Professional Documents
Culture Documents
Classification of Common Acetabular Fractures: Radiographic and CT Appearances
Classification of Common Acetabular Fractures: Radiographic and CT Appearances
Uploaded by
Sharan SahotaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Classification of Common Acetabular Fractures: Radiographic and CT Appearances
Classification of Common Acetabular Fractures: Radiographic and CT Appearances
Uploaded by
Sharan SahotaCopyright:
Available Formats
Durkee et al.
M u s c u l o s ke l e t a l I m ag i n g • P i c t o r i a l E s s ay
Radiographic and CT
Classification of Acetabular
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Fractures
A C E N T U
R Y O F Classification of Common
Acetabular Fractures:
MEDICAL IMAGING
Radiographic and CT Appearances
N. Jarrod Durkee1,2 OBJECTIVE. Accurate characterization of acetabular fractures can be difficult because of
Jon Jacobson1 the complex acetabular anatomy and the many fracture patterns. In this article, the five most
David Jamadar1 common acetabular fractures are reviewed: both-column, T-shaped, transverse, transverse with
Madhav A. Karunakar3 posterior wall, and isolated posterior wall. Fracture patterns on radiography are correlated with
Yoav Morag1 CT, including multiplanar reconstruction and 3D surface rendering.
CONCLUSION. In the evaluation of the five most common acetabular fractures, assessment
Curtis Hayes1,4
of the obturator ring, followed by the iliopectineal and ilioischial lines and iliac wing, for fracture
Durkee NJ, Jacobson J, Jamadar D, allows accurate classification. CT is helpful in understanding the various fracture patterns.
Karunakar MA, Morag Y, Hayes C
ccurate classification of acetabular posterior column extends superiorly from the
A fractures is important for determin-
ing the proper surgical treatment
[1, 2]. Because of the complex ace-
ischiopubic ramus as the ischium toward the
ilium. The anterior and posterior columns of
bone unite to support the acetabulum. In turn,
tabular anatomy, various classification schemes the sciatic buttress extends posteriorly from
have been suggested [3–5], but the Judet-Le- the anterior and posterior columns to become
tournel classification system remains the most the articular surface of the sacroiliac joint,
widely accepted [2, 4, 6]. Although radio-
graphic examination provides essential infor-
Keywords: acetabular fracture, CT, musculoskeletal mation for acetabular classification, CT, includ-
imaging, pelvic imaging, radiography, trauma ing multiplanar reconstruction, is helpful in the
visualization of complex fractures [7].
DOI:10.2214/AJR.05.1269 This article reviews the pelvic bone anat-
Received July 21, 2005; accepted after revision
omy and the five most common acetabular
September 18, 2005. fractures: both-column, T-shaped, transverse,
transverse with posterior wall, and isolated
1Department of Radiology, University of Michigan Medical
posterior wall [2]. A fracture classification al-
Center, 1500 E Medical Center Dr., TC-2910G, Ann Arbor, MI gorithm based on radiography is used, with
48109-0326. Address correspondence to J. Jacobson
(jjacobsn@umich.edu).
correlation made to CT.
2Present address: Department of Radiology, University of Normal Anatomy: Columns and Walls
Washington, Seattle, WA. The acetabulum is formed by anterior and
3Department of Orthopedic Surgery, University of Michigan
posterior columns of bone, which join in the
Medical Center, Ann Arbor, MI 48109-0326. supraacetabular region [2, 6, 8]. The anterior
and posterior walls extend from each respec-
4Present address: Department of Radiology, Medical
tive column and form the cup of the acetabu-
College of Virginia, Virginia Commonwealth University, lum. The anterior and posterior columns con-
Richmond, VA.
nect to the axial skeleton through a strut of
CME bone called the sciatic buttress. When looking
This article is available for 1 CME credit. See www.arrs.org at the acetabulum en face, the anterior and A
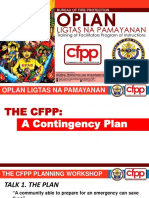
for more information. posterior columns have the appearance of the Fig. 1—Normal pelvic bone anatomy.
Greek letter lambda (λ) [2, 6] (Fig. 1A). The A, Surface-rendering 3D CT of pelvis in lateral view
AJR 2006; 187:915–925 with femur and right hemipelvis removed shows
anterior column represents the longer, larger anterior column (green), posterior column (blue), and
0361–803X/06/1874–915
portion, which extends superiorly from the sciatic buttress (red).
© American Roentgen Ray Society superior pubic ramus into the iliac wing. The (Fig. 1 continues on next page)
AJR:187, October 2006 915
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Durkee et al.
B C
Fig. 1 (continued)—Normal pelvic bone anatomy.
B, Axial section through acetabulum shows anterior (arrowhead) and posterior (arrow) walls.
C, Anteroposterior radiograph shows iliopectineal line (green), ilioischial line (blue), anterior acetabular wall (yellow), posterior acetabular wall (pink), and obturator foramen (O).
A B C
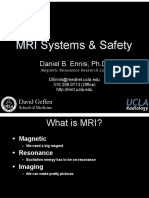
Fig. 2—Illustrations of classification of five most common acetabular fractures.
A, Both-column fracture.
B, T-shaped fracture.
C, Transverse fracture.
