
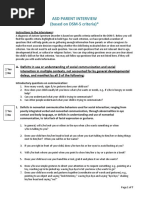
Parent Intake Interview Form
Parent Intake Interview Form
You might also like
- MOCA Sample ReportDocument1 pageMOCA Sample ReportHong Chun Yeoh100% (2)
- Johnstone 2015Document13 pagesJohnstone 2015Siti MinartiNo ratings yet
- Initial Clinical Assessment FormDocument10 pagesInitial Clinical Assessment FormOchee De Guzman CorpusNo ratings yet
- Beck Cognitive Insight ScaleDocument3 pagesBeck Cognitive Insight ScalesrinivasanaNo ratings yet
- Case Conceptualization EhDocument2 pagesCase Conceptualization Ehapi-2393512500% (2)
- Bipolar II Depression Questionnaire-8 Item (BPIIDQ-8) : S2 TableDocument2 pagesBipolar II Depression Questionnaire-8 Item (BPIIDQ-8) : S2 TableLuís Gustavo Ribeiro100% (2)
- 1983 - The Brief Symptom Inventory, An Introductory ReportDocument11 pages1983 - The Brief Symptom Inventory, An Introductory ReportBogdan BaceanuNo ratings yet
- Adolescent Biopsychosocial AssessmentDocument10 pagesAdolescent Biopsychosocial AssessmentFar Sultan100% (2)
- Sample Case History FormDocument4 pagesSample Case History FormHearty Love100% (3)
- AQ AdolescentDocument5 pagesAQ Adolescentdnutter012576No ratings yet
- Yp Core PDFDocument2 pagesYp Core PDFPetra Moala ČipmankNo ratings yet
- Adaptive Behavior Checklist Age Range 6-13Document4 pagesAdaptive Behavior Checklist Age Range 6-13loie anthony nudalo100% (1)
- Addiction Severity Index LiteDocument12 pagesAddiction Severity Index LiteClaudio M. Cruz-Fierro100% (1)
- Autism Diagnostic Observation ScheduleDocument1 pageAutism Diagnostic Observation SchedulenicoletaNo ratings yet
- Vanderbilt Adhd Diagnostic ParentDocument3 pagesVanderbilt Adhd Diagnostic Parentadinaroman100% (1)
- Neuropsychological Evaluation ReportDocument1 pageNeuropsychological Evaluation ReportTrinidad Mercado100% (1)
- NCBRF ScoreSheetDocument3 pagesNCBRF ScoreSheetPryscilla Ugas WisnarNo ratings yet
- Homoeopathic Management of Anxiety Disorders With The Help oDocument240 pagesHomoeopathic Management of Anxiety Disorders With The Help oDr Dushyant Kamal Dhari100% (1)
- Child & Adolescent Intake QuestionnaireDocument15 pagesChild & Adolescent Intake QuestionnaireSadar Psychological and Sports Center100% (2)
- Child and Adolescent HistoryDocument6 pagesChild and Adolescent HistoryRoman KhanNo ratings yet
- Child or Adolescent Client FormsDocument7 pagesChild or Adolescent Client FormsSodfa EttafakshiNo ratings yet
- Child Case History Form CASDocument5 pagesChild Case History Form CASNoor Khalil100% (1)
- Developmental History QuestionnaireDocument6 pagesDevelopmental History QuestionnaireMariana RzNo ratings yet
- Teen QuestionsDocument4 pagesTeen QuestionsANOJ KUMARNo ratings yet
- Developmental History Form 2016Document5 pagesDevelopmental History Form 2016Mariya KhanNo ratings yet
- WISC-V TemplateDocument3 pagesWISC-V TemplateLindsayNo ratings yet
- Childhood Developmental History FormDocument5 pagesChildhood Developmental History FormMariya KhanNo ratings yet
- Kutcher Depression Scale KADS-11Document3 pagesKutcher Depression Scale KADS-11sunnyNo ratings yet
- Adaptive Behavior Scale OutlineDocument3 pagesAdaptive Behavior Scale OutlineZu Gayu 'sNo ratings yet
- Birleson Self-Rating Scale For Child Depressive DisorderDocument4 pagesBirleson Self-Rating Scale For Child Depressive DisordervkNo ratings yet
- GARS - Report FormatDocument1 pageGARS - Report FormatNazema_SagiNo ratings yet
