Download as docx, pdf, or txt
You might also like
- Customer Satisfaction of Amul ProductsDocument38 pagesCustomer Satisfaction of Amul ProductsVineet Kumar Aggarwal77% (13)
- Hypothyroidism: Progressive Weight Gain and Decreased AppetiteDocument5 pagesHypothyroidism: Progressive Weight Gain and Decreased AppetiteKrisianne Mae Lorenzo Francisco100% (2)
- A. Physical (Dillon'S Physical Assessment Tool)Document7 pagesA. Physical (Dillon'S Physical Assessment Tool)Jim RashidNo ratings yet
- Warehouse LayoutDocument48 pagesWarehouse LayoutZubair Aslam100% (1)
- NCP For Pancreatic CancerDocument5 pagesNCP For Pancreatic CancerLindy JaneNo ratings yet
- NRS456 - Malnutrition - Written Assignment-2Document12 pagesNRS456 - Malnutrition - Written Assignment-2najwaNo ratings yet
- NCP & Discharge PlanningDocument12 pagesNCP & Discharge PlanningStephanie Mae Amoylen OdchigueNo ratings yet
- NCP For Liver AbcessDocument1 pageNCP For Liver AbcessTroy MirandaNo ratings yet
- Imbalanced Nutrition Less Than Body Requirements Related To Altered Image, Inadequate Nutrient Intake, and Chronic Vomiting.Document2 pagesImbalanced Nutrition Less Than Body Requirements Related To Altered Image, Inadequate Nutrient Intake, and Chronic Vomiting.Senyorita KHaye100% (1)
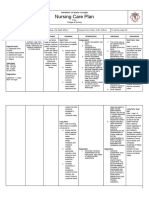
- Nursing Care PlanDocument12 pagesNursing Care PlanScribdTranslationsNo ratings yet
- Altered Nutrition NCPDocument2 pagesAltered Nutrition NCPLeiAnnManaleseNo ratings yet
- NCP For MIDocument5 pagesNCP For MIjaira magbanuaNo ratings yet
- NCPDocument4 pagesNCPAngela Neri0% (1)
- Afinidad, Jiezl A: Davao Doctors College Nursing ProgramDocument4 pagesAfinidad, Jiezl A: Davao Doctors College Nursing ProgramJiezl Abellano AfinidadNo ratings yet
- Interventions For Nutrition PDFDocument19 pagesInterventions For Nutrition PDFSheila LaNo ratings yet
- Activity 5 NCPDocument5 pagesActivity 5 NCPAl-Mujib TanogNo ratings yet
- Nursing Care Plan Patient With Diabetes MellitusDocument5 pagesNursing Care Plan Patient With Diabetes MellitusNajla Khairunnisa100% (1)
- DX Hyperthyoidism PDFDocument10 pagesDX Hyperthyoidism PDFSherree HayesNo ratings yet
- Nursing Care Plan: Saint Louis University School of Nursing Bonifacio Street, Baguio CityDocument3 pagesNursing Care Plan: Saint Louis University School of Nursing Bonifacio Street, Baguio CitySoniaMarieBalanayNo ratings yet
- Cholelithiasis NCP FINALDocument6 pagesCholelithiasis NCP FINALShreshthi VermaNo ratings yet
- Imbalance Nutrition Less Than Body RequirementsDocument4 pagesImbalance Nutrition Less Than Body Requirementshatred heartNo ratings yet
- NCP - Imbalanced Nutrition Less Than Body Requirements Related To Poor Dietary Intake As Evidenced by Weight Less Than NormalDocument2 pagesNCP - Imbalanced Nutrition Less Than Body Requirements Related To Poor Dietary Intake As Evidenced by Weight Less Than NormalMeroy Cleofe67% (9)
- Nutrition Care Plan: Assessment Diagnosis Intervention Rationale Monitoring EvaluateDocument1 pageNutrition Care Plan: Assessment Diagnosis Intervention Rationale Monitoring EvaluateLarr SumalpongNo ratings yet
