
Cohen 2020
Cohen 2020
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Ricardo v. Lloyd, Robert Y. Osamura, Gunter Kloppel, Juan Rosai - WHO Classification of Tumours of Endocrine Organs-IARC (2019)Document283 pagesRicardo v. Lloyd, Robert Y. Osamura, Gunter Kloppel, Juan Rosai - WHO Classification of Tumours of Endocrine Organs-IARC (2019)leartaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Functional Assessment For Challenging Behaviors 2012Document244 pagesFunctional Assessment For Challenging Behaviors 2012khadidja BOUTOUILNo ratings yet
- Borge Fagerli - 10 Good Habits For Better ResultsDocument12 pagesBorge Fagerli - 10 Good Habits For Better ResultscoctyusNo ratings yet
- Standardized Curriculum in General Surgery 2012Document102 pagesStandardized Curriculum in General Surgery 2012Martin EscasuraNo ratings yet
- Poster ProceedingsDocument804 pagesPoster Proceedingskhadidja BOUTOUILNo ratings yet
- التقنيات التجريبية والعمل بهاDocument9 pagesالتقنيات التجريبية والعمل بهاkhadidja BOUTOUILNo ratings yet
- nimbalkar2018-التواصل غير اللفظي عند الرضع حديثي الولادة في العناية المركزة-مقالDocument3 pagesnimbalkar2018-التواصل غير اللفظي عند الرضع حديثي الولادة في العناية المركزة-مقالkhadidja BOUTOUILNo ratings yet
- Ars Lan 2019Document3 pagesArs Lan 2019khadidja BOUTOUILNo ratings yet
- Stone 2019Document11 pagesStone 2019khadidja BOUTOUILNo ratings yet
- Ody Nop HagiaDocument2 pagesOdy Nop Hagiakhadidja BOUTOUILNo ratings yet
- Shah 2019Document2 pagesShah 2019khadidja BOUTOUILNo ratings yet
- A Patient With Dysphagia: Case PresentationDocument3 pagesA Patient With Dysphagia: Case Presentationkhadidja BOUTOUILNo ratings yet
- Dysphagia in Parkinson's Disease Improves With Vocal AugmentationDocument7 pagesDysphagia in Parkinson's Disease Improves With Vocal Augmentationkhadidja BOUTOUILNo ratings yet
- Effects of Tongue Strengthening Exercise On The Geniohyoid Muscle in Young Healthy AdultsDocument7 pagesEffects of Tongue Strengthening Exercise On The Geniohyoid Muscle in Young Healthy Adultskhadidja BOUTOUILNo ratings yet
- Changes in The Excitability of Corticobulbar Projections Due To Intraoral Cooling With IceDocument5 pagesChanges in The Excitability of Corticobulbar Projections Due To Intraoral Cooling With Icekhadidja BOUTOUILNo ratings yet
- Posterior Tongue Tie, Base of Tongue Movement, and Pharyngeal Dysphagia: What Is The Connection?Document4 pagesPosterior Tongue Tie, Base of Tongue Movement, and Pharyngeal Dysphagia: What Is The Connection?khadidja BOUTOUILNo ratings yet
- An Evaluation of Chewing and Swallowing For A Child Diagnosed With AutismDocument12 pagesAn Evaluation of Chewing and Swallowing For A Child Diagnosed With Autismkhadidja BOUTOUILNo ratings yet
- Pharyngeal Area Changes in Parkinson's Disease and Its Effect On Swallowing Safety, Efficiency, and KinematicsDocument10 pagesPharyngeal Area Changes in Parkinson's Disease and Its Effect On Swallowing Safety, Efficiency, and Kinematicskhadidja BOUTOUILNo ratings yet
- Respiratory Swallow Pattern Following Total LaryngectomyDocument7 pagesRespiratory Swallow Pattern Following Total Laryngectomykhadidja BOUTOUILNo ratings yet
- Whiplash Associated Dysphagia and Dysphonia: A Scoping ReviewDocument13 pagesWhiplash Associated Dysphagia and Dysphonia: A Scoping Reviewkhadidja BOUTOUILNo ratings yet
- Interventions For Feeding and Swallowing Disorders in Adults With Intellectual Disability: A Systematic Review of The EvidenceDocument13 pagesInterventions For Feeding and Swallowing Disorders in Adults With Intellectual Disability: A Systematic Review of The Evidencekhadidja BOUTOUILNo ratings yet
