
Study 4
Study 4
You might also like
- Lab Result Chart With Normal Range, Purpose, Reason For High/low Results (Nursing)Document5 pagesLab Result Chart With Normal Range, Purpose, Reason For High/low Results (Nursing)Linsey Bowen100% (6)
- The Top 50 High-Yield USMLE® Step 1 TopicsDocument10 pagesThe Top 50 High-Yield USMLE® Step 1 TopicsRubayet Tasfin Alif100% (3)
- Camgfr V2: A New Model For Estimating The Glomerular Filtration Rate From Standardized or Non-Standardized Creatinine in Patients With CancerDocument10 pagesCamgfr V2: A New Model For Estimating The Glomerular Filtration Rate From Standardized or Non-Standardized Creatinine in Patients With CancerMaria Jose Gonzalez FarrisNo ratings yet
- AinsworthDocument9 pagesAinsworthJesse Helmut Hansen-BartelNo ratings yet
- Bosl 1988Document8 pagesBosl 1988Bruno AlanNo ratings yet
- 8235.full AACRDocument9 pages8235.full AACRMohammed Khair BashirNo ratings yet
- 1 s2.0 S0302283818300198 MainDocument7 pages1 s2.0 S0302283818300198 MainM Rizqi FiryalNo ratings yet
- Drug Dosing and Estimates of Kidney Function: Michael P Bosomworth and Jonathan AT SandoeDocument3 pagesDrug Dosing and Estimates of Kidney Function: Michael P Bosomworth and Jonathan AT SandoeJesse Helmut Hansen-BartelNo ratings yet
- CKD - Drug DosingDocument7 pagesCKD - Drug DosingRafaelNo ratings yet
- NGS de Panel para CCR - JCO 2015 - Costo-EfectividadDocument12 pagesNGS de Panel para CCR - JCO 2015 - Costo-EfectividadSebas Barrionuevo VediaNo ratings yet
- Population Pharmacokinetic Comparison and Pharmacodynamic Breakpoints of Ceftazidime in Cystic Fibrosis Patients and Healthy VolunteersDocument8 pagesPopulation Pharmacokinetic Comparison and Pharmacodynamic Breakpoints of Ceftazidime in Cystic Fibrosis Patients and Healthy Volunteershailemicael mesfinNo ratings yet
- Jco 2016 71 7397Document9 pagesJco 2016 71 7397brasilianaraNo ratings yet
- Novel Diagnostic and Predictive Biomarkers in Pancreatic AdenocarcinomaDocument14 pagesNovel Diagnostic and Predictive Biomarkers in Pancreatic AdenocarcinomaChavdarNo ratings yet
- Overestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementDocument7 pagesOverestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementJesse Helmut Hansen-BartelNo ratings yet
- Cu Line 2007Document8 pagesCu Line 2007Bruno AlanNo ratings yet
- Prognostic Value of C Reactive Protein - AlbuminDocument8 pagesPrognostic Value of C Reactive Protein - AlbuminfernandallmagalhaesNo ratings yet
- Shi Et AlDocument7 pagesShi Et AlK. O.No ratings yet
- A Retrospective Analysis of Magnetic Resonance Cholangiopancreatography Investigating Gallstones in A Contemporary Surgical SettingDocument6 pagesA Retrospective Analysis of Magnetic Resonance Cholangiopancreatography Investigating Gallstones in A Contemporary Surgical SettingRupak GhimireNo ratings yet
- Estimating Glomerular Filtration Rate From Serum Creatinine and Cystatin CDocument10 pagesEstimating Glomerular Filtration Rate From Serum Creatinine and Cystatin CIsyfaun NisaNo ratings yet
- Fórmulas para El Cálculo de Filtración GlomerularDocument7 pagesFórmulas para El Cálculo de Filtración GlomerularNoel Saúl Argüello SánchezNo ratings yet
