesDocument4 pagesWeek 5. EHR Implementation ChallengesJulie KiselevNo ratings yet
- Module 6. Transformational Leadership TraitsDocument3 pagesModule 6. Transformational Leadership TraitsJulie KiselevNo ratings yet
- Final Reflective Practice WorksheetDocument6 pagesFinal Reflective Practice WorksheetJulie KiselevNo ratings yet
- Module 5 Self-AssessmentDocument4 pagesModule 5 Self-AssessmentJulie KiselevNo ratings yet
- M4 Final Project Topic and OutlineDocument2 pagesM4 Final Project Topic and OutlineJulie KiselevNo ratings yet
- Roll Number Name Subject Marks Obtained Total Grade Result: 2967917 Bhagesh Ari MauryaDocument3 pagesRoll Number Name Subject Marks Obtained Total Grade Result: 2967917 Bhagesh Ari MauryaShiv PoojanNo ratings yet
- Kid Friendly 8th Grade California State StandardsDocument2 pagesKid Friendly 8th Grade California State StandardsEmily Q. LiuNo ratings yet
- Utilization of Space PDFDocument426 pagesUtilization of Space PDFDiksha DubeyNo ratings yet
- E-Vehicle Article FinalDocument22 pagesE-Vehicle Article Finalvishnu varthanNo ratings yet
- Grade 1 Olympiad My PDFDocument3 pagesGrade 1 Olympiad My PDFConnie Hii100% (1)
- A7X ManualDocument32 pagesA7X ManualStephen LichotaNo ratings yet
- CHN Transes Week 1Document5 pagesCHN Transes Week 1cheskalyka.asiloNo ratings yet
- Kongsberg Cjoy Ot Junction Box: Hardware Module DescriptionDocument26 pagesKongsberg Cjoy Ot Junction Box: Hardware Module DescriptionБогдан МелехедаNo ratings yet
- Collins Sentence MemoDocument17 pagesCollins Sentence MemoRoy S. JohnsonNo ratings yet
- PUSTAK SOOCHI 15 Pages 2022Document16 pagesPUSTAK SOOCHI 15 Pages 2022राहुल चाहरNo ratings yet
- Portfolio Isaac B 1Document17 pagesPortfolio Isaac B 1api-690889230No ratings yet
- Fiber Post Vs Metal PostDocument13 pagesFiber Post Vs Metal PostOdontología UnibeNo ratings yet
- Lean Management Tools in Aviation Industry - New Wine Into Old Wineskins (#1037251) - 2134747Document7 pagesLean Management Tools in Aviation Industry - New Wine Into Old Wineskins (#1037251) - 2134747Mohammed Yassin ChampionNo ratings yet
- Intrusion Detection Systems & HoneypotsDocument33 pagesIntrusion Detection Systems & HoneypotsmanahujaNo ratings yet
- Dissertation Topics CriminologyDocument7 pagesDissertation Topics CriminologyCustomPapersPaterson100% (1)
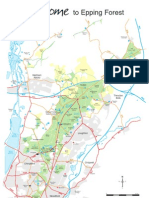
- Epping Forest MapDocument1 pageEpping Forest MapViktor CasualNo ratings yet
- Huge Collection of Finacle MenuDocument26 pagesHuge Collection of Finacle MenurajsundarsNo ratings yet
- L'Altra Montessori School Inc.,: High School Department First Periodical Exam Technology and Livelihood Education 9Document4 pagesL'Altra Montessori School Inc.,: High School Department First Periodical Exam Technology and Livelihood Education 9Kristine HensonNo ratings yet
- CH 6 Properties of Lasers in Introduction To OpticsDocument34 pagesCH 6 Properties of Lasers in Introduction To OpticsmoatazNo ratings yet
- NBTS PlannerDocument1 pageNBTS Planneradriyanmohammed786No ratings yet
- Arts 8Document34 pagesArts 8Joanna joannaNo ratings yet
- PAS 28 - Investments in Associates and Joint Ventures-1Document12 pagesPAS 28 - Investments in Associates and Joint Ventures-1Krizzia DizonNo ratings yet
- Introduction To Law 1.: Meaning and Definition of LawDocument33 pagesIntroduction To Law 1.: Meaning and Definition of LawArthur p90No ratings yet
- Book Project FinalDocument12 pagesBook Project FinalAuguste RiedlNo ratings yet
- B Com English 2016Document12 pagesB Com English 2016PRIYANK PATEL67% (3)
- Discovering Computers Enhanced Edition ©2017: Introducing Today's TechnologiesDocument37 pagesDiscovering Computers Enhanced Edition ©2017: Introducing Today's TechnologiesKent PerezNo ratings yet
- E FilingDocument259 pagesE FilingtestingNo ratings yet
- C5. Catholic Vicar Apostolic of The Mt. Province v. Court of Appeals, 165 SCRA 515Document5 pagesC5. Catholic Vicar Apostolic of The Mt. Province v. Court of Appeals, 165 SCRA 515dondzNo ratings yet