Download as doc, pdf, or txt
You might also like
- Regional Monitoring Report On The Conduct of Different Assessments March 15Document5 pagesRegional Monitoring Report On The Conduct of Different Assessments March 15Nik NokNo ratings yet
- ESOL - Entry 3 - Writing Candidate Paper - Practice Paper C 2Document8 pagesESOL - Entry 3 - Writing Candidate Paper - Practice Paper C 2Sergiu Niculita50% (4)
- 8D Human Error Root Cause Analysis Worksheet Revision Date: 4/3/2018 Revision #: 1Document1 page8D Human Error Root Cause Analysis Worksheet Revision Date: 4/3/2018 Revision #: 1Thee Bouyy100% (1)
- Understanding Operating Systems 7th Edition Mchoes Test BankDocument6 pagesUnderstanding Operating Systems 7th Edition Mchoes Test BankRobertSmithgezya100% (17)
- Ateneo de Zamboanga University: Reflection/Insight Paper - Cerae FormatDocument2 pagesAteneo de Zamboanga University: Reflection/Insight Paper - Cerae FormatSheldon Bazinga100% (8)
- NE212 Spring 2019 Final Exam Guide PDFDocument3 pagesNE212 Spring 2019 Final Exam Guide PDFKyle HuntNo ratings yet
- Isoiec 20000-1 Mapping Guide Final-En PDFDocument16 pagesIsoiec 20000-1 Mapping Guide Final-En PDFIamSajid JatoiNo ratings yet
- Flexibility Method: Worked Example 6.16Document13 pagesFlexibility Method: Worked Example 6.16MohamedNo ratings yet
- Final Performance Standards - 33Document76 pagesFinal Performance Standards - 33JYOTI KATIYAR SVUNo ratings yet
- Job Sheet 1.2 4Document8 pagesJob Sheet 1.2 4Clezel DeL MarNo ratings yet
- Training MatrixDocument2 pagesTraining MatrixJean Bungaos100% (2)
- Training Workshop Activity Evaluation Form 2Document1 pageTraining Workshop Activity Evaluation Form 2Christopher IgnacioNo ratings yet
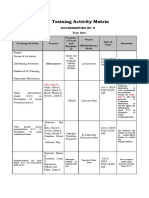
- 01 Training Activity MatrixDocument4 pages01 Training Activity MatrixDave RapsingNo ratings yet
- Vigilance Squad Report For Mscit Exam (Sept 2018) : Yes / NoDocument1 pageVigilance Squad Report For Mscit Exam (Sept 2018) : Yes / NoYogesh ChaudhariNo ratings yet
- Training Activity MatrixDocument2 pagesTraining Activity MatrixKyle Angeles GomezNo ratings yet
- EQ Domestic Biometric Data OperatorDocument4 pagesEQ Domestic Biometric Data OperatorParthibanNo ratings yet
- Rubric Instructor EvaluationDocument2 pagesRubric Instructor EvaluationMesut OzilNo ratings yet
- Excel FileDocument30 pagesExcel FileLawrence Patrick Ladia LimenNo ratings yet
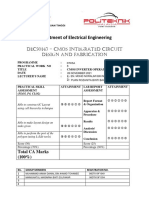
- Department of Electrical Engineering: dEC50143 - CMOS Integrated Circuit Design and FabricationDocument2 pagesDepartment of Electrical Engineering: dEC50143 - CMOS Integrated Circuit Design and FabricationMANNo ratings yet
- UTAR UEMH4413 Sensors and Instrumentation Lab 2Document5 pagesUTAR UEMH4413 Sensors and Instrumentation Lab 2Tan Yuan QingNo ratings yet
- 2013 TCHC Technical Annex Xls 1Document1,369 pages2013 TCHC Technical Annex Xls 1Praditya DhimasNo ratings yet
- Series FormatDocument50 pagesSeries FormatOgabang Cherry C.No ratings yet
- Sample - Session PlanDocument25 pagesSample - Session PlanLorraine LagascaNo ratings yet
- Project Report - 2023-24Document16 pagesProject Report - 2023-24kunalchavan766No ratings yet
- Format of Inspection ReportDocument21 pagesFormat of Inspection Reportlogu044No ratings yet
- Booklet Physics 10-11 - 240528 - 134730Document313 pagesBooklet Physics 10-11 - 240528 - 134730randalkempkesNo ratings yet