(Fig. 2 continues on next page)
which attaches the columns to the axial skel- On radiographs, the iliopectineal (or ilio- of the anterior and posterior walls are also
eton. The anterior and posterior walls, which pubic) line represents the border of the ante- identified. The obturator rings are composed
extend from the columns and support the hip rior column, and the ilioischial line represents of the osseous structures that surround the ob-
joint, are well seen on an axial CT (Fig. 1B). the posterior column [9] (Fig. 1C). The edges turator foramen, which include the superior
916 AJR:187, October 2006
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Radiographic and CT Classification of Acetabular Fractures
on the most common fracture patterns,
which represent 90% of acetabular frac-
tures [2, 6] (Fig. 2). The five most com-
mon fracture types may be divided into
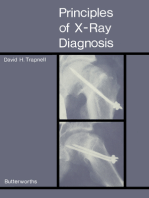
two groups on the basis of presence or ab-
sence of obturator ring fracture (Fig. 3).
Although fracture of the obturator ring
may be seen in combination with acetabu-
lar fractures, it is important to note that ob-
turator ring fractures may be associated
with other pelvic injuries outside of the ac-
etabulum, such as lateral pelvic compres-
sion injury, where the obturator ring frac-
ture is associated with either an ipsilateral
or contralateral sacral fracture [6].
We first discuss the two acetabular frac-
ture types (both-column and T-shaped)
associated with obturator ring disruption.
Next we discuss the three acetabular frac-
tures types that spare the obturator ring
(transverse, transverse with posterior wall,
and isolated posterior wall).
D E Both-Column Fracture
A both-column acetabular fracture (Figs. 4
Fig. 2 (continued)—Illustrations of classification of five most common acetabular fractures.
D, Transverse with posterior wall fracture. and 5) involves both anterior and posterior col-
E, Isolated posterior wall fracture. umns with extension into the obturator ring
and iliac wing, and is one of the most common
acetabular fractures [4]. On radiographs, frac-
ture involvement of the anterior and posterior
columns is characterized by disruption of the
iliopectineal line and ilioischial line, respec-
ACETABULAR
FRACTURE
tively. However, disruption of these lines may
IDENTIFIED also be seen with other fracture patterns, such
OBTURATOR
as a transverse fracture. Obturator ring and il-
RING iac wing involvement must also be present for
DISRUPTION?
YES NO
classification as a both-column acetabular
fracture. Fracture extension into the iliac wing
FRACTURE LINE ILIOISCHIAL AND
EXTENSION INTO ILIAC ILIOPECTINEAL LINE is not always obvious on the anteroposterior ra-
WING? DISRUPTION?
diograph; oblique Judet views or CT often re-
YES NO veal this finding.
YES NO POSTERIOR POSTERIOR On CT, fracture involvement of the ante-
WALL WALL
FRACTURE? FRACTURE?
rior and posterior columns is seen, and the
YES NO YES
fracture may be comminuted. Fracture dis-
Fig. 3—Classification ruption of the obturator ring has a variable
TRANSVERSE + ISOLATED
algorithm for five BOTH-COLUMN T-SHAPED
POSTERIOR WALL
TRANSVERSE
POSTERIOR
appearance; fracture of the superior pubic
FRACTURE FRACTURE FRACTURE
common acetabular FRACTURE WALL FRACTURE ramus may occur at the puboacetabular
fractures [2].
junction. In addition, fracture of the inferior
pubic ramus may be difficult to identify if
nondisplaced. The principal fracture line,
which extends superiorly from the acetabu-
lum into the iliac wing, is characteristically
pubic ramus and a combination of the inferior Fracture Patterns in the coronal plane.
pubic ramus and ischium (or ischiopubic ra- The most widely accepted classification If present, a pathognomonic sign of a
mus). Anteroposterior and bilateral oblique scheme for acetabular fractures is that of both-column fracture is the spur sign [2]
(or Judet) views of the pelvis are important to Judet and Letournel [2, 4, 6]. Although this (Fig. 5). This sign represents posterior dis-
adequately assess each of the radiographic classification scheme describes 10 types placement of the sciatic buttress of the iliac
lines for fracture. of acetabular fractures, we have focused wing fracture, which essentially discon-
AJR:187, October 2006 917
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Durkee et al.
nects the roof of the acetabulum from the shard of bone extending posteriorly at the T-Shaped Fracture
axial skeleton. When this occurs, weight level of the superior acetabulum. Evaluation A T-shaped acetabular fracture (Fig. 6) is a
from the torso and upper body can no longer of sequential CT images shows the fracture, combination of a transverse acetabular frac-
be supported by the acetabulum. On radio- which separates the sciatic buttress from the ture with extension inferiorly into the obtura-
graphs and CT, the spur sign appears as a acetabular roof. tor ring. It is similar to a both-column fracture
A B
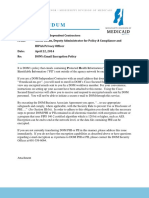
Fig. 4—45-year-old man with both-column acetabular fracture.
A–E, Anteroposterior pelvic radiograph (A), bilateral oblique pelvic radiographs (B,
C), axial CT scan (D), and sagittal reconstruction CT scan (E) show acetabular
fracture (straight arrows, A–C), with break in obturator ring (arrowheads, A–C) and
extension into iliac wing (curved arrows). Note coronal plane of fracture on CT and
superior pubic ramus fractured at puboacetabular junction.
(Fig. 4 continues on next page)
C
918 AJR:187, October 2006
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Radiographic and CT Classification of Acetabular Fractures
Fig. 4 (continued)—45-year-old man with both-column acetabular fracture.