- Neuropsych Eval Report Sample MTBI 2Document4 pagesNeuropsych Eval Report Sample MTBI 2ddb5013No ratings yet
- Child MSEDocument31 pagesChild MSEFaiza ShereefNo ratings yet
- Mental Health Plan Assessment Form: Relationship PhoneDocument6 pagesMental Health Plan Assessment Form: Relationship Phonealotfya100% (1)
- Child Assessment ToolDocument5 pagesChild Assessment ToolIvy Yvonne Quinico MalubagNo ratings yet
- Strengths and Difficulties Questionnaire (SDQ) : Informant Parent Young PersonDocument25 pagesStrengths and Difficulties Questionnaire (SDQ) : Informant Parent Young PersonAdjengIkaWulandari100% (2)
- Cognitive 1Document3 pagesCognitive 1bobbysingersyahooNo ratings yet
- CCC Adhd TestingDocument6 pagesCCC Adhd TestingAnnisa Chaerani Burhanuddin100% (1)
- Check List For Strengths and Needs When Planning For Educational GoalsDocument6 pagesCheck List For Strengths and Needs When Planning For Educational GoalsMbizi Joseph100% (1)
- Attention Deficit/ Hyperactivity Disorder: Changes To The DisorderDocument2 pagesAttention Deficit/ Hyperactivity Disorder: Changes To The DisorderGemanDuenasNo ratings yet
- Sample CBCL NarrativeDocument1 pageSample CBCL NarrativeMohamed Abozeid100% (1)
- BRIEF - IR - Parent - Form SAMPLE PDFDocument10 pagesBRIEF - IR - Parent - Form SAMPLE PDFAna Sofía BolañosNo ratings yet
- Basc-3 Psimas 2hr Masp 2015Document20 pagesBasc-3 Psimas 2hr Masp 2015Jean Yi CheongNo ratings yet
- Vanderbilt ADHDDocument7 pagesVanderbilt ADHDGnaneswar PiduguNo ratings yet
- Screening Questionnaire-1Document3 pagesScreening Questionnaire-1nikhila911No ratings yet
- Adaptive Behavior Assessment System-II: Technical ReportDocument5 pagesAdaptive Behavior Assessment System-II: Technical ReportLisa MariaNo ratings yet
- ADHD Scoring InstructionsDocument1 pageADHD Scoring Instructionsnaseeruddin1No ratings yet
- Psychological Assessment ReportDocument3 pagesPsychological Assessment ReportmobeenNo ratings yet
- Childhood Autism Rating ScaleDocument2 pagesChildhood Autism Rating ScaleAsmaa ElarabyNo ratings yet
- Conners Rating ScaleDocument6 pagesConners Rating ScaleNeeraj MishraNo ratings yet
- Dyslexia BookletN PDFDocument33 pagesDyslexia BookletN PDFDr.V.Sivaprakasam100% (3)
- Asd-Parent-Interview Formatted 2012 0325 PDFDocument7 pagesAsd-Parent-Interview Formatted 2012 0325 PDFVivek SagarNo ratings yet
- Koppitz 2Document14 pagesKoppitz 2mhickomhicko0% (1)
- Assessing Adaptive Behavior in Young ChildrenDocument34 pagesAssessing Adaptive Behavior in Young Childrenlia luthfiahNo ratings yet
- Vanderbilt ADHD Diagnostic Rating ScaleDocument2 pagesVanderbilt ADHD Diagnostic Rating ScalevkNo ratings yet
- Clinical Intake InterviewDocument9 pagesClinical Intake Interviewvaz21No ratings yet
- Collaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeFrom EverandCollaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeAlisha R. PollastriNo ratings yet
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionFrom EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionNo ratings yet
- Ebook - Information Technology Project Management-302-317Document16 pagesEbook - Information Technology Project Management-302-317Milleony TianaNo ratings yet
- Allen Clinical HintsDocument359 pagesAllen Clinical HintsSyed SajidNo ratings yet
- Emotional MasteryDocument837 pagesEmotional MasteryPavanNo ratings yet