- Pilot Study of Quantitative Methods For Differentiating Pharyngeal Swallowing Mechanics by Dysphagia EtiologyDocument11 pagesPilot Study of Quantitative Methods For Differentiating Pharyngeal Swallowing Mechanics by Dysphagia Etiologykhadidja BOUTOUILNo ratings yet
- Neuropsychology of CommunicationDocument13 pagesNeuropsychology of Communicationkhadidja BOUTOUILNo ratings yet
- Sa Jun 2018 PDFDocument6 pagesSa Jun 2018 PDFdpcamposhNo ratings yet
- Miko SisDocument90 pagesMiko SisFahlevi QalbiNo ratings yet
- Imaging Criteria For Assessing Tumour Response: Recist, Mrecist, ChesonDocument15 pagesImaging Criteria For Assessing Tumour Response: Recist, Mrecist, ChesonSitha MahendrataNo ratings yet
- Molecular Aspects of MedicineDocument20 pagesMolecular Aspects of MedicineLorena RamosNo ratings yet
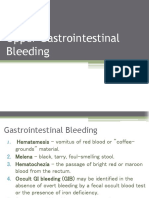
- Upper Gastrointestinal BleedingDocument7 pagesUpper Gastrointestinal BleedingironNo ratings yet
- The Borax Conspiracy How The Arthritis Cure Has Been Stopped - Walter LastDocument11 pagesThe Borax Conspiracy How The Arthritis Cure Has Been Stopped - Walter LastDazNo ratings yet
- Mechanical Plaque ControlDocument58 pagesMechanical Plaque ControlNeelam Khalia100% (1)
- Burkholderia CepaciaDocument3 pagesBurkholderia Cepaciavecerzan_lilianaNo ratings yet
- PCS Questions-6 PDFDocument10 pagesPCS Questions-6 PDFAzra MuzafarNo ratings yet
- V80832 MSDS Petro Canada DuronE Engine Oil SAE 15W-40Document5 pagesV80832 MSDS Petro Canada DuronE Engine Oil SAE 15W-40PaulPaucarCamposNo ratings yet
- Cancers 15 04479Document14 pagesCancers 15 04479Anu ShaNo ratings yet
- Aaa PDFDocument26 pagesAaa PDFnonika sianturiNo ratings yet
- Signs and Symptoms of Respiratory DiseasesDocument42 pagesSigns and Symptoms of Respiratory DiseasesjabeedNo ratings yet
- Seborrheic DermatitisDocument34 pagesSeborrheic DermatitisRizky Takdir RamadhanNo ratings yet
- Trimethoprim Sulfamethoxazole (TMP SMZ) Co TrimoxazoleDocument1 pageTrimethoprim Sulfamethoxazole (TMP SMZ) Co TrimoxazoleRenmico Aquino0% (1)
- IPS Empress System - Dental LabsDocument159 pagesIPS Empress System - Dental LabsAlex BurdeNo ratings yet
- Olanzapina Antiemesis 2018Document5 pagesOlanzapina Antiemesis 2018Dra. Rossmery Espinosa MendozaNo ratings yet
- Med and Surg RecallDocument15 pagesMed and Surg RecallSherif ElbadrawyNo ratings yet
- Otorhino Dr. R. RegaladoDocument4 pagesOtorhino Dr. R. RegaladoDoctor CastleNo ratings yet
- Management of Ruptured Liver Abscess: A Study of 54 CasesDocument4 pagesManagement of Ruptured Liver Abscess: A Study of 54 CasesIndah FebrianaNo ratings yet
- Asthma or Copd Case StudyDocument10 pagesAsthma or Copd Case StudyMahendra ShrimaliNo ratings yet
- Asbestos: From Wikipedia, The Free Encyclopedia Jump To:, For Other Uses, SeeDocument26 pagesAsbestos: From Wikipedia, The Free Encyclopedia Jump To:, For Other Uses, SeeSonorizari BrasovNo ratings yet
- Chronic Pancreatitis: PathophysiologyDocument7 pagesChronic Pancreatitis: PathophysiologyMadelaine De Arco J.No ratings yet
- ST NoDocument89 pagesST NoShaz Chindhy100% (1)
- Stem Cell Cryobank: Cord Blood and Stem Cells For LifeDocument23 pagesStem Cell Cryobank: Cord Blood and Stem Cells For LifelyndonlinNo ratings yet
- 1.TUM Benigne UterinaDocument47 pages1.TUM Benigne UterinaPavel BerlinschiNo ratings yet
- Surgical Techniques For Prostate Cancer, 1E (2015)Document137 pagesSurgical Techniques For Prostate Cancer, 1E (2015)DiahaNo ratings yet























