- 1 s2.0 S245210942100097X MainDocument7 pages1 s2.0 S245210942100097X MainhidayatullahhaqyaarNo ratings yet
- CRP 2 PDFDocument8 pagesCRP 2 PDFAdarsiya JayakumarNo ratings yet
- Does Obesity Impact Lymph Node Retrieval in Colon CancerDocument5 pagesDoes Obesity Impact Lymph Node Retrieval in Colon Cancersee yinNo ratings yet
- Jcav 07 P 1701Document10 pagesJcav 07 P 1701leehongkaiNo ratings yet
- Treatment of Advanced or Recurrent Cervical Cancer With Cisplatin or Cisplatin Containing Regimens: A Cost Effective AnalysisDocument5 pagesTreatment of Advanced or Recurrent Cervical Cancer With Cisplatin or Cisplatin Containing Regimens: A Cost Effective Analysisyahya restiNo ratings yet
- The Role of FDG-PET Scans in Patients With Lymphoma: Review in Translational HematologyDocument11 pagesThe Role of FDG-PET Scans in Patients With Lymphoma: Review in Translational HematologyPunam SinhaNo ratings yet
- Pros TataDocument8 pagesPros TataMartin ElenaNo ratings yet
- PIIS1548559517301738Document7 pagesPIIS1548559517301738Joseph BoatengNo ratings yet
- The Role of Hypofractionated Radiotherapy in ProstDocument10 pagesThe Role of Hypofractionated Radiotherapy in ProstАнастасия АнохинаNo ratings yet
- Qi 2022Document12 pagesQi 2022Jonathan Billy ChristianNo ratings yet
- Clinical Laboratory Analysis - 2012 - Hashad - Free Circulating Tumor DNA As A Diagnostic Marker For Breast CancerDocument6 pagesClinical Laboratory Analysis - 2012 - Hashad - Free Circulating Tumor DNA As A Diagnostic Marker For Breast Cancerfaraz.mirza1No ratings yet
- Beriwal 2006Document5 pagesBeriwal 2006Bruno MendesNo ratings yet
- 10 1016@j Critrevonc 2020 102962Document16 pages10 1016@j Critrevonc 2020 102962bouh aichetouNo ratings yet
- 10 1200@jco 2001 19 6 1629Document12 pages10 1200@jco 2001 19 6 1629Bruno AlanNo ratings yet
- Pooled Rates of Adenoma Detection by ColonosDocument29 pagesPooled Rates of Adenoma Detection by ColonoscarolinaNo ratings yet
- CreatinineDocument7 pagesCreatinineLintang SuroyaNo ratings yet
- 1 s2.0 S0167814016000736 MainDocument7 pages1 s2.0 S0167814016000736 MainOkky HusainNo ratings yet
- CMW 051Document4 pagesCMW 051Laila Kurnia PramonoNo ratings yet
- New Creatinine-And Cystatin C-Based Equations To Estimate GFR Without RaceDocument13 pagesNew Creatinine-And Cystatin C-Based Equations To Estimate GFR Without RaceAlizaPinkyNo ratings yet
- Kenapa Pakai Formula SendiriDocument11 pagesKenapa Pakai Formula SendiriYoan RahmahNo ratings yet
- EeDocument8 pagesEeEstiPramestiningtyasNo ratings yet
- Ournal of Linical Ncology: PurposeDocument7 pagesOurnal of Linical Ncology: PurposeIvor Wiguna Hartanto WilopoNo ratings yet
- Clinical 88 (8620 CorrectionsDocument12 pagesClinical 88 (8620 CorrectionsLiv IuNo ratings yet
- Renal PhysiologyDocument7 pagesRenal PhysiologyLucas TheotonioNo ratings yet
- Role of Carbohydrate Antigen (Ca19-9) and Carcinoembryonic Antigen (Cea) As A Prognostic Factors in Pancreatic CarcinomaDocument6 pagesRole of Carbohydrate Antigen (Ca19-9) and Carcinoembryonic Antigen (Cea) As A Prognostic Factors in Pancreatic CarcinomaIJAR JOURNALNo ratings yet
- Aspirin and Colorectal DiagnosisDocument7 pagesAspirin and Colorectal DiagnosisErnesto PiconNo ratings yet