- D.ict 1 Computer Laboratory Monitoring ReportDocument4 pagesD.ict 1 Computer Laboratory Monitoring ReportTeacher JoshNo ratings yet
- Guided Notes Edsc 304Document2 pagesGuided Notes Edsc 304api-526335239No ratings yet
- Mathematics 216 Carrousel 2:: Itinerary 8Document2 pagesMathematics 216 Carrousel 2:: Itinerary 8Louis GuyNo ratings yet
- 6 - Session Plan Owen Dae PaDocument5 pages6 - Session Plan Owen Dae PaBilly SalameroNo ratings yet
- Training Activity Trainee Facilities/Tools and Equipment Venue Date & Time Remarks (Workstation/ Area) Training Activity MatrixDocument3 pagesTraining Activity Trainee Facilities/Tools and Equipment Venue Date & Time Remarks (Workstation/ Area) Training Activity Matrixteresa mataincaiNo ratings yet
- Training Activity MatrixDocument3 pagesTraining Activity MatrixDuval LimosNo ratings yet
- LO 2. Use FOS Tools Equipment and ParaphernaliaDocument5 pagesLO 2. Use FOS Tools Equipment and ParaphernaliaReymond SumayloNo ratings yet
- Session Plan - Observe Procedures, Specifications and Manuals of Instruction - JAR & LMN - v1.1Document4 pagesSession Plan - Observe Procedures, Specifications and Manuals of Instruction - JAR & LMN - v1.1Edward RaagasNo ratings yet
- LabManual - PHY2049L.pdf (1) 2Document67 pagesLabManual - PHY2049L.pdf (1) 2juanfelipecadavidherreraNo ratings yet
- SHE Inspection-General - SafetyCultureDocument36 pagesSHE Inspection-General - SafetyCulturematthew kagurabadzaNo ratings yet
- cs0355 Theory of Computation PDFDocument5 pagescs0355 Theory of Computation PDFRituraj choudharyNo ratings yet
- AC Self Assessment Checklist 1Document2 pagesAC Self Assessment Checklist 1Tvet AcnNo ratings yet
- Midterm Exam SolutionsDocument10 pagesMidterm Exam SolutionsAlfin AbdullahNo ratings yet
- Detailed Lesson Plan 5Document5 pagesDetailed Lesson Plan 5France Nicole Joy MoracaNo ratings yet
- Student FeedbackDocument8 pagesStudent FeedbackamitNo ratings yet
- 2019 Sciences Stidrakiya KeyDocument1 page2019 Sciences Stidrakiya KeyACHRAF DOUKARNENo ratings yet
- Andrade - DoodlingDocument7 pagesAndrade - DoodlingRishi ChousalkarNo ratings yet
- Complab Monitoring Report-1Document6 pagesComplab Monitoring Report-1Cheryl Orehuela Colita-LusaresNo ratings yet
- MIKROPLAN PROJECT 4E - Level 1Document4 pagesMIKROPLAN PROJECT 4E - Level 1jelenashijanNo ratings yet
- Lab Write-Up Format and Marking SchemeDocument3 pagesLab Write-Up Format and Marking SchemeritikhNo ratings yet
- ITT300 Individual AssignmentDocument5 pagesITT300 Individual Assignmentizzatanuar04No ratings yet
- Create Your Own Geometry - RubricDocument1 pageCreate Your Own Geometry - Rubricapi-252752147100% (1)
- Checklist of Compliance To Standard Item and Good Practices in TechnologyDocument13 pagesChecklist of Compliance To Standard Item and Good Practices in Technologymbotsrr02newcyclekvkNo ratings yet
- Project Egg Drop Rubric: CategoryDocument2 pagesProject Egg Drop Rubric: CategoryFilipe MagnumNo ratings yet
- Housekeeping Schedule: PC & Printers Training UseDocument12 pagesHousekeeping Schedule: PC & Printers Training UseJepthe Jane MancioNo ratings yet
- Materials Science: Lecture 1, Week 27: Module Introduction and S.I. UnitsDocument83 pagesMaterials Science: Lecture 1, Week 27: Module Introduction and S.I. UnitsQwerty1992ABCNo ratings yet
- Mka 03 (B) Francis TurbineDocument5 pagesMka 03 (B) Francis TurbineHawaiiChongNo ratings yet