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5824)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Ricardo v. Lloyd, Robert Y. Osamura, Gunter Kloppel, Juan Rosai - WHO Classification of Tumours of Endocrine Organs-IARC (2019)Document283 pagesRicardo v. Lloyd, Robert Y. Osamura, Gunter Kloppel, Juan Rosai - WHO Classification of Tumours of Endocrine Organs-IARC (2019)leartaNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Functional Assessment For Challenging Behaviors 2012Document244 pagesFunctional Assessment For Challenging Behaviors 2012khadidja BOUTOUILNo ratings yet
- Borge Fagerli - 10 Good Habits For Better ResultsDocument12 pagesBorge Fagerli - 10 Good Habits For Better ResultscoctyusNo ratings yet
- Standardized Curriculum in General Surgery 2012Document102 pagesStandardized Curriculum in General Surgery 2012Martin EscasuraNo ratings yet
- Poster ProceedingsDocument804 pagesPoster Proceedingskhadidja BOUTOUILNo ratings yet
- التقنيات التجريبية والعمل بهاDocument9 pagesالتقنيات التجريبية والعمل بهاkhadidja BOUTOUILNo ratings yet
- nimbalkar2018-التواصل غير اللفظي عند الرضع حديثي الولادة في العناية المركزة-مقالDocument3 pagesnimbalkar2018-التواصل غير اللفظي عند الرضع حديثي الولادة في العناية المركزة-مقالkhadidja BOUTOUILNo ratings yet
- Ars Lan 2019Document3 pagesArs Lan 2019khadidja BOUTOUILNo ratings yet
- Stone 2019Document11 pagesStone 2019khadidja BOUTOUILNo ratings yet
- Ody Nop HagiaDocument2 pagesOdy Nop Hagiakhadidja BOUTOUILNo ratings yet
- Shah 2019Document2 pagesShah 2019khadidja BOUTOUILNo ratings yet
- A Patient With Dysphagia: Case PresentationDocument3 pagesA Patient With Dysphagia: Case Presentationkhadidja BOUTOUILNo ratings yet
- Dysphagia in Parkinson's Disease Improves With Vocal AugmentationDocument7 pagesDysphagia in Parkinson's Disease Improves With Vocal Augmentationkhadidja BOUTOUILNo ratings yet
- Effects of Tongue Strengthening Exercise On The Geniohyoid Muscle in Young Healthy AdultsDocument7 pagesEffects of Tongue Strengthening Exercise On The Geniohyoid Muscle in Young Healthy Adultskhadidja BOUTOUILNo ratings yet
- Changes in The Excitability of Corticobulbar Projections Due To Intraoral Cooling With IceDocument5 pagesChanges in The Excitability of Corticobulbar Projections Due To Intraoral Cooling With Icekhadidja BOUTOUILNo ratings yet
- Posterior Tongue Tie, Base of Tongue Movement, and Pharyngeal Dysphagia: What Is The Connection?Document4 pagesPosterior Tongue Tie, Base of Tongue Movement, and Pharyngeal Dysphagia: What Is The Connection?khadidja BOUTOUILNo ratings yet
- An Evaluation of Chewing and Swallowing For A Child Diagnosed With AutismDocument12 pagesAn Evaluation of Chewing and Swallowing For A Child Diagnosed With Autismkhadidja BOUTOUILNo ratings yet
- Pharyngeal Area Changes in Parkinson's Disease and Its Effect On Swallowing Safety, Efficiency, and KinematicsDocument10 pagesPharyngeal Area Changes in Parkinson's Disease and Its Effect On Swallowing Safety, Efficiency, and Kinematicskhadidja BOUTOUILNo ratings yet
- Respiratory Swallow Pattern Following Total LaryngectomyDocument7 pagesRespiratory Swallow Pattern Following Total Laryngectomykhadidja BOUTOUILNo ratings yet
- Whiplash Associated Dysphagia and Dysphonia: A Scoping ReviewDocument13 pagesWhiplash Associated Dysphagia and Dysphonia: A Scoping Reviewkhadidja BOUTOUILNo ratings yet
- Interventions For Feeding and Swallowing Disorders in Adults With Intellectual Disability: A Systematic Review of The EvidenceDocument13 pagesInterventions For Feeding and Swallowing Disorders in Adults With Intellectual Disability: A Systematic Review of The Evidencekhadidja BOUTOUILNo ratings yet