- Abm Homer Group 3 Research Paper 2Document18 pagesAbm Homer Group 3 Research Paper 2Aviona Gail RazoNo ratings yet
- Tokyo Ravens - Volume 07 - Darkness - EmergeDocument369 pagesTokyo Ravens - Volume 07 - Darkness - EmergeLhieNo ratings yet
- Levels of Self-Efficacy of Student-MotherDocument17 pagesLevels of Self-Efficacy of Student-MotherPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Dental Fear, Anxiety and Phobia (Final1)Document55 pagesDental Fear, Anxiety and Phobia (Final1)Aj VishwadheebNo ratings yet
- Alternative DSM-5 For PDDocument15 pagesAlternative DSM-5 For PDadffsaNo ratings yet
- "Finding Home": Understanding How Music Supports Listeners' Mental Health Through A Case Study of BtsDocument8 pages"Finding Home": Understanding How Music Supports Listeners' Mental Health Through A Case Study of BtsAribun GayoNo ratings yet
- 10 Common Thinking Traps EBook PDFDocument21 pages10 Common Thinking Traps EBook PDFDeaf Canuck100% (2)
- FEMA - Pastoral Crisis InterventionDocument33 pagesFEMA - Pastoral Crisis InterventionThe Prophetic ExplorerNo ratings yet
- Stress, Coping, and Immune Function in Breast Cancer: Linda J. Luecken, PH.DDocument9 pagesStress, Coping, and Immune Function in Breast Cancer: Linda J. Luecken, PH.Dana rosaNo ratings yet
- Explorando La Suspension de La Incredulidad Durante El Aprendizaje Basado en Las SimulacionesDocument7 pagesExplorando La Suspension de La Incredulidad Durante El Aprendizaje Basado en Las SimulacionesVictoriano MendezNo ratings yet
- Theory CritiqueDocument11 pagesTheory CritiquemelmulanNo ratings yet
- Psychiatry MethodicalDocument65 pagesPsychiatry MethodicalsyhnzNo ratings yet
- Adaptacion Emocional de La Perdida de Una ExtremidadDocument22 pagesAdaptacion Emocional de La Perdida de Una ExtremidadDeborah SalinasNo ratings yet
- Sample of RRLDocument10 pagesSample of RRLAwesome100% (1)
- Mindfullness TeenDocument163 pagesMindfullness TeenCarla Barbosa Rocha100% (5)
- Text News AnchorDocument2 pagesText News AnchorPUTRI SHIFA AULIANo ratings yet
- NCM 111 Group Proposal SampleDocument32 pagesNCM 111 Group Proposal SampleBSN 2 - Sasis, Rusmaryte C.No ratings yet
- IntroductionDocument2 pagesIntroductionmary ann patenoNo ratings yet
- Rosenfield, Sarah. The Effects of Women's Employment Personal Control and Sex Differences in Mental HealthDocument16 pagesRosenfield, Sarah. The Effects of Women's Employment Personal Control and Sex Differences in Mental HealthTengiz VerulavaNo ratings yet
- Miasms Sankaran Sankaran View of Miasms MiasmsDocument46 pagesMiasms Sankaran Sankaran View of Miasms Miasmslilian_vera_150% (2)
- Excerpt From "The Last Walk: Reflections On Our Pets at The End of Their Lives" by Jessica PierceDocument4 pagesExcerpt From "The Last Walk: Reflections On Our Pets at The End of Their Lives" by Jessica Piercewamu885No ratings yet
- A Narrative Report On Mental Health and Psychological Support and Services RJCC REALDocument1 pageA Narrative Report On Mental Health and Psychological Support and Services RJCC REALRoxanne Jessa CatibogNo ratings yet
- Nursing Care Plan: IndependentDocument9 pagesNursing Care Plan: IndependentblairNo ratings yet
- Admission, Discharge, Transfer, and ReferralsDocument5 pagesAdmission, Discharge, Transfer, and ReferralsMohammedNo ratings yet
- Current Status of Soviet Psychotherapy: W. LauterbachDocument4 pagesCurrent Status of Soviet Psychotherapy: W. Lauterbachhelio donadiNo ratings yet
























































