A–E, Anteroposterior pelvic radiograph (A), bilateral oblique pelvic radiographs (B,
C), axial CT scan (D), and sagittal reconstruction CT scan (E) show acetabular
fracture (straight arrows, A–C), with break in obturator ring (arrowheads, A–C) and
extension into iliac wing (curved arrows). Note coronal plane of fracture on CT and
superior pubic ramus fractured at puboacetabular junction.
D E
Fig. 5—35-year-old man with both-column acetabular fracture and spur sign.
A and B, Oblique pelvic radiograph (A) and axial CT image (B) show spur sign (arrow),
which represents displacement of fracture involving sciatic buttress (arrowheads).
Note that sciatic buttress (arrowheads, B) no longer connects to weight-bearing
portion of acetabulum.
A B
in that it disrupts the obturator ring iliac wing, which allows differentiation from actually in the anatomic transverse plane, but
(Figs. 6A–6C). Another similarity is disrup- the both-column fracture. rather it is transverse relative to the acetabu-
tion of both the iliopectineal and ilioischial One area of potential confusion with the T- lum. Because the cup shape of the acetabulum
lines (Figs. 6A–6C). However, the superior shaped fracture is in regard to the transverse is normally tilted inferiorly and anteriorly, the
extension of the fracture does not involve the component. The transverse fracture line is not transverse fracture plane assumes a similar
AJR:187, October 2006 919
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Durkee et al.
A B
Fig. 6—40-year-old man with T-shaped acetabular fracture.
A–E, Anteroposterior pelvic radiograph (A), bilateral oblique pelvic radiographs (B,
C), axial CT scan (D), and surface-rendering 3D CT scan viewed laterally (E), with
right hemipelvis and femur removed, show obturator ring fractures (arrowheads) and
transverse component (arrows) through acetabulum. Note characteristic
oblique–sagittal orientation of transverse acetabular fracture component on CT
scans that is transverse relative to acetabulum on radiographs.
(Fig. 6 continues on next page)
orientation. Therefore, on radiographs, the Transverse Fracture fracture described previously, this fracture
fracture lines that disrupt the iliopectineal and The transverse fracture of the acetabu- line extends superiorly and medially from
ilioischial lines course superiorly and medi- lum (Fig. 7) is limited to the acetabulum, the acetabulum. On CT, the characteristic
ally in an oblique plane from the acetabulum. without involvement of the obturator ring. sagittally oriented fracture line can be seen
This is best appreciated by looking at the ac- A transverse fracture must involve both the moving laterally to medially on subsequent
etabulum en face (Fig. 6E). On CT, this trans- anterior and posterior aspects of the acetab- CT images when scrolling from inferior to
verse fracture component is seen as a sagit- ulum, so the iliopectineal and ilioischial superior. Although not anatomically trans-
tally oriented fracture coursing medially and lines are disrupted on radiography. Similar verse, the fracture plane is transverse rela-
superiorly from the acetabulum. to the transverse component of the T-shaped tive to the acetabulum, which is relatively
920 AJR:187, October 2006
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Radiographic and CT Classification of Acetabular Fractures
Fig. 6 (continued)—
40-year-old man with
T-shaped acetabular
fracture.
A–E, Anteroposterior
pelvic radiograph (A),
bilateral oblique pelvic
radiographs (B, C), axial
CT scan (D), and surface-
rendering 3D CT scan
viewed laterally (E), with
right hemipelvis and
femur removed, show
obturator ring fractures
(arrowheads) and
transverse component
(arrows) through
acetabulum. Note
characteristic
oblique–sagittal
orientation of transverse
acetabular fracture
component on CT scans
that is transverse relative
to acetabulum on
radiographs.
D E
A B
Fig. 7—23-year-old woman with transverse acetabular fracture.
A–E, Anteroposterior pelvic radiograph (A), bilateral oblique pelvic radiographs (B, C), axial CT scan (D), and surface-rendering 3D CT scan viewed laterally (E), with right
hemipelvis and femur removed, show fracture (arrows) orientation transverse to acetabulum, disrupting iliopectineal and ilioischial lines (arrowheads). Note characteristic
sagittal–oblique fracture plane on CT scan (D).
(Fig. 7 continues on next page)
tilted inferiorly and anteriorly. This fracture Transverse with Posterior Wall posterior wall fracture that is often displaced.
plane orientation is best seen on CT recon- The transverse with posterior wall fracture As with an isolated transverse fracture, the
struction images of the acetabulum en face (Fig. 8) is a transverse fracture, described pre- key is recognizing that the obturator ring is
(Fig. 7E). viously, with the addition of a comminuted not disrupted, as this excludes both-column
AJR:187, October 2006 921
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Durkee et al.
C
Fig. 7 (continued)—23-year-old woman with transverse acetabular fracture.
