Download as docx, pdf, or txt
You might also like
- Full Chapter Case Studies On Diversity and Social Justice Education 3Rd Edition Paul C Gorski PDFDocument53 pagesFull Chapter Case Studies On Diversity and Social Justice Education 3Rd Edition Paul C Gorski PDFjosephine.chandler412100% (4)
- Evaluation Tool For Localized LRDocument2 pagesEvaluation Tool For Localized LRXYLEANE ALFORTE96% (54)
- ISEE Lower Level Exam Prep 2020-2021: ISEE Study Guide with 512 Test Questions and Answer Explanations (4 Full Practice Tests)From EverandISEE Lower Level Exam Prep 2020-2021: ISEE Study Guide with 512 Test Questions and Answer Explanations (4 Full Practice Tests)No ratings yet
- Diagnostic Test Report Form - 2019Document5 pagesDiagnostic Test Report Form - 2019Karima RihaniNo ratings yet
- BPP Credibiltiy Interview - Updated... HAROONDocument7 pagesBPP Credibiltiy Interview - Updated... HAROONfahimNo ratings yet
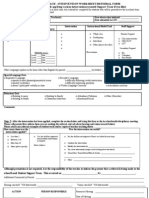
- IEP Draft Form StevenAndrewsDocument5 pagesIEP Draft Form StevenAndrewsAshley ThomasNo ratings yet
- General Assessment Form: (For PR, Visitor Visa and Work Permit)Document2 pagesGeneral Assessment Form: (For PR, Visitor Visa and Work Permit)Arshpreet KaurNo ratings yet
- Academic Tiered Interventions ListsDocument1 pageAcademic Tiered Interventions Listsapi-249399814No ratings yet
- Sample IepDocument10 pagesSample Iepapi-277472970100% (3)
- Informal Speech and Language Assessment GuideDocument13 pagesInformal Speech and Language Assessment GuideGiannina Nicole Cepeda CastilloNo ratings yet
- SBT Referral FormDocument2 pagesSBT Referral FormStephanie WongNo ratings yet
- IRCS-NSP PV FormDocument7 pagesIRCS-NSP PV FormkingofkasurNo ratings yet
- Pre Referral Intervention StrategiesDocument2 pagesPre Referral Intervention StrategiesStephanie Wong100% (1)
- Speech-Generating Device EvaluationDocument4 pagesSpeech-Generating Device EvaluationlabavillaNo ratings yet
- Assessment Workshop For Parents Sept '23Document28 pagesAssessment Workshop For Parents Sept '23Fatima LakisNo ratings yet
- Saludes - IEP Format 1Document7 pagesSaludes - IEP Format 1Angela ApolonioNo ratings yet
- Monitoring and Evaluation Tools To Sci Activity With FamilyDocument5 pagesMonitoring and Evaluation Tools To Sci Activity With FamilySuzette VillonNo ratings yet
- Authentic Assessment ToolsDocument10 pagesAuthentic Assessment ToolsMary Christine IgnacioNo ratings yet
- El Aio MtssDocument18 pagesEl Aio Mtssapi-2966931000% (1)
- Vacancy App FormDocument5 pagesVacancy App FormKV RAIWALANo ratings yet
- Level:: Test Aspect / Section Covered Date: Observations / CommentsDocument5 pagesLevel:: Test Aspect / Section Covered Date: Observations / CommentsRodrigo Leao100% (1)
- Azenith Ilag - Personalized Learning Plan Template For Gifted and Talented LearnerDocument5 pagesAzenith Ilag - Personalized Learning Plan Template For Gifted and Talented LearnerAzenith Talamor IlagNo ratings yet
- Questionnaire Speech TherapyDocument4 pagesQuestionnaire Speech Therapyshabbir hussainNo ratings yet
- Resource Packet Assessment of Developmental DelayDocument37 pagesResource Packet Assessment of Developmental DelayXlian Myzter YosaNo ratings yet
- 26 Observation ToolsDocument11 pages26 Observation ToolsNATIPER BAÑADOSNo ratings yet
- Tiered Approach Referral SheetDocument3 pagesTiered Approach Referral SheetUruz86100% (1)
- Individualized Education PlanDocument9 pagesIndividualized Education PlanimeldaNo ratings yet
- LR ToolDocument3 pagesLR ToolJohn Christian Basas100% (1)
- TOS (Format)Document1 pageTOS (Format)Charlotte GallegoNo ratings yet
- Episode 8 FS1Document12 pagesEpisode 8 FS1Nole Jr. Tanjay Oczon100% (1)
- Lecture 07 SelectionDocument26 pagesLecture 07 SelectionRAVI SHARMA-DM 21DM163No ratings yet
- Rita GDocument10 pagesRita Gapi-458486566No ratings yet
- School Discipline FormDocument2 pagesSchool Discipline FormRHANDY EVANGELISTANo ratings yet
- Appendix B: WCE Application Form - Template - Rev. 10112017Document1 pageAppendix B: WCE Application Form - Template - Rev. 10112017PWU Graduate Studies100% (1)