Download as docx, pdf, or txt
You might also like
- MOCA Sample ReportDocument1 pageMOCA Sample ReportHong Chun Yeoh100% (2)
- Johnstone 2015Document13 pagesJohnstone 2015Siti MinartiNo ratings yet
- Initial Clinical Assessment FormDocument10 pagesInitial Clinical Assessment FormOchee De Guzman CorpusNo ratings yet
- Beck Cognitive Insight ScaleDocument3 pagesBeck Cognitive Insight ScalesrinivasanaNo ratings yet
- Case Conceptualization EhDocument2 pagesCase Conceptualization Ehapi-2393512500% (2)
- Bipolar II Depression Questionnaire-8 Item (BPIIDQ-8) : S2 TableDocument2 pagesBipolar II Depression Questionnaire-8 Item (BPIIDQ-8) : S2 TableLuís Gustavo Ribeiro100% (2)
- 1983 - The Brief Symptom Inventory, An Introductory ReportDocument11 pages1983 - The Brief Symptom Inventory, An Introductory ReportBogdan BaceanuNo ratings yet
- Adolescent Biopsychosocial AssessmentDocument10 pagesAdolescent Biopsychosocial AssessmentFar Sultan100% (2)
- Sample Case History FormDocument4 pagesSample Case History FormHearty Love100% (3)
- AQ AdolescentDocument5 pagesAQ Adolescentdnutter012576No ratings yet
- Yp Core PDFDocument2 pagesYp Core PDFPetra Moala ČipmankNo ratings yet
- Adaptive Behavior Checklist Age Range 6-13Document4 pagesAdaptive Behavior Checklist Age Range 6-13loie anthony nudalo100% (1)
- Addiction Severity Index LiteDocument12 pagesAddiction Severity Index LiteClaudio M. Cruz-Fierro100% (1)
- Autism Diagnostic Observation ScheduleDocument1 pageAutism Diagnostic Observation SchedulenicoletaNo ratings yet
- Vanderbilt Adhd Diagnostic ParentDocument3 pagesVanderbilt Adhd Diagnostic Parentadinaroman100% (1)
- Neuropsychological Evaluation ReportDocument1 pageNeuropsychological Evaluation ReportTrinidad Mercado100% (1)
- NCBRF ScoreSheetDocument3 pagesNCBRF ScoreSheetPryscilla Ugas WisnarNo ratings yet
- Homoeopathic Management of Anxiety Disorders With The Help oDocument240 pagesHomoeopathic Management of Anxiety Disorders With The Help oDr Dushyant Kamal Dhari100% (1)
- Child & Adolescent Intake QuestionnaireDocument15 pagesChild & Adolescent Intake QuestionnaireSadar Psychological and Sports Center100% (2)
- Child and Adolescent HistoryDocument6 pagesChild and Adolescent HistoryRoman KhanNo ratings yet
- Child or Adolescent Client FormsDocument7 pagesChild or Adolescent Client FormsSodfa EttafakshiNo ratings yet
- Child Case History Form CASDocument5 pagesChild Case History Form CASNoor Khalil100% (1)
- Developmental History QuestionnaireDocument6 pagesDevelopmental History QuestionnaireMariana RzNo ratings yet
- Teen QuestionsDocument4 pagesTeen QuestionsANOJ KUMARNo ratings yet
- Developmental History Form 2016Document5 pagesDevelopmental History Form 2016Mariya KhanNo ratings yet
- WISC-V TemplateDocument3 pagesWISC-V TemplateLindsayNo ratings yet
- Childhood Developmental History FormDocument5 pagesChildhood Developmental History FormMariya KhanNo ratings yet
- Kutcher Depression Scale KADS-11Document3 pagesKutcher Depression Scale KADS-11sunnyNo ratings yet
- Adaptive Behavior Scale OutlineDocument3 pagesAdaptive Behavior Scale OutlineZu Gayu 'sNo ratings yet
- Birleson Self-Rating Scale For Child Depressive DisorderDocument4 pagesBirleson Self-Rating Scale For Child Depressive DisordervkNo ratings yet
- GARS - Report FormatDocument1 pageGARS - Report FormatNazema_SagiNo ratings yet
- Neuropsych Eval Report Sample MTBI 2Document4 pagesNeuropsych Eval Report Sample MTBI 2ddb5013No ratings yet
- Child MSEDocument31 pagesChild MSEFaiza ShereefNo ratings yet
- Mental Health Plan Assessment Form: Relationship PhoneDocument6 pagesMental Health Plan Assessment Form: Relationship Phonealotfya100% (1)
- Child Assessment ToolDocument5 pagesChild Assessment ToolIvy Yvonne Quinico MalubagNo ratings yet
- Strengths and Difficulties Questionnaire (SDQ) : Informant Parent Young PersonDocument25 pagesStrengths and Difficulties Questionnaire (SDQ) : Informant Parent Young PersonAdjengIkaWulandari100% (2)
- Cognitive 1Document3 pagesCognitive 1bobbysingersyahooNo ratings yet
- CCC Adhd TestingDocument6 pagesCCC Adhd TestingAnnisa Chaerani Burhanuddin100% (1)
- Check List For Strengths and Needs When Planning For Educational GoalsDocument6 pagesCheck List For Strengths and Needs When Planning For Educational GoalsMbizi Joseph100% (1)
- Attention Deficit/ Hyperactivity Disorder: Changes To The DisorderDocument2 pagesAttention Deficit/ Hyperactivity Disorder: Changes To The DisorderGemanDuenasNo ratings yet
- Sample CBCL NarrativeDocument1 pageSample CBCL NarrativeMohamed Abozeid100% (1)
- BRIEF - IR - Parent - Form SAMPLE PDFDocument10 pagesBRIEF - IR - Parent - Form SAMPLE PDFAna Sofía BolañosNo ratings yet
- Basc-3 Psimas 2hr Masp 2015Document20 pagesBasc-3 Psimas 2hr Masp 2015Jean Yi CheongNo ratings yet
- Vanderbilt ADHDDocument7 pagesVanderbilt ADHDGnaneswar PiduguNo ratings yet
- Screening Questionnaire-1Document3 pagesScreening Questionnaire-1nikhila911No ratings yet
- Adaptive Behavior Assessment System-II: Technical ReportDocument5 pagesAdaptive Behavior Assessment System-II: Technical ReportLisa MariaNo ratings yet
- ADHD Scoring InstructionsDocument1 pageADHD Scoring Instructionsnaseeruddin1No ratings yet
- Psychological Assessment ReportDocument3 pagesPsychological Assessment ReportmobeenNo ratings yet
- Childhood Autism Rating ScaleDocument2 pagesChildhood Autism Rating ScaleAsmaa ElarabyNo ratings yet
- Conners Rating ScaleDocument6 pagesConners Rating ScaleNeeraj MishraNo ratings yet
- Dyslexia BookletN PDFDocument33 pagesDyslexia BookletN PDFDr.V.Sivaprakasam100% (3)
- Asd-Parent-Interview Formatted 2012 0325 PDFDocument7 pagesAsd-Parent-Interview Formatted 2012 0325 PDFVivek SagarNo ratings yet
- Koppitz 2Document14 pagesKoppitz 2mhickomhicko0% (1)
- Assessing Adaptive Behavior in Young ChildrenDocument34 pagesAssessing Adaptive Behavior in Young Childrenlia luthfiahNo ratings yet
- Vanderbilt ADHD Diagnostic Rating ScaleDocument2 pagesVanderbilt ADHD Diagnostic Rating ScalevkNo ratings yet
- Clinical Intake InterviewDocument9 pagesClinical Intake Interviewvaz21No ratings yet
- Collaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeFrom EverandCollaborative Problem Solving: An Evidence-Based Approach to Implementation and PracticeAlisha R. PollastriNo ratings yet
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionFrom EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionNo ratings yet
- Ebook - Information Technology Project Management-302-317Document16 pagesEbook - Information Technology Project Management-302-317Milleony TianaNo ratings yet
- Allen Clinical HintsDocument359 pagesAllen Clinical HintsSyed SajidNo ratings yet
- Emotional MasteryDocument837 pagesEmotional MasteryPavanNo ratings yet