- Pilot Study of Quantitative Methods For Differentiating Pharyngeal Swallowing Mechanics by Dysphagia EtiologyDocument11 pagesPilot Study of Quantitative Methods For Differentiating Pharyngeal Swallowing Mechanics by Dysphagia Etiologykhadidja BOUTOUILNo ratings yet
- Neuropsychology of CommunicationDocument13 pagesNeuropsychology of Communicationkhadidja BOUTOUILNo ratings yet
- Sa Jun 2018 PDFDocument6 pagesSa Jun 2018 PDFdpcamposhNo ratings yet
- Miko SisDocument90 pagesMiko SisFahlevi QalbiNo ratings yet
- Imaging Criteria For Assessing Tumour Response: Recist, Mrecist, ChesonDocument15 pagesImaging Criteria For Assessing Tumour Response: Recist, Mrecist, ChesonSitha MahendrataNo ratings yet
- Molecular Aspects of MedicineDocument20 pagesMolecular Aspects of MedicineLorena RamosNo ratings yet
- Upper Gastrointestinal BleedingDocument7 pagesUpper Gastrointestinal BleedingironNo ratings yet
- The Borax Conspiracy How The Arthritis Cure Has Been Stopped - Walter LastDocument11 pagesThe Borax Conspiracy How The Arthritis Cure Has Been Stopped - Walter LastDazNo ratings yet
- Mechanical Plaque ControlDocument58 pagesMechanical Plaque ControlNeelam Khalia100% (1)
- Burkholderia CepaciaDocument3 pagesBurkholderia Cepaciavecerzan_lilianaNo ratings yet
- PCS Questions-6 PDFDocument10 pagesPCS Questions-6 PDFAzra MuzafarNo ratings yet
- V80832 MSDS Petro Canada DuronE Engine Oil SAE 15W-40Document5 pagesV80832 MSDS Petro Canada DuronE Engine Oil SAE 15W-40PaulPaucarCamposNo ratings yet
- Cancers 15 04479Document14 pagesCancers 15 04479Anu ShaNo ratings yet
- Aaa PDFDocument26 pagesAaa PDFnonika sianturiNo ratings yet
- Signs and Symptoms of Respiratory DiseasesDocument42 pagesSigns and Symptoms of Respiratory DiseasesjabeedNo ratings yet
- Seborrheic DermatitisDocument34 pagesSeborrheic DermatitisRizky Takdir RamadhanNo ratings yet
- Trimethoprim Sulfamethoxazole (TMP SMZ) Co TrimoxazoleDocument1 pageTrimethoprim Sulfamethoxazole (TMP SMZ) Co TrimoxazoleRenmico Aquino0% (1)
- IPS Empress System - Dental LabsDocument159 pagesIPS Empress System - Dental LabsAlex BurdeNo ratings yet
- Olanzapina Antiemesis 2018Document5 pagesOlanzapina Antiemesis 2018Dra. Rossmery Espinosa MendozaNo ratings yet
- Med and Surg RecallDocument15 pagesMed and Surg RecallSherif ElbadrawyNo ratings yet
- Otorhino Dr. R. RegaladoDocument4 pagesOtorhino Dr. R. RegaladoDoctor CastleNo ratings yet
- Management of Ruptured Liver Abscess: A Study of 54 CasesDocument4 pagesManagement of Ruptured Liver Abscess: A Study of 54 CasesIndah FebrianaNo ratings yet
- Asthma or Copd Case StudyDocument10 pagesAsthma or Copd Case StudyMahendra ShrimaliNo ratings yet
- Asbestos: From Wikipedia, The Free Encyclopedia Jump To:, For Other Uses, SeeDocument26 pagesAsbestos: From Wikipedia, The Free Encyclopedia Jump To:, For Other Uses, SeeSonorizari BrasovNo ratings yet
- Chronic Pancreatitis: PathophysiologyDocument7 pagesChronic Pancreatitis: PathophysiologyMadelaine De Arco J.No ratings yet
- ST NoDocument89 pagesST NoShaz Chindhy100% (1)
- Stem Cell Cryobank: Cord Blood and Stem Cells For LifeDocument23 pagesStem Cell Cryobank: Cord Blood and Stem Cells For LifelyndonlinNo ratings yet
- 1.TUM Benigne UterinaDocument47 pages1.TUM Benigne UterinaPavel BerlinschiNo ratings yet
- Surgical Techniques For Prostate Cancer, 1E (2015)Document137 pagesSurgical Techniques For Prostate Cancer, 1E (2015)DiahaNo ratings yet