- NCP Imbalanced Nutrition Less Than Body Requirements DIARRHEADocument2 pagesNCP Imbalanced Nutrition Less Than Body Requirements DIARRHEAMa. Elaine Carla TatingNo ratings yet
- MNT in Critically Ill - Lora2015Document11 pagesMNT in Critically Ill - Lora2015pusatdatagizi soewondokendalNo ratings yet
- Ncp-Potential-Fernandez Hashhash Navarro PaitDocument3 pagesNcp-Potential-Fernandez Hashhash Navarro PaitBasema HashhashNo ratings yet
- Basis Nutrition and Nutritional TherapyDocument9 pagesBasis Nutrition and Nutritional TherapyPrincess CaidoNo ratings yet
- NCP EatingDocument1 pageNCP Eatingsnow.parconNo ratings yet
- Nursing Care Plan - CancerDocument3 pagesNursing Care Plan - CancerChristineAla0% (1)
- Y2 S2 MT NCM 109 RLE - Reporting Draft - Feeding Helpless PatientsDocument39 pagesY2 S2 MT NCM 109 RLE - Reporting Draft - Feeding Helpless PatientsAlyssa Claire TumulakNo ratings yet
- NCP of Patient With GastritisDocument4 pagesNCP of Patient With GastritisBer AnneNo ratings yet
- TPN, CVP, Mech Vent, Dialysis SKILLS LABDocument14 pagesTPN, CVP, Mech Vent, Dialysis SKILLS LABmelba040510No ratings yet
- Finalize Nursing CareplanDocument20 pagesFinalize Nursing Careplanglaizarosario8No ratings yet
- NCP Lec 3Document5 pagesNCP Lec 3goya kitkatNo ratings yet
- Critical Ill PDFDocument5 pagesCritical Ill PDFAnish H DaveNo ratings yet
- RTD Vital 1,5 KkalDocument36 pagesRTD Vital 1,5 KkalLuther ThengNo ratings yet
- NCP in POC Module (Bernales)Document11 pagesNCP in POC Module (Bernales)Jan Lianne BernalesNo ratings yet
- Nutritional Support NotesDocument14 pagesNutritional Support NotesAudrie Allyson Gabales100% (1)
- Potential: Assessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationDocument3 pagesPotential: Assessment Explanation of The Problem Objectives Nursing Interventions Rationale EvaluationBasema HashhashNo ratings yet
- NCP GDMDocument1 pageNCP GDMboom100% (1)
- Nursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationDocument3 pagesNursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationMarivic Yuson MalagarNo ratings yet
- 2B - 5 - Chindy Anzellica - Review QuizDocument6 pages2B - 5 - Chindy Anzellica - Review QuizCece ArcylaNo ratings yet
- Gastrointestinal and MetabolismDocument5 pagesGastrointestinal and MetabolismDan HizonNo ratings yet
- Improved NutritionDocument2 pagesImproved NutritionDaintyGarciaNo ratings yet
- Surg - Surgical Nutrition X DokkaebiDocument8 pagesSurg - Surgical Nutrition X DokkaebivictorazucenaNo ratings yet
- Bradycardia and HypothermiaDocument3 pagesBradycardia and HypothermiaWILMARIE SAPANTANo ratings yet
- Ackerman SupportiveFeedingMethods TVNWinter2020Document6 pagesAckerman SupportiveFeedingMethods TVNWinter2020FinishNo ratings yet
- 88 FinalDocument4 pages88 FinalEshiebel OrganistaNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care PlanJasha MaeNo ratings yet
- Risk For Imbalanced NutritionDocument3 pagesRisk For Imbalanced Nutritionaudreyann.acobNo ratings yet
- Nursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term GoalDocument2 pagesNursing Care Plan Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective Data: Short Term GoalRhos Antonette GuimbanNo ratings yet
- Introduction To NutritionDocument19 pagesIntroduction To Nutritionseanne kskwkwkaNo ratings yet
- Imbalanced Nutrition Less Than Body Requirements Diabetes NCP PDFDocument5 pagesImbalanced Nutrition Less Than Body Requirements Diabetes NCP PDFashamy acolNo ratings yet
- NCP GDMDocument2 pagesNCP GDMboomNo ratings yet
- Basic Nutrition and Doctor Prescribed Diets-Resource GuideDocument120 pagesBasic Nutrition and Doctor Prescribed Diets-Resource GuideArun100% (1)
- NCP Uterine ProlapsedDocument4 pagesNCP Uterine ProlapsedPrincessYnaRonquillo100% (1)
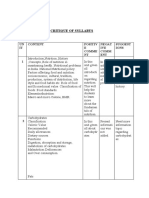
- Critique of Syllabus: UN IT Content Positiv E Comme NT Negat IVE Comm ENT Suggest IonsDocument6 pagesCritique of Syllabus: UN IT Content Positiv E Comme NT Negat IVE Comm ENT Suggest Ionsmerin sunilNo ratings yet
- Critique of Syllabus: UN IT Content Positiv E Comme NT Negat IVE Comm ENT Suggest IonsDocument6 pagesCritique of Syllabus: UN IT Content Positiv E Comme NT Negat IVE Comm ENT Suggest Ionsmerin sunilNo ratings yet
- Imbalanced Nutrition Less Than Body RequirementsDocument2 pagesImbalanced Nutrition Less Than Body RequirementsFrudz Orjaleza100% (1)
- Anorexia. Fisiología y ExperimentoDocument2 pagesAnorexia. Fisiología y Experimentoliz solanoNo ratings yet
- Gi Case StudyDocument3 pagesGi Case Studyapi-622273373No ratings yet
- Nutrition InterventionDocument12 pagesNutrition Interventionsham ibrahimNo ratings yet
- Nutrition: A Handbook for NursesFrom EverandNutrition: A Handbook for NursesCarolyn BestNo ratings yet
- Approval SheetDocument1 pageApproval SheetJim RashidNo ratings yet
- Progress NotesDocument7 pagesProgress NotesJim RashidNo ratings yet
- Complete Blood Count: Table 6. Laboratory and ProceduresDocument2 pagesComplete Blood Count: Table 6. Laboratory and ProceduresJim RashidNo ratings yet
- Implementation Phase: Table 19. Nursing Care ImplementationDocument5 pagesImplementation Phase: Table 19. Nursing Care ImplementationJim RashidNo ratings yet
- Summary, Conclusion, and RecommendationDocument3 pagesSummary, Conclusion, and RecommendationJim RashidNo ratings yet
- Henderson's 14 ComponentsDocument6 pagesHenderson's 14 ComponentsJim RashidNo ratings yet
- A. Physical (Dillon'S Physical Assessment Tool)Document7 pagesA. Physical (Dillon'S Physical Assessment Tool)Jim RashidNo ratings yet
- Problem Identification and PrioritizationDocument4 pagesProblem Identification and PrioritizationJim RashidNo ratings yet
- Appendix B Health TeachingDocument5 pagesAppendix B Health TeachingJim RashidNo ratings yet
- MedsDocument6 pagesMedsJim RashidNo ratings yet
- Bibliography 1. BooksDocument4 pagesBibliography 1. BooksJim RashidNo ratings yet
- He Tone Ews: Feeling Crowded? Thank God!Document8 pagesHe Tone Ews: Feeling Crowded? Thank God!Stone Church of Willow GlenNo ratings yet
- 2024 Elementary School SyllabusDocument37 pages2024 Elementary School SyllabusgiselafariniaprofNo ratings yet