- Individualized Education Plan (Iep)Document8 pagesIndividualized Education Plan (Iep)Sarah Lombres Antigua Montefalco100% (1)
- Sample Neuropsychological ReportDocument23 pagesSample Neuropsychological ReporttanishasvNo ratings yet
- Validation Sheet For Questionnaire: Scale: 5-Very High 4-High 3-Moderate 2-Poor 1-Very PoorDocument2 pagesValidation Sheet For Questionnaire: Scale: 5-Very High 4-High 3-Moderate 2-Poor 1-Very PoorAndre Deyniel CabreraNo ratings yet
- SefweDocument10 pagesSefweapi-699389850No ratings yet
- Teacher Data Analysis Form Student Spreadsheet: Class: - SubjectDocument9 pagesTeacher Data Analysis Form Student Spreadsheet: Class: - Subjectapi-327228379No ratings yet
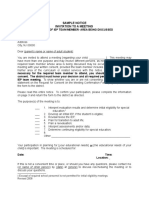
- Sample Notice Invitation To A Meeting: Child) Is Important. The Meeting Is Scheduled ForDocument4 pagesSample Notice Invitation To A Meeting: Child) Is Important. The Meeting Is Scheduled ForMarife CulabaNo ratings yet
- Teacher School ME Report S.Y. 2019 2020Document6 pagesTeacher School ME Report S.Y. 2019 2020Rufus TanhuecoNo ratings yet
- Teacher School ME Report S.Y. 2019 2020Document6 pagesTeacher School ME Report S.Y. 2019 2020Josie LebrinoNo ratings yet
- CHCLEG001 STUDENT WORKBOOK (WORD) (C3) .v1.1Document44 pagesCHCLEG001 STUDENT WORKBOOK (WORD) (C3) .v1.1shrestha31dristiNo ratings yet
- IEN Registration Form 2022Document1 pageIEN Registration Form 2022drummernico25No ratings yet
- SURVEY QUESTIONS FMA 2022 - Katryn AnisDocument7 pagesSURVEY QUESTIONS FMA 2022 - Katryn AnisRhica Macasaya MendozaNo ratings yet
- TeacherDocument6 pagesTeacherElaine RyanaNo ratings yet
- Needs Analysis Naxi Jgs Conversation Topics Dialogs - 139242Document2 pagesNeeds Analysis Naxi Jgs Conversation Topics Dialogs - 139242Nouraiz AwanNo ratings yet
- FT SDW 098 00 Career Planning FormDocument1 pageFT SDW 098 00 Career Planning FormNasi RiceNo ratings yet
- Kuesioner Learning DifficultiesDocument6 pagesKuesioner Learning Difficultieseva pandanaNo ratings yet
- 4-5 Writing Data ToolDocument5 pages4-5 Writing Data Toolapi-405348458No ratings yet
- Internal Control Questionnaire: Prepared By: - Date: - Reviewed By: - DateDocument5 pagesInternal Control Questionnaire: Prepared By: - Date: - Reviewed By: - DateChooji HachiiNo ratings yet
- CHCDIS007 STUDENT WORKBOOK (WORD) (C3) .v1.1Document60 pagesCHCDIS007 STUDENT WORKBOOK (WORD) (C3) .v1.1Elsa Miriam Binoy100% (4)
- School Profile TemplateDocument2 pagesSchool Profile TemplateIFTIIN SCHOOLSNo ratings yet
- GRADE 7 ENGLISH ACTIVITY SHEETQuarter 1 Module2 PDFDocument7 pagesGRADE 7 ENGLISH ACTIVITY SHEETQuarter 1 Module2 PDFMike Rowen BanaresNo ratings yet
- Verification-Adhd-Psych-2020 (1) - 211108 - 095107Document3 pagesVerification-Adhd-Psych-2020 (1) - 211108 - 095107Stephan ChiariniNo ratings yet
- M2 FinalDocument61 pagesM2 FinalJeranz ColansiNo ratings yet
- Checklist 2023Document2 pagesChecklist 2023f20230222No ratings yet
- Next Steps: Will Master Reading and Math Learning Targets: ALL 3-5 StudentsDocument83 pagesNext Steps: Will Master Reading and Math Learning Targets: ALL 3-5 StudentsetoweeNo ratings yet
- Benchmark Data Worksheet: Analysis To ActionDocument1 pageBenchmark Data Worksheet: Analysis To Actionapi-361935578No ratings yet
- TA LRP ImplementationDocument25 pagesTA LRP Implementationreniag. banezNo ratings yet
- PSAT/NMSQT Premium Study Guide: 2025: 2 Practice Tests + Comprehensive Review + 200 Online DrillsFrom EverandPSAT/NMSQT Premium Study Guide: 2025: 2 Practice Tests + Comprehensive Review + 200 Online DrillsRating: 5 out of 5 stars5/5 (1)
- Practice Makes Perfect: Advanced English Grammar for ESL Learners, Second EditionFrom EverandPractice Makes Perfect: Advanced English Grammar for ESL Learners, Second EditionRating: 5 out of 5 stars5/5 (1)
- 530 BenchmarkDocument6 pages530 Benchmarkapi-550921670No ratings yet
- Impatient Parents: Case Analysis SummaryDocument3 pagesImpatient Parents: Case Analysis Summaryapi-550921670No ratings yet