- Abm Homer Group 3 Research Paper 2Document18 pagesAbm Homer Group 3 Research Paper 2Aviona Gail RazoNo ratings yet
- Tokyo Ravens - Volume 07 - Darkness - EmergeDocument369 pagesTokyo Ravens - Volume 07 - Darkness - EmergeLhieNo ratings yet
- Levels of Self-Efficacy of Student-MotherDocument17 pagesLevels of Self-Efficacy of Student-MotherPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Dental Fear, Anxiety and Phobia (Final1)Document55 pagesDental Fear, Anxiety and Phobia (Final1)Aj VishwadheebNo ratings yet
- Alternative DSM-5 For PDDocument15 pagesAlternative DSM-5 For PDadffsaNo ratings yet
- "Finding Home": Understanding How Music Supports Listeners' Mental Health Through A Case Study of BtsDocument8 pages"Finding Home": Understanding How Music Supports Listeners' Mental Health Through A Case Study of BtsAribun GayoNo ratings yet
- 10 Common Thinking Traps EBook PDFDocument21 pages10 Common Thinking Traps EBook PDFDeaf Canuck100% (2)
- FEMA - Pastoral Crisis InterventionDocument33 pagesFEMA - Pastoral Crisis InterventionThe Prophetic ExplorerNo ratings yet
- Stress, Coping, and Immune Function in Breast Cancer: Linda J. Luecken, PH.DDocument9 pagesStress, Coping, and Immune Function in Breast Cancer: Linda J. Luecken, PH.Dana rosaNo ratings yet
- Explorando La Suspension de La Incredulidad Durante El Aprendizaje Basado en Las SimulacionesDocument7 pagesExplorando La Suspension de La Incredulidad Durante El Aprendizaje Basado en Las SimulacionesVictoriano MendezNo ratings yet
- Theory CritiqueDocument11 pagesTheory CritiquemelmulanNo ratings yet
- Psychiatry MethodicalDocument65 pagesPsychiatry MethodicalsyhnzNo ratings yet
- Adaptacion Emocional de La Perdida de Una ExtremidadDocument22 pagesAdaptacion Emocional de La Perdida de Una ExtremidadDeborah SalinasNo ratings yet
- Sample of RRLDocument10 pagesSample of RRLAwesome100% (1)
- Mindfullness TeenDocument163 pagesMindfullness TeenCarla Barbosa Rocha100% (5)
- Text News AnchorDocument2 pagesText News AnchorPUTRI SHIFA AULIANo ratings yet
- NCM 111 Group Proposal SampleDocument32 pagesNCM 111 Group Proposal SampleBSN 2 - Sasis, Rusmaryte C.No ratings yet
- IntroductionDocument2 pagesIntroductionmary ann patenoNo ratings yet
- Rosenfield, Sarah. The Effects of Women's Employment Personal Control and Sex Differences in Mental HealthDocument16 pagesRosenfield, Sarah. The Effects of Women's Employment Personal Control and Sex Differences in Mental HealthTengiz VerulavaNo ratings yet
- Miasms Sankaran Sankaran View of Miasms MiasmsDocument46 pagesMiasms Sankaran Sankaran View of Miasms Miasmslilian_vera_150% (2)
- Excerpt From "The Last Walk: Reflections On Our Pets at The End of Their Lives" by Jessica PierceDocument4 pagesExcerpt From "The Last Walk: Reflections On Our Pets at The End of Their Lives" by Jessica Piercewamu885No ratings yet
- A Narrative Report On Mental Health and Psychological Support and Services RJCC REALDocument1 pageA Narrative Report On Mental Health and Psychological Support and Services RJCC REALRoxanne Jessa CatibogNo ratings yet
- Nursing Care Plan: IndependentDocument9 pagesNursing Care Plan: IndependentblairNo ratings yet
- Admission, Discharge, Transfer, and ReferralsDocument5 pagesAdmission, Discharge, Transfer, and ReferralsMohammedNo ratings yet
- Current Status of Soviet Psychotherapy: W. LauterbachDocument4 pagesCurrent Status of Soviet Psychotherapy: W. Lauterbachhelio donadiNo ratings yet