- Wanna Bet R S BurnettDocument197 pagesWanna Bet R S BurnettCatalina Jipa100% (1)
- Task 4.: Let'S TalkDocument7 pagesTask 4.: Let'S TalkGabriel GuioNo ratings yet
- Commercial Refrigeration Equipment Research OpportunitiesDocument221 pagesCommercial Refrigeration Equipment Research Opportunitiesandrei1108No ratings yet
- Important TIPS When Composing Your ResumeDocument4 pagesImportant TIPS When Composing Your ResumeMohidin Kumayog MaslamamaNo ratings yet
- Tle BPP10 Q2 M6Document8 pagesTle BPP10 Q2 M6Genevie SisonNo ratings yet
- Group 1A - Alkali Metals Elements Compounds Pharmaceutical Uses Chemical Name Chemical FormulaDocument2 pagesGroup 1A - Alkali Metals Elements Compounds Pharmaceutical Uses Chemical Name Chemical FormulaCharlyn Keith100% (1)
- Formulation and Evaluation of Herbal Lip Rouge.: Research ArticleDocument5 pagesFormulation and Evaluation of Herbal Lip Rouge.: Research ArticleTynNo ratings yet
- 115 D2CDocument8 pages115 D2CkshitijgoyalNo ratings yet
- Conversation Questions PDFDocument2 pagesConversation Questions PDFاسامه محمدNo ratings yet
- Company Profile PizzavilleDocument7 pagesCompany Profile PizzavilleSatrioSaktiUtomoNo ratings yet
- Ankush English SolutionsDocument107 pagesAnkush English SolutionsAbhilasha ChopraNo ratings yet
- DIY Spirulina Superfood Food of The Future WindowDocument11 pagesDIY Spirulina Superfood Food of The Future WindowtononoinkNo ratings yet
- Eight Little LeprechaunsDocument3 pagesEight Little LeprechaunsVic RabayaNo ratings yet
- BAC GIANG - Đề thi chọn ĐT 2023 (chính thức)Document19 pagesBAC GIANG - Đề thi chọn ĐT 2023 (chính thức)Le Thi Lan Huong Truong THPT chuyen Hoang Le KhaNo ratings yet
- Presentation On Pizza Hut.Document14 pagesPresentation On Pizza Hut.patidarsunilNo ratings yet
- Food and Health Unit 1Document59 pagesFood and Health Unit 1Tsz Yan LeungNo ratings yet
- 2023학년도 7월 고3 전국연합학력평가 3교시 영어영역Document4 pages2023학년도 7월 고3 전국연합학력평가 3교시 영어영역Bee JamesNo ratings yet
- Breaking Chains of Poverty PDFDocument31 pagesBreaking Chains of Poverty PDFKiiza Wa'UgunguNo ratings yet
- Utilization of Some Food Processing Wastes As A Fat Replacers in CakesDocument12 pagesUtilization of Some Food Processing Wastes As A Fat Replacers in CakesBanuraspatiNo ratings yet
- British MealsDocument2 pagesBritish MealsStrafalogea Serban100% (1)
- Breakfast Feeding PresentationDocument64 pagesBreakfast Feeding PresentationHoneylet Ü FerolNo ratings yet
- ISE III Practice ExamDocument9 pagesISE III Practice ExamesthermuelaNo ratings yet
- Travel Guide Hyderabad Mumbai Bengaluru and DelhiDocument80 pagesTravel Guide Hyderabad Mumbai Bengaluru and DelhiVikram BaggaNo ratings yet
- Improved Cookstoves As A Pathway Between Food Preparation and Reduced Domestic Violence in UgandaDocument9 pagesImproved Cookstoves As A Pathway Between Food Preparation and Reduced Domestic Violence in UgandagernNo ratings yet
- Mamcn Poster LastDocument1 pageMamcn Poster LastmichelNo ratings yet
- HLF NewspaperDocument8 pagesHLF Newspaperlgrecu77No ratings yet