- Dress Code PolicyDocument3 pagesDress Code Policyapi-550921670No ratings yet
- Establishing A Continuous Professional Learning Culture 1Document1 pageEstablishing A Continuous Professional Learning Culture 1api-550921670No ratings yet
- Building Trust in A Diverse Community Case AnalysisDocument2 pagesBuilding Trust in A Diverse Community Case Analysisapi-550921670No ratings yet
- Reviving The Professional CultureDocument3 pagesReviving The Professional Cultureapi-550921670No ratings yet
- LCMT Form 2Document3 pagesLCMT Form 2api-550921670No ratings yet
- Ethics ProjectDocument3 pagesEthics Projectapi-550921670No ratings yet
- Out PDFDocument15 pagesOut PDFAnonymous XpakVbJYDSNo ratings yet
- Semester - I: R.T.M.Nagpur University, Nagpur Syllabus For Bachelor of Science Part - I Supplementary English CourseDocument4 pagesSemester - I: R.T.M.Nagpur University, Nagpur Syllabus For Bachelor of Science Part - I Supplementary English CourseAkash DNo ratings yet
- Sjastad, H., & Baumeister, R. F., (2023), Fast Optimism, Slow Realism. Causal Evidence For Two-Step Model of Future ThinkingDocument14 pagesSjastad, H., & Baumeister, R. F., (2023), Fast Optimism, Slow Realism. Causal Evidence For Two-Step Model of Future Thinking9 PsychologyNo ratings yet
- Pangasinan School of Arts and Trade (SUB PROFESSIONAL) PDFDocument19 pagesPangasinan School of Arts and Trade (SUB PROFESSIONAL) PDFPhilBoardResultsNo ratings yet
- ET Classroom Trainer Step Up Card: Education & Training PillarDocument2 pagesET Classroom Trainer Step Up Card: Education & Training PillarHamza Bin MasoodNo ratings yet
- Timed Up and Go - Diagnóstico de DemênciaDocument6 pagesTimed Up and Go - Diagnóstico de DemênciaMarta SilvaNo ratings yet
- Assignment 2Document10 pagesAssignment 2Joseph PerezNo ratings yet
- Venkataravikirand1 45L)Document3 pagesVenkataravikirand1 45L)nvvsganesh1984No ratings yet
- TWAS Research Grant FormDocument5 pagesTWAS Research Grant Formwaseemkhan49No ratings yet
- 'A' Level Tropical African HistoryDocument278 pages'A' Level Tropical African HistorymarimanziolynNo ratings yet
- DLP Cookery SAMPLEDocument9 pagesDLP Cookery SAMPLEMha Riz100% (4)
- Kane and Abel Case Study Answer KeyDocument3 pagesKane and Abel Case Study Answer KeyJordan SteeleNo ratings yet
- 12ft - Object Oriented Data Science - Refactoring Code - by Molly Ruby - Aug, 2023 - Towards Data ScienceDocument4 pages12ft - Object Oriented Data Science - Refactoring Code - by Molly Ruby - Aug, 2023 - Towards Data SciencePERLUESNo ratings yet
- Easy Guide To MeditationDocument49 pagesEasy Guide To Meditationapextrader_955187937100% (1)
- 1 Anagram MaimunahDocument13 pages1 Anagram MaimunahAnn NmayaNo ratings yet
- Chapter VDocument37 pagesChapter VKeir HeiNo ratings yet
- Business Management: TH THDocument2 pagesBusiness Management: TH THcosmo world0% (1)
- Business ProposalDocument11 pagesBusiness ProposalMelchorCandelariaNo ratings yet
- How To Do in Text and End Text CitationDocument24 pagesHow To Do in Text and End Text CitationLogeswaran Tangavello67% (3)
- 251 A Bar at The Folies - BergereDocument1 page251 A Bar at The Folies - BergereDavid FanNo ratings yet
- Jealousy and Problems of CommitmentDocument10 pagesJealousy and Problems of Commitmentricardo nNo ratings yet
- Illuminati ConstitutionDocument7 pagesIlluminati ConstitutionBoban TrpevskiNo ratings yet
- HRM 613 Handouts 1 45 PDFDocument99 pagesHRM 613 Handouts 1 45 PDFsaadNo ratings yet
- Course Hero Application KitDocument17 pagesCourse Hero Application KitRONALYN GONZALESNo ratings yet
- Detailed Lesson PlanDocument3 pagesDetailed Lesson PlanPhinelie Gardose CelinoNo ratings yet
- World English 3e Level Intro Grammar Activities Unit 6 Lesson CDocument1 pageWorld English 3e Level Intro Grammar Activities Unit 6 Lesson CFernanda Santos FreitasNo ratings yet
- 2.module - PR 2 (Day 3 & 4 of Week 6) - Defining TermsDocument29 pages2.module - PR 2 (Day 3 & 4 of Week 6) - Defining TermsKevz Becerro Espiel100% (1)
- Iwip-C NDTDocument4 pagesIwip-C NDTชุมพล พลตรีNo ratings yet