A–E, Anteroposterior pelvic radiograph (A), bilateral oblique pelvic radiographs (B,
C), axial CT scan (D), and surface-rendering 3D CT scan viewed laterally (E), with
right hemipelvis and femur removed, show fracture (arrows) orientation transverse
to acetabulum, disrupting iliopectineal and ilioischial lines (arrowheads). Note
characteristic sagittal–oblique fracture plane on CT scan (D).
and T-shaped fractures. As with the simple Isolated Posterior Wall Conclusion
transverse fracture, this fracture type does not The isolated posterior wall fracture Common acetabular fractures can easily be
extend into the iliac wing. (Fig. 9) is one of the most common types of classified using disruption of the obturator ring
On radiographs, disruption of both ilio- acetabular fracture, with a prevalence of as the basis of a decision tree (Fig. 3). Fracture
pectineal and ilioischial lines is seen as with 27% [8]. An isolated posterior wall fracture of the obturator ring indicates both-column or
the isolated transverse fracture. Unlike an iso- does not have a complete transverse acetab- T-shaped fracture, with additional iliac wing
lated transverse fracture, however, additional ular component. Therefore, the iliopectineal involvement differentiating the both-column
comminution of the posterior wall is seen. In line is not disrupted, which excludes classi- from the T-shaped fracture. Sparing of the ob-
the absence of displacement, comminution of fication of the transverse with posterior wall turator ring commonly indicates transverse,
the posterior wall may be difficult to identify fracture. However, disruption of the iliois- transverse with posterior wall, or isolated pos-
on anteroposterior radiographs because the chial line may or may not be present as an terior wall fracture. Disruption of both the ilio-
fragments are superimposed on the femoral extension of the comminuted posterior wall pectineal and ilioischial lines indicates a trans-
head. Oblique Judet radiographs and CT are component. Oblique (Judet) radiographs verse fracture, and comminution of the posterior
helpful in showing the comminuted posterior and CT are helpful in showing the isolated wall indicates a posterior wall fracture. A both-
wall component. posterior wall fracture. column fracture is in the coronal plane, whereas
922 AJR:187, October 2006
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Radiographic and CT Classification of Acetabular Fractures
A B
Fig. 8—20-year-old man showing transverse with posterior wall acetabular fracture.
A–E, Anteroposterior pelvic radiograph (A), bilateral oblique pelvic radiographs (B,
C), axial CT scan (D), and surface-rendering 3D CT scan viewed laterally (E), with
right hemipelvis and femur removed, show transverse fracture (straight arrows)
disrupting iliopectineal and ilioischial lines (arrowheads) with displaced and
comminuted posterior wall fracture fragment (curved arrows).
E
AJR:187, October 2006 923
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Durkee et al.
A B
Fig. 9—18-year-old man with isolated posterior wall acetabular fracture.
A–F, Anteroposterior pelvic radiograph (A), bilateral oblique pelvic radiographs (B,
C), axial CT images (D, E), and parasagittal reconstruction CT image (F) show
displaced fracture fragments (curved arrows) from isolated posterior wall fracture
(straight arrow, D).
(Fig. 9 continues on next page)
E
924 AJR:187, October 2006
Downloaded from www.ajronline.org by 2607:fea8:4fc0:7540:483d:123d:a7ca:8731 on 05/20/21 from IP address 2607:fea8:4fc0:7540:483d:123d:a7ca:8731. Copyright ARRS. For personal use only; all rights reserved
Radiographic and CT Classification of Acetabular Fractures
Fig. 9 (continued)— References
18-year-old man with 1. Goulet JA, Bray TJ. Complex acetabular fractures.
isolated posterior wall
acetabular fracture. Clin Orthop Relat Res 1989; 240:9–20
A–F, Anteroposterior 2. Brandser E, Marsh JL. Acetabular fractures: easier
pelvic radiograph (A), classification with a systematic approach. AJR
bilateral oblique pelvic
1998; 171:1217–1228
radiographs (B, C), axial
CT images (D, E), and 3. Judet R, Judet J, Letournel E. Fractures of the ace-
parasagittal tabulum: classification and surgical approaches for
reconstruction CT open reduction—preliminary report. J Bone Joint
image (F) show
displaced fracture Surg Am 1964; 46:1615–1646
fragments (curved 4. Letournel E, Judet R. Fractures of the acetabulum,
arrows) from isolated 2nd ed. Heidelberg, Germany: Springer-Verlag,
posterior wall fracture
(straight arrow, D). 1993
5. Harris JH Jr, Coupe KJ, Lee JS, Trotscher T. Ace-
tabular fractures revisited. Part 2. A new CT-based
classification. AJR 2004; 182:1367–1375
6. Hunter JC, Brandser EA, Tran KA. Pelvic and ac-
etabular trauma. Radiol Clin North Am 1997;
35:559–590
7. Falchi M, Rollandi GA. CT of pelvic fractures. Eur
J Radiol 2004; 50:96–105
8. Martinez CR, Di Pasquale TG, Helfet DL, Graham
AW, Sanders RW, Ray LD. Evaluation of acetabular
F fractures with two- and three-dimensional CT. Ra-
dioGraphics 1992; 12:227–242
9. Saks BJ. Normal acetabular anatomy for acetabular
a transverse or T-shaped fracture is in the sagit- Acknowledgment fracture assessment: CT and plain film correlation.
tal oblique plane on CT. The addition of CT We thank Robert W. Jacobson for the Radiology 1986; 159:139–145
with multiplanar reconstruction and 3D surface illustrations.
rendering is helpful in understanding and clas-
sifying acetabular fractures.
F O R YO U R I N F O R M AT I O N
This article is available for 1 CME credit. See www.arrs.org for more information.
AJR:187, October 2006 925
You might also like
- OLP CFPP The Contingency PlanDocument70 pagesOLP CFPP The Contingency PlanHerle Lobrino Barrios100% (2)
- Hip Fractures in The Frail Elderly: Is There Enough Evidence To Guide Management?Document17 pagesHip Fractures in The Frail Elderly: Is There Enough Evidence To Guide Management?Sharan SahotaNo ratings yet
- Classification of Common Acetabular Fractures: Radiographic and CT AppearancesDocument11 pagesClassification of Common Acetabular Fractures: Radiographic and CT AppearancesGeorge MathewNo ratings yet
- Acetabular FracturesDocument7 pagesAcetabular FracturesAltaf HossainNo ratings yet
- Ajr.12.10010 Aortic RootDocument9 pagesAjr.12.10010 Aortic Rootfranti76No ratings yet
- Cardiac MRI 1Document8 pagesCardiac MRI 1drpankajsNo ratings yet
- Comparison of Computed Tomography With Conventional Radiography For Midfacial FracturesDocument6 pagesComparison of Computed Tomography With Conventional Radiography For Midfacial FracturesadityailhamNo ratings yet
- Rita Barros - Wrist - And.hand - EULAR TTT 2022Document17 pagesRita Barros - Wrist - And.hand - EULAR TTT 2022Rita BarrosNo ratings yet
- Ankle and Foot Injuries:: Analysis of MDCT FindingsDocument8 pagesAnkle and Foot Injuries:: Analysis of MDCT FindingsraditNo ratings yet
- GCT ThumbDocument10 pagesGCT ThumbMoeez AkramNo ratings yet
- CTA ExtremityDocument8 pagesCTA Extremityrio trisonaNo ratings yet
- Brittle Microtectonics Principles and PR PDFDocument21 pagesBrittle Microtectonics Principles and PR PDFMartin GriffinNo ratings yet
- Lateral EpicondylitisDocument12 pagesLateral EpicondylitisIshitaNo ratings yet
- Cole 2013Document5 pagesCole 2013Angie MorrisNo ratings yet
- Ajr.07.2754 Jurnal Foreksik 1Document6 pagesAjr.07.2754 Jurnal Foreksik 1sintaNo ratings yet
- Galeazzi-Fracture 6Document14 pagesGaleazzi-Fracture 6MIGUEL ANGEL MEJIA FERNANDEZNo ratings yet
- Extein Et Al 2017 CT Findings of Traumatic Bucket Handle Mesenteric InjuriesDocument5 pagesExtein Et Al 2017 CT Findings of Traumatic Bucket Handle Mesenteric Injuries132 Naga VamsiNo ratings yet
- Orbital Blow Out FractureDocument8 pagesOrbital Blow Out FractureNickNo ratings yet
- Wrist Joint DislocationDocument10 pagesWrist Joint DislocationAnnisa HidayatiNo ratings yet
- Misses and Errors in Upper Extremity Trauma Radiographs: Soterios Gyftopoulos Munish Chitkara Jenny T. BencardinoDocument15 pagesMisses and Errors in Upper Extremity Trauma Radiographs: Soterios Gyftopoulos Munish Chitkara Jenny T. BencardinorasyidNo ratings yet
- Brittle MicrotectonicsDocument19 pagesBrittle MicrotectonicsPaul Quispe SolanoNo ratings yet
- Fracture of The Distal Radius: Epidemiology and Premanagement Radiographic CharacterizationDocument9 pagesFracture of The Distal Radius: Epidemiology and Premanagement Radiographic CharacterizationodivarNo ratings yet
- Isolated Tympanic Plate Fracture Frequency and - 2014 - Canadian Association ofDocument6 pagesIsolated Tympanic Plate Fracture Frequency and - 2014 - Canadian Association ofChilaka Priyanka1996No ratings yet
- Aydıngöz Et Al 2022 Zero Echo Time Musculoskeletal Mri Technique Optimization Applications and PitfallsDocument17 pagesAydıngöz Et Al 2022 Zero Echo Time Musculoskeletal Mri Technique Optimization Applications and PitfallsThuyet Nguyen PhuocNo ratings yet
- Brittle Microtectonics PDFDocument21 pagesBrittle Microtectonics PDFRenato Santiago100% (2)
- Diagnosis of Midface Fractures With CT: What The Surgeon Needs To KnowDocument24 pagesDiagnosis of Midface Fractures With CT: What The Surgeon Needs To KnowMohammad AdhityaNo ratings yet
- Arthrography in Recurrent Dislocation of The Elbow: Case ReportsDocument3 pagesArthrography in Recurrent Dislocation of The Elbow: Case ReportsDr LAUMONERIENo ratings yet
- Effect of The Properties of The Constituents On The Fatigue Performance of Composites: A ReviewDocument12 pagesEffect of The Properties of The Constituents On The Fatigue Performance of Composites: A ReviewM.Muslim RehmanNo ratings yet
- World Journal of Oral and Maxillofacial SurgeryDocument6 pagesWorld Journal of Oral and Maxillofacial SurgeryAshish AgarwalNo ratings yet
- Normative Measurements of Orbital Structures Using CT: Aiiozgen' Macit AriyurekDocument4 pagesNormative Measurements of Orbital Structures Using CT: Aiiozgen' Macit AriyurekLammii BoruuNo ratings yet
- Fractures of The Distal End of The Radius Treated by Internal Fixation and Early Function. A Preliminary Report of 20 CasesDocument6 pagesFractures of The Distal End of The Radius Treated by Internal Fixation and Early Function. A Preliminary Report of 20 Casessanjay chhawraNo ratings yet
- Kapandji Vs K-Wires StudyDocument6 pagesKapandji Vs K-Wires StudymonkeyzergNo ratings yet
- Gradient-Echo MR Imaging of The: Cervical Spine: Evaluation of Extradural DiseaseDocument6 pagesGradient-Echo MR Imaging of The: Cervical Spine: Evaluation of Extradural DiseaseSabrina MantikaNo ratings yet
- Lasers For The Treatment of Coronary Artery DiseaseDocument36 pagesLasers For The Treatment of Coronary Artery Diseasesurbhib268No ratings yet
- McGonagle2019 Article TibiaPlateauFractureMappingAndDocument6 pagesMcGonagle2019 Article TibiaPlateauFractureMappingAndFarizka Dwinda HNo ratings yet
- Imaging of Anterior Cruciate Ligament Repair and Its ComplicationsDocument9 pagesImaging of Anterior Cruciate Ligament Repair and Its ComplicationsDanaAmaranducaiNo ratings yet
- Clavicula FractureDocument6 pagesClavicula Fracturedrian pamungkasNo ratings yet
- Imaging Analyses of Bone Tumors JBJSDocument11 pagesImaging Analyses of Bone Tumors JBJSVera VeraNo ratings yet
- InterpretationDocument1 pageInterpretationsiriNo ratings yet
- Zygomatic Arch Deformation - An Anatomic and Clinical StudyDocument8 pagesZygomatic Arch Deformation - An Anatomic and Clinical StudyGabriel LeviNo ratings yet
- Nakagawa2002 Aplicacion Del CBCT en Ccirugia Oral Limitaciones en El PreoperatorioDocument5 pagesNakagawa2002 Aplicacion Del CBCT en Ccirugia Oral Limitaciones en El PreoperatorioIgnacio Roberto Gamboa MuñozNo ratings yet
- Ankle Ligaments On MRI: Appearance of Normal and Injured LigamentsDocument9 pagesAnkle Ligaments On MRI: Appearance of Normal and Injured Ligamentspjanu86No ratings yet
- Cardiac CT Part 2. Ekstracardiac Findings and Cardiac FunctionDocument15 pagesCardiac CT Part 2. Ekstracardiac Findings and Cardiac Functionafdhal.888980No ratings yet
- Multidetector CT of Midfacial Fractures: Classification Systems, Principles of Reduction, and Common ComplicationsDocument27 pagesMultidetector CT of Midfacial Fractures: Classification Systems, Principles of Reduction, and Common ComplicationsZaira TrejoNo ratings yet
- Scapular Fractures: What Radiologists Need To Know: Alan M. Ropp Derik L. DavisDocument11 pagesScapular Fractures: What Radiologists Need To Know: Alan M. Ropp Derik L. DavisikhsanNo ratings yet
- Tatuajes en MastografiaDocument2 pagesTatuajes en MastografiaJorge RojasNo ratings yet
- Lecture01 Residents MRI Systems and SafetyDocument109 pagesLecture01 Residents MRI Systems and SafetyMSNo ratings yet
- Diagnostic Imaging of The TMJ October 16 2020Document51 pagesDiagnostic Imaging of The TMJ October 16 2020AlysonNo ratings yet
- Radiograph Interpretation - WeldsDocument7 pagesRadiograph Interpretation - WeldsMejdi SANo ratings yet
- Frequently Used Grafts in RhinoplastyDocument16 pagesFrequently Used Grafts in RhinoplastyongchenguanNo ratings yet
- Ringe Et Al 2012 Gadoxetate Disodium Enhanced Mri of The Liver Part 1 Protocol Optimization and Lesion Appearance inDocument16 pagesRinge Et Al 2012 Gadoxetate Disodium Enhanced Mri of The Liver Part 1 Protocol Optimization and Lesion Appearance indynachNo ratings yet
- Rotator Cuff Tear: ImagingDocument7 pagesRotator Cuff Tear: ImagingAurelie VainNo ratings yet
- Prehensive Fracture Evaluation Using Wireline Borehole Imager and Array Acoustic ToolsDocument17 pagesPrehensive Fracture Evaluation Using Wireline Borehole Imager and Array Acoustic ToolsHerry SuhartomoNo ratings yet
- Abdominal MRI at 3.0 T: The Basics Revisited: Elmar M. Merkle Brian M. DaleDocument9 pagesAbdominal MRI at 3.0 T: The Basics Revisited: Elmar M. Merkle Brian M. DalehusadaNo ratings yet
- Micromechanisms of Brittle Fracture: OfbrittlefractureDocument12 pagesMicromechanisms of Brittle Fracture: Ofbrittlefractureamd mhmNo ratings yet
- Disc Displacement and Changes in Condylar PositionDocument8 pagesDisc Displacement and Changes in Condylar PositionCem ÜnsalNo ratings yet
- 3D Surface Crack Characterization by Eddy Current Array Image and A Fast Algorithm SearchDocument6 pages3D Surface Crack Characterization by Eddy Current Array Image and A Fast Algorithm SearchTarik BouchalaNo ratings yet
- 10 1061@asceem 1943-7889 0001822Document14 pages10 1061@asceem 1943-7889 0001822Can LiNo ratings yet
- CT MXFDocument6 pagesCT MXFAhmed KhattabNo ratings yet
