Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Surgery Viva QuestionsDocument24 pagesSurgery Viva QuestionsKay Bristol90% (10)
- Clinical Laboratory Medicine: 2nd EditionDocument1,709 pagesClinical Laboratory Medicine: 2nd EditionBeatriz BelottiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Med Surg Test 4 Study GuideDocument29 pagesMed Surg Test 4 Study GuideJess100% (2)
- MOH Pocket Manual in General SurgeryDocument118 pagesMOH Pocket Manual in General SurgeryPavel Luna100% (1)
- (Artigo) (Procedimentos) Effectiveness of Different Central Venous Catheter Fixation Suture Techniques: An in Vitro Crossover StudyDocument11 pages(Artigo) (Procedimentos) Effectiveness of Different Central Venous Catheter Fixation Suture Techniques: An in Vitro Crossover StudyBeatriz BelottiNo ratings yet
- (Artigo) (CG) (Nutrição) Pre-Operative Nutrition and The Elective Surgical Patient - Why, How and What Gillis (2019)Document9 pages(Artigo) (CG) (Nutrição) Pre-Operative Nutrition and The Elective Surgical Patient - Why, How and What Gillis (2019)Beatriz BelottiNo ratings yet
- Dual Plane Breast Augmentation: Optimizing Implant-Soft-Tissue Relationships in A Wide Range of Breast TypesDocument18 pagesDual Plane Breast Augmentation: Optimizing Implant-Soft-Tissue Relationships in A Wide Range of Breast TypesBeatriz BelottiNo ratings yet
- (Artigo) (CG) (Classificacão) Recent Classifications of The Common Bile Duct Injury (2014)Document4 pages(Artigo) (CG) (Classificacão) Recent Classifications of The Common Bile Duct Injury (2014)Beatriz BelottiNo ratings yet
- Lzizj: Comprehensive Manuals of Surgical SpecialtiesDocument288 pagesLzizj: Comprehensive Manuals of Surgical SpecialtiesBeatriz BelottiNo ratings yet
- (Artigo) Jardini Barbosa (2009)Document4 pages(Artigo) Jardini Barbosa (2009)Beatriz BelottiNo ratings yet
- Chole CystitisDocument61 pagesChole CystitisPlain GerlNo ratings yet
- Anatomy Liver, Biliary, Pancreas and Spleen 2022Document58 pagesAnatomy Liver, Biliary, Pancreas and Spleen 2022Osama AbdelazizNo ratings yet
- Cholelithiasis Treatment & ManagementDocument8 pagesCholelithiasis Treatment & ManagementRayhanun MardhatillahNo ratings yet
- NutriDiet ReviewerDocument6 pagesNutriDiet ReviewerCherry BoticarioNo ratings yet
- Cynara Scolymus ArtichokeDocument8 pagesCynara Scolymus Artichokeplanet_renNo ratings yet
- Cholel FinalDocument39 pagesCholel FinalRizza DaleNo ratings yet
- Rekomendasi Antibiotik Pada Profilaksis BedahDocument4 pagesRekomendasi Antibiotik Pada Profilaksis BedahRya At ChinnamorariaNo ratings yet
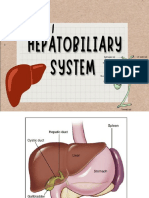
- Hepatobiliary SystemDocument131 pagesHepatobiliary SystemCurt Leye RodriguezNo ratings yet
- Acute CholecystitisDocument27 pagesAcute CholecystitisAleks MendozaNo ratings yet
- Protocol of UltrasoundDocument22 pagesProtocol of UltrasoundAzie Azizah AGNo ratings yet
- Bile Production - Constituents - TeachMePhysiologyDocument2 pagesBile Production - Constituents - TeachMePhysiologynotesom44No ratings yet
- Pone D 24 09157Document27 pagesPone D 24 09157Wilson Adrian WijayaNo ratings yet
- Frog Digestive SystemDocument2 pagesFrog Digestive SystemNiezhel Anne JimenezNo ratings yet
- Radiology Casebook ExamDocument23 pagesRadiology Casebook ExamNiko Montgomery0% (1)
- Digestion ResonanceDocument52 pagesDigestion ResonanceEkta ManglaniNo ratings yet
- Early Recurrence of Carcinoma Gall Bladder After R0 Resection of Stage T1B-T3Document6 pagesEarly Recurrence of Carcinoma Gall Bladder After R0 Resection of Stage T1B-T3IJAR JOURNALNo ratings yet
- Indications and Complications of ErcpDocument57 pagesIndications and Complications of ErcpNuha AL-YousfiNo ratings yet
- Effectiveness of Tokyoguidelines 2018 in The Management of Acute Cholangitis and Acute CholecystitisDocument13 pagesEffectiveness of Tokyoguidelines 2018 in The Management of Acute Cholangitis and Acute CholecystitisIJAR JOURNALNo ratings yet
- Ultrasonographic Differences Between Dogs and CatsDocument13 pagesUltrasonographic Differences Between Dogs and Catsludiegues752No ratings yet
- 11 Gallbladder Cholesterolosis - Libre PathologyDocument3 pages11 Gallbladder Cholesterolosis - Libre PathologyfadoNo ratings yet
- Cholecystitis Litiasis EctomyDocument23 pagesCholecystitis Litiasis EctomyTimothy WilliamsNo ratings yet
- 10.1007@s00261 019 02364 XDocument12 pages10.1007@s00261 019 02364 XPNo ratings yet
- Digestion AND Absorption: - 1 - HSE Zoology BlogDocument88 pagesDigestion AND Absorption: - 1 - HSE Zoology BlogMahir AfranNo ratings yet
- Spark Zoology XI XII Eng 1Document16 pagesSpark Zoology XI XII Eng 1dfdsfsdefsdNo ratings yet
- Kebo116 PDFDocument13 pagesKebo116 PDFbashraaNo ratings yet
- Diagnostic Ultrasound Abdomen and Pelvis 2Nd Edition Aya Kamaya Full ChapterDocument67 pagesDiagnostic Ultrasound Abdomen and Pelvis 2Nd Edition Aya Kamaya Full Chapterkevin.larson517100% (19)
- Biliary Atresia Digestive IVDocument13 pagesBiliary Atresia Digestive IVherdigunantaNo ratings yet