- E4 Calendario Inglés UPC 2022-02Document4 pagesE4 Calendario Inglés UPC 2022-02AlvaroNo ratings yet
- OMG 5 English Form 2 - Unit 5Document7 pagesOMG 5 English Form 2 - Unit 5maaran sivamNo ratings yet
- Digital Electronics Ece 213 PDFDocument15 pagesDigital Electronics Ece 213 PDFAlisha AgarwalNo ratings yet
- Wati Consideration Guide - Laura DobbsDocument3 pagesWati Consideration Guide - Laura Dobbsapi-519218367No ratings yet
- Trouble Call ProcessDocument27 pagesTrouble Call ProcessDanNo ratings yet
- Lovely Professional University, Punjab: /lecture-Notes/lecture-29.pdf DFDocument11 pagesLovely Professional University, Punjab: /lecture-Notes/lecture-29.pdf DFAkashdeep SharmaNo ratings yet
- DEMO Presentation 5S Approach in The WorkplaceDocument37 pagesDEMO Presentation 5S Approach in The Workplacelanjhan.abantao12No ratings yet
- Lab Report Assessment Rubrics: Total (%)Document13 pagesLab Report Assessment Rubrics: Total (%)Hafiz NasriNo ratings yet
- Laboratory Experiment Report Rubric: N S: D S: B J M, C K, D J J 10/30/2020 E T E: T DCC M - C L E - GDocument10 pagesLaboratory Experiment Report Rubric: N S: D S: B J M, C K, D J J 10/30/2020 E T E: T DCC M - C L E - GCapalar KyleNo ratings yet
- On Family PlanningDocument30 pagesOn Family PlanningNational Child Health Resource Centre (NCHRC)No ratings yet
- Program Implementation Plans (PIP)Document7 pagesProgram Implementation Plans (PIP)National Child Health Resource Centre (NCHRC)No ratings yet
- Health Systems 2009 20aug ADocument74 pagesHealth Systems 2009 20aug ANational Child Health Resource Centre (NCHRC)No ratings yet
- Health System ComponetsDocument33 pagesHealth System ComponetsNational Child Health Resource Centre (NCHRC)100% (1)
- Quality Training DR Utsuk DattaDocument9 pagesQuality Training DR Utsuk DattaNational Child Health Resource Centre (NCHRC)No ratings yet
- Guidelines For Training Under ARSH For NIHFW 14.7.11Document26 pagesGuidelines For Training Under ARSH For NIHFW 14.7.11National Child Health Resource Centre (NCHRC)50% (2)
- Online Catalogue of Repository On Maternal Child Health (August 2011)Document169 pagesOnline Catalogue of Repository On Maternal Child Health (August 2011)Anil MishraNo ratings yet
- Final Presentation On Training Analysis - 13-15 July 2011Document21 pagesFinal Presentation On Training Analysis - 13-15 July 2011National Child Health Resource Centre (NCHRC)No ratings yet
- Yearly Analysis of The Repository September 2011Document21 pagesYearly Analysis of The Repository September 2011National Child Health Resource Centre (NCHRC)No ratings yet
- Stress MGTDocument21 pagesStress MGTNational Child Health Resource Centre (NCHRC)No ratings yet
- Problems in Health Care Delivery - Shimla.18.5.2010Document72 pagesProblems in Health Care Delivery - Shimla.18.5.2010National Child Health Resource Centre (NCHRC)No ratings yet
- Prof. Deoki Nandan: DirectorDocument52 pagesProf. Deoki Nandan: DirectorNational Child Health Resource Centre (NCHRC)No ratings yet
- Conflict Management: 1 Prof.A.K. Sood NIHFWDocument42 pagesConflict Management: 1 Prof.A.K. Sood NIHFWNational Child Health Resource Centre (NCHRC)No ratings yet
- Ministry of Health & Family WelfareDocument44 pagesMinistry of Health & Family WelfareNational Child Health Resource Centre (NCHRC)No ratings yet
- Political Feasibility and Political Strategies For HRH Policy Reform (Theory Into Practice - The Agra Experience)Document17 pagesPolitical Feasibility and Political Strategies For HRH Policy Reform (Theory Into Practice - The Agra Experience)National Child Health Resource Centre (NCHRC)No ratings yet
- CMO (FW) Certificate ListDocument1 pageCMO (FW) Certificate ListNational Child Health Resource Centre (NCHRC)No ratings yet
- Statement True FalseDocument5 pagesStatement True FalseAbdul Ahad YousafNo ratings yet
- Apache - Hadoop StreamingDocument13 pagesApache - Hadoop Streamingrajan periNo ratings yet
- Harmonic DS NMXDocument3 pagesHarmonic DS NMXBbaPbaNo ratings yet
- VB JoystickDocument8 pagesVB JoystickAshok KumarNo ratings yet
- Auto - Car BarrierDocument70 pagesAuto - Car BarrierkarthiyuvenNo ratings yet
- Flex Catalogue of Tailwind Css Compiled by Muhammad Rizwan - CompressedDocument88 pagesFlex Catalogue of Tailwind Css Compiled by Muhammad Rizwan - Compressedsajid.amz.expertNo ratings yet
- Select Using Work Area Inline Declaration ABAP 7.4Document2 pagesSelect Using Work Area Inline Declaration ABAP 7.4Frbf FrbfbnNo ratings yet
- The Digital Divide and Web 2.0 Collide: The Digital Production GapDocument48 pagesThe Digital Divide and Web 2.0 Collide: The Digital Production Gapschradie50% (2)
- Edius Pro 9: Nonlinear Editing SoftwareDocument7 pagesEdius Pro 9: Nonlinear Editing SoftwareTarak Raj KumarNo ratings yet
- Building An Enterprise CMDB For ITSM-Progress EnergyDocument100 pagesBuilding An Enterprise CMDB For ITSM-Progress Energyshivani_marwahaNo ratings yet
- SeminarDocument12 pagesSeminarPD AneeshNo ratings yet
- Data Sheet: 4-Digit LED-driver With I C-Bus InterfaceDocument19 pagesData Sheet: 4-Digit LED-driver With I C-Bus Interfacegiapy0000No ratings yet
- PanditDocument13 pagesPanditRishabh MehrotraNo ratings yet
- 8086 Program To Generate Fibonacci Sequence - GeeksforGeeksDocument5 pages8086 Program To Generate Fibonacci Sequence - GeeksforGeeksSudhanshu ShekharNo ratings yet
- RackWare Migration BriefDocument4 pagesRackWare Migration BriefAmeena AlsoutiNo ratings yet
- Program No 9: WAP To Print Fibonacci Series Using Copy ConstructorDocument26 pagesProgram No 9: WAP To Print Fibonacci Series Using Copy ConstructorHimanshu SethNo ratings yet
- Fce Exam Class Reading PT 1 Digital DetoxDocument6 pagesFce Exam Class Reading PT 1 Digital Detoxcristiana.2586587No ratings yet
- ESP MonitoringDocument16 pagesESP Monitoringtrunglqvpi100% (1)
- Autodesk AutoCAD Civil 3D V2012Document3 pagesAutodesk AutoCAD Civil 3D V2012leonardofullenkampNo ratings yet
- Syllabus Computer OrganizationDocument3 pagesSyllabus Computer OrganizationRazonable Morales RommelNo ratings yet
- Recorrection Cola-051935 Ns 065Document29 pagesRecorrection Cola-051935 Ns 065Vagish KirubaharanNo ratings yet
- Cinema 4D Install GuideDocument32 pagesCinema 4D Install GuideodinfarwandererNo ratings yet
- 020 Instrument Performance Characteristics PDFDocument17 pages020 Instrument Performance Characteristics PDFBolWolNo ratings yet
- Three Dimensional (3-D) Tooth ATLAS PDFDocument19 pagesThree Dimensional (3-D) Tooth ATLAS PDFwhussien7376No ratings yet
- Personal Computer Installation RubricDocument55 pagesPersonal Computer Installation Rubricellen_ramaNo ratings yet
- Blackmagic Switchers SDK PDFDocument588 pagesBlackmagic Switchers SDK PDFdj_mic100% (1)
- BD BACTEC 9050 Manual 201910916115Document136 pagesBD BACTEC 9050 Manual 201910916115RAULNo ratings yet