- (Année) : Manual For Use by Geologists, Geophysicists and ProducersDocument12 pages(Année) : Manual For Use by Geologists, Geophysicists and ProducerslolobsNo ratings yet
- Normative Measurements of Orbital Structures Using CT: Aiiozgen' Macit AriyurekDocument4 pagesNormative Measurements of Orbital Structures Using CT: Aiiozgen' Macit AriyurekMoch NizamNo ratings yet
- Aspirin and Fracture Risk: A Systematic Review and Exploratory Meta-Analysis of Observational StudiesDocument12 pagesAspirin and Fracture Risk: A Systematic Review and Exploratory Meta-Analysis of Observational StudiesSharan SahotaNo ratings yet
- Purpureocillium Paecilomyces Lilacinus:, A New Genus For The Medically ImportantDocument9 pagesPurpureocillium Paecilomyces Lilacinus:, A New Genus For The Medically ImportantSharan SahotaNo ratings yet
- Preschool Stuttering - Parent Information Handbook: Speech-Language Pathologist But Here Are Some General GuidelinesDocument7 pagesPreschool Stuttering - Parent Information Handbook: Speech-Language Pathologist But Here Are Some General GuidelinesSharan SahotaNo ratings yet
- Burden of Illness For Osteoporotic Fractures Compared With Other Serious Diseases Among Postmenopausal Women in The United StatesDocument10 pagesBurden of Illness For Osteoporotic Fractures Compared With Other Serious Diseases Among Postmenopausal Women in The United StatesSharan SahotaNo ratings yet
- Plant Guide: Late LilacDocument2 pagesPlant Guide: Late LilacSharan SahotaNo ratings yet
- Pamidronate in The Treatment of Childhood SAPHO Syndrome: C. Kerrison, J. E. Davidson, A. G. Cleary and M. W. BeresfordDocument6 pagesPamidronate in The Treatment of Childhood SAPHO Syndrome: C. Kerrison, J. E. Davidson, A. G. Cleary and M. W. BeresfordSharan SahotaNo ratings yet
- Original Article: Splint Bone Fractures in The Horse: A Retrospective Study 1992-2001Document7 pagesOriginal Article: Splint Bone Fractures in The Horse: A Retrospective Study 1992-2001Sharan SahotaNo ratings yet
- PHP BR 15 0055Document2 pagesPHP BR 15 0055Sharan SahotaNo ratings yet
- JMCP 2017 23 7 735Document14 pagesJMCP 2017 23 7 735Sharan SahotaNo ratings yet
- Atypical Fracture With Long-Term Bisphosphonate Therapy Is Associated With Altered Cortical Composition and Reduced Fracture ResistanceDocument6 pagesAtypical Fracture With Long-Term Bisphosphonate Therapy Is Associated With Altered Cortical Composition and Reduced Fracture ResistanceSharan SahotaNo ratings yet
- Tracing Ancient Hydrogeological Fracture Network Age and Compartmentalisation Using Noble GasesDocument23 pagesTracing Ancient Hydrogeological Fracture Network Age and Compartmentalisation Using Noble GasesSharan SahotaNo ratings yet
- E914 FullDocument1 pageE914 FullSharan SahotaNo ratings yet
- Nej Mo A 1916525Document11 pagesNej Mo A 1916525Sharan SahotaNo ratings yet
- The Crucial Role of Neutrophil Granulocytes in Bone Fracture HealingDocument11 pagesThe Crucial Role of Neutrophil Granulocytes in Bone Fracture HealingSharan SahotaNo ratings yet
- Comparative of Probiotics Reveals Cecal Microbial Component Associated With Performance Parameters in BroilersDocument24 pagesComparative of Probiotics Reveals Cecal Microbial Component Associated With Performance Parameters in BroilersSharan SahotaNo ratings yet
- Fracture Growth in Layered and Discontinuous Media: Norm WarpinskiDocument20 pagesFracture Growth in Layered and Discontinuous Media: Norm WarpinskiSharan SahotaNo ratings yet
- Temperature? Warm and Cold Complex Regional Pain Syndromes: Differences Beyond SkinDocument10 pagesTemperature? Warm and Cold Complex Regional Pain Syndromes: Differences Beyond SkinSharan SahotaNo ratings yet
- 266 Correspondence: Diane - Gold@channing - Harvard.eduDocument2 pages266 Correspondence: Diane - Gold@channing - Harvard.eduSharan SahotaNo ratings yet
- Evidence-Based Review) : Report of The Quality Standards Subcommittee of The Practice Parameter: Assessing Patients in A Neurology Practice For Risk of Falls (AnDocument9 pagesEvidence-Based Review) : Report of The Quality Standards Subcommittee of The Practice Parameter: Assessing Patients in A Neurology Practice For Risk of Falls (AnSharan SahotaNo ratings yet
- Economic Evaluation Alongside The Probiotics To Prevent Severe Pneumonia and Endotracheal Colonization Trial (E-PROSPECT) : Study ProtocolDocument8 pagesEconomic Evaluation Alongside The Probiotics To Prevent Severe Pneumonia and Endotracheal Colonization Trial (E-PROSPECT) : Study ProtocolSharan SahotaNo ratings yet