- ESR Vs CRPDocument6 pagesESR Vs CRPMuhammad Imran MirzaNo ratings yet
- ANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFDocument8 pagesANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFRong LiuNo ratings yet
- Paper 2 Cancer DicoveryDocument18 pagesPaper 2 Cancer DicoverySuraj ShahNo ratings yet
- Kansal 2018Document1 pageKansal 2018Sheena Mae MansinadesNo ratings yet
- Kondagunta 2005Document5 pagesKondagunta 2005Bruno AlanNo ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- Damit 2022 (KRAS)Document10 pagesDamit 2022 (KRAS)Healthcare Pro LearningNo ratings yet
- Cholong It As 2016Document2 pagesCholong It As 2016arieftamaNo ratings yet
- Kolagocarsinoma PDFDocument7 pagesKolagocarsinoma PDFBerlyan RuslanNo ratings yet
- Circulating Endothelial Cells and Other Angiogenesis Factors in Pancreatic Carcinoma Patients Receiving Gemcitabine ChemotherapyDocument10 pagesCirculating Endothelial Cells and Other Angiogenesis Factors in Pancreatic Carcinoma Patients Receiving Gemcitabine ChemotherapyftwNo ratings yet
- Hand RefractometerDocument5 pagesHand RefractometerAntigona2001No ratings yet
- Jeffrey L Carson Restrictive or Liberal TransfusionDocument11 pagesJeffrey L Carson Restrictive or Liberal Transfusionmiguel aghelNo ratings yet
- Articulo de HistologiaDocument6 pagesArticulo de HistologiaalexbowwNo ratings yet
- Faecal Occult Blood Screening Reduced The Incidence of Colorectal CancerDocument1 pageFaecal Occult Blood Screening Reduced The Incidence of Colorectal CancerAgus PraktyasaNo ratings yet
- A Review of The Role of Carcinoembryonic Antigen IDocument12 pagesA Review of The Role of Carcinoembryonic Antigen IMarcellia AngelinaNo ratings yet
- Facta About Pediatric-Nasopharyngeal-CarcinomaDocument8 pagesFacta About Pediatric-Nasopharyngeal-CarcinomaJesse Helmut Hansen-BartelNo ratings yet
- Results of Proton ReirradiationDocument9 pagesResults of Proton ReirradiationJesse Helmut Hansen-BartelNo ratings yet
- Comparative Treatment Planning Study of Photons and ProtonsDocument15 pagesComparative Treatment Planning Study of Photons and ProtonsJesse Helmut Hansen-BartelNo ratings yet
- Pediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsDocument5 pagesPediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsJesse Helmut Hansen-BartelNo ratings yet
- JZareh Coarctation Aorta Case PresDocument13 pagesJZareh Coarctation Aorta Case PresJesse Helmut Hansen-BartelNo ratings yet
- SVC SyndromeDocument17 pagesSVC SyndromeJesse Helmut Hansen-BartelNo ratings yet
- Paediatric Trauma - DR Nicole WilliamsDocument36 pagesPaediatric Trauma - DR Nicole WilliamsJesse Helmut Hansen-BartelNo ratings yet
- Update in Inflammatory Bowel Disease: Graham MorrisonDocument6 pagesUpdate in Inflammatory Bowel Disease: Graham MorrisonJesse Helmut Hansen-BartelNo ratings yet
- Gestational Alloimmune Liver Disease: Ethan TangDocument14 pagesGestational Alloimmune Liver Disease: Ethan TangJesse Helmut Hansen-BartelNo ratings yet
- AinsworthDocument9 pagesAinsworthJesse Helmut Hansen-BartelNo ratings yet
- Carboplatin Dosing 2nd Draft DrLinkDocument4 pagesCarboplatin Dosing 2nd Draft DrLinkJesse Helmut Hansen-BartelNo ratings yet