- Intestinal Microbiota in Human Health and Disease: The Impact of ProbioticsDocument32 pagesIntestinal Microbiota in Human Health and Disease: The Impact of ProbioticsSharan SahotaNo ratings yet
- Mechanical Thrombectomy in The Era of The COVID-19 Pandemic: Emergency Preparedness For Neuroscience TeamsDocument6 pagesMechanical Thrombectomy in The Era of The COVID-19 Pandemic: Emergency Preparedness For Neuroscience TeamsSharan SahotaNo ratings yet
- Value at Induced Risk: Injection Induced Seismic Risk From Low Probability, High Impact EventsDocument11 pagesValue at Induced Risk: Injection Induced Seismic Risk From Low Probability, High Impact EventsSharan SahotaNo ratings yet
- Vanderlaan Taggart MarMamSci-23 2007Document13 pagesVanderlaan Taggart MarMamSci-23 2007Sharan SahotaNo ratings yet
- CPJ 0000000000000836 FullDocument12 pagesCPJ 0000000000000836 FullSharan SahotaNo ratings yet
- Vrot EnvDocument19 pagesVrot EnvSharan SahotaNo ratings yet
- Rmrs 2016 Wilcox t001Document8 pagesRmrs 2016 Wilcox t001Sharan SahotaNo ratings yet
- Email Encryption Memo Download in PDF FormatDocument6 pagesEmail Encryption Memo Download in PDF FormatAri BencuyaNo ratings yet
- Preliminaries: Volume 1: The Comprehensive Land Use PlanDocument40 pagesPreliminaries: Volume 1: The Comprehensive Land Use PlanJerson BuanNo ratings yet
- Caries Diagnosis and TreatmentDocument18 pagesCaries Diagnosis and Treatmentrxmskdkd33No ratings yet
- Site Mobilzation PlanDocument18 pagesSite Mobilzation PlanRAMY ABOU AL DAHABNo ratings yet
- Mouth Cancer Research PaperDocument6 pagesMouth Cancer Research Paperqhujvirhf100% (1)
- New Introduction Rachel MiliaccaDocument9 pagesNew Introduction Rachel Miliaccaapi-285111901No ratings yet
- Abdominal TuberculosisDocument9 pagesAbdominal TuberculosisImmanuelNo ratings yet
- Acupuncture ObesityDocument4 pagesAcupuncture Obesityferry7765100% (1)
- ოქსფორდის სახელმძღვანელო ფსიქიატრიაში 4Document9 pagesოქსფორდის სახელმძღვანელო ფსიქიატრიაში 4a.utiashviliNo ratings yet
- 04-25-13 EditionDocument36 pages04-25-13 EditionSan Mateo Daily JournalNo ratings yet
- Reino FungiDocument1 pageReino FungiRuben Choquicota MaquitoNo ratings yet
- Diagnosis and Management of Tremor.11Document16 pagesDiagnosis and Management of Tremor.11Stephanie Queiroz Dos SantosNo ratings yet
- Risk Assesment CSSDDocument9 pagesRisk Assesment CSSDTianti Puadi100% (1)
- ITFAS Ambassador Presentation 2Document27 pagesITFAS Ambassador Presentation 2Sugeng WahyudiNo ratings yet
- Malnutrition NCPDocument4 pagesMalnutrition NCPDenise Espinosa100% (3)
- Social 1Document59 pagesSocial 1Jessa DongaNo ratings yet
- Vet Radiology Ultrasound - 2011 - Hittmair - RADIOGRAPHIC AND ULTRASONOGRAPHIC DIAGNOSIS OF STENOSING TENOSYNOVITIS OF THEDocument7 pagesVet Radiology Ultrasound - 2011 - Hittmair - RADIOGRAPHIC AND ULTRASONOGRAPHIC DIAGNOSIS OF STENOSING TENOSYNOVITIS OF THECésar Sa JimNo ratings yet
- Worksheet - Digestive System - 2020-21Document9 pagesWorksheet - Digestive System - 2020-21riddhiNo ratings yet
- NCM 109 Pedia PreschoolDocument11 pagesNCM 109 Pedia PreschoolMantilla, Kristina Cassandra A.No ratings yet
- A Clinical Guide To Orthodontics - J. Sandy (2004) WW PDFDocument77 pagesA Clinical Guide To Orthodontics - J. Sandy (2004) WW PDFAntonela CeremușNo ratings yet
- Biology: PAPER 6 Alternative To PracticalDocument12 pagesBiology: PAPER 6 Alternative To Practicalmstudy1234560% (1)
- Summit One Condominium Corp. vs. PAB - Yung Wasterwater SampleDocument3 pagesSummit One Condominium Corp. vs. PAB - Yung Wasterwater SampleAra GrospeNo ratings yet
- Green Tea ExtractDocument1 pageGreen Tea Extractajitbadboy2No ratings yet
- SerratiaDocument26 pagesSerratiaduverney.gaviriaNo ratings yet
- Experiment 5 LipidsDocument13 pagesExperiment 5 LipidsClemence Marie FuentesNo ratings yet
- Chapter 8 Electrical ServiceDocument7 pagesChapter 8 Electrical ServicepavloneNo ratings yet
- Orem Based Brain Rehab Clinic Is The First in The State To Offer Innovative GyroStim Neuro TherapyDocument2 pagesOrem Based Brain Rehab Clinic Is The First in The State To Offer Innovative GyroStim Neuro TherapyPR.comNo ratings yet
- Nursing Care Plan - NCP-PIHDocument4 pagesNursing Care Plan - NCP-PIHAally ChandraNo ratings yet
- The Last LeafDocument3 pagesThe Last Leafyana931931No ratings yet