- Filamin A Mutations: Jesse Hansen-BartelDocument8 pagesFilamin A Mutations: Jesse Hansen-BartelJesse Helmut Hansen-BartelNo ratings yet
- Mar FansDocument14 pagesMar FansJesse Helmut Hansen-BartelNo ratings yet
- Overestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementDocument7 pagesOverestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementJesse Helmut Hansen-BartelNo ratings yet
- Prospective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaDocument8 pagesProspective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaJesse Helmut Hansen-BartelNo ratings yet
- Should We Continue To Use The Cockcroft-Gault Formula?: MinireviewDocument15 pagesShould We Continue To Use The Cockcroft-Gault Formula?: MinireviewJesse Helmut Hansen-BartelNo ratings yet
- Validity of Prediction Models: When Is A Model Clinically Useful?Document20 pagesValidity of Prediction Models: When Is A Model Clinically Useful?Jesse Helmut Hansen-BartelNo ratings yet
- Ekhart2009 Article CarboplatinDosingInOverweightADocument8 pagesEkhart2009 Article CarboplatinDosingInOverweightAJesse Helmut Hansen-Bartel100% (1)
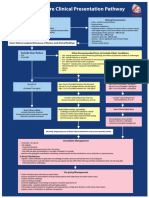
- Heart Failure Clinical Presentation PathwayDocument1 pageHeart Failure Clinical Presentation PathwayJesse Helmut Hansen-BartelNo ratings yet
- Study 3Document12 pagesStudy 3Jesse Helmut Hansen-BartelNo ratings yet
- How To Adjust Drug Doses in Chronic Kidney DiseaseDocument5 pagesHow To Adjust Drug Doses in Chronic Kidney DiseaseJesse Helmut Hansen-BartelNo ratings yet
- Chinkenl 2014 PHDDocument227 pagesChinkenl 2014 PHDJesse Helmut Hansen-BartelNo ratings yet
- Bsa 2Document4 pagesBsa 2Jesse Helmut Hansen-BartelNo ratings yet
- Study 1Document9 pagesStudy 1Jesse Helmut Hansen-BartelNo ratings yet
- For The Clinician: Estimation of Kidney Function in OncologyDocument9 pagesFor The Clinician: Estimation of Kidney Function in OncologyJesse Helmut Hansen-BartelNo ratings yet
- The Investigation of Wound Healing DisordersDocument15 pagesThe Investigation of Wound Healing DisordersRadulescu IonelaNo ratings yet
- Usg Abdomen Pelvis MaleDocument2 pagesUsg Abdomen Pelvis MaleBhaktivedanta HospitalNo ratings yet
- Blood Pressure Regulation - SlidesDocument35 pagesBlood Pressure Regulation - Slidesمحمد السنجلاويNo ratings yet
- Excretion in Humans Igcse BiologyDocument26 pagesExcretion in Humans Igcse BiologyThe PassionNo ratings yet
- ICSE Sample Papers For Class 7 Biology Part 1 (2023-24)Document9 pagesICSE Sample Papers For Class 7 Biology Part 1 (2023-24)Dr. M. PrinceNo ratings yet
- Diuretics IDocument17 pagesDiuretics Iأمجد محمدNo ratings yet
- CPSP Demo Mcqs - 2022Document24 pagesCPSP Demo Mcqs - 2022Farhan AfzalNo ratings yet
- RENAL Nephrometry Scoring System: The Radiologist's PerspectiveDocument5 pagesRENAL Nephrometry Scoring System: The Radiologist's PerspectiveGaltieri OtavioNo ratings yet
- Exercise 9 Diet RX: 2000 Kcal CHO-325G Protein - 75G FATS - 44.4GDocument8 pagesExercise 9 Diet RX: 2000 Kcal CHO-325G Protein - 75G FATS - 44.4Gjho piangNo ratings yet
- Kidney and Liver FunctionDocument6 pagesKidney and Liver FunctionAhmad Ripani Musyaffa AhdanLabNo ratings yet
- Kidney Food RecipesDocument11 pagesKidney Food RecipesLouie Cedrick Camposano TriaNo ratings yet
- Pharmacokinetics of Clozapine and Its Metabolites in Psychiatric Patients: Plasma Protein Binding and Renal ClearanceDocument7 pagesPharmacokinetics of Clozapine and Its Metabolites in Psychiatric Patients: Plasma Protein Binding and Renal ClearancegowaryNo ratings yet
- Renal Effects of NSAIDDocument8 pagesRenal Effects of NSAIDtaner_soysurenNo ratings yet
- Anatomy and Physiology Module 2Document16 pagesAnatomy and Physiology Module 2JayR MendonesNo ratings yet
- ASN - Phenotype and Outcomes of Acute Kidney Injury Associated With COVID-19 in Urban New OrleansDocument1 pageASN - Phenotype and Outcomes of Acute Kidney Injury Associated With COVID-19 in Urban New OrleansCésar Hernández-ArroyoNo ratings yet
- Dr. Erlieza Roosdhania, SP - PD (CKD)Document38 pagesDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNo ratings yet
- Drug StudyDocument3 pagesDrug StudyKristine Faith AzcuetaNo ratings yet
- Doppler Ultrasound of The KidneysDocument23 pagesDoppler Ultrasound of The KidneysivoklarinNo ratings yet
- Potter Syndrome: A Case Study: August 2017Document6 pagesPotter Syndrome: A Case Study: August 2017rmysdsNo ratings yet
- Biology O Level 5090 SylllabusDocument35 pagesBiology O Level 5090 SylllabusBalakrishnan MarappanNo ratings yet
- Renal Function TestsDocument31 pagesRenal Function TestsPhysiology by Dr RaghuveerNo ratings yet
- Pex 09 01Document5 pagesPex 09 01Gerardien Elham AfifahNo ratings yet
- Blood Pressure in Early Autosomal Dominant Polycystic Kidney DiseaseDocument5 pagesBlood Pressure in Early Autosomal Dominant Polycystic Kidney DiseaseNancy MolinaNo ratings yet
- Urinalysis Practice QuizDocument4 pagesUrinalysis Practice QuizGrace GasconNo ratings yet
- Ion Transport, Osmoregulation, and Acid Base BalanceDocument54 pagesIon Transport, Osmoregulation, and Acid Base Balancefikriafis100% (1)
- Sulfonamides: (Veterinary-Systemic)Document17 pagesSulfonamides: (Veterinary-Systemic)Ursula HilleNo ratings yet
- Unit - V Chapter-22. Excretory Products and Their EliminationDocument15 pagesUnit - V Chapter-22. Excretory Products and Their EliminationBattuJayakrishnaNo ratings yet
- Fenofibrate-Associated Nephrotoxicity: A Review of Current EvidenceDocument8 pagesFenofibrate-Associated Nephrotoxicity: A Review of Current EvidencefevianaNo ratings yet















































































































Download as pdf or txt
You might also like
- Lab Result Chart With Normal Range, Purpose, Reason For High/low Results (Nursing)Document5 pagesLab Result Chart With Normal Range, Purpose, Reason For High/low Results (Nursing)Linsey Bowen100% (6)
- The Top 50 High-Yield USMLE® Step 1 TopicsDocument10 pagesThe Top 50 High-Yield USMLE® Step 1 TopicsRubayet Tasfin Alif100% (3)
- Camgfr V2: A New Model For Estimating The Glomerular Filtration Rate From Standardized or Non-Standardized Creatinine in Patients With CancerDocument10 pagesCamgfr V2: A New Model For Estimating The Glomerular Filtration Rate From Standardized or Non-Standardized Creatinine in Patients With CancerMaria Jose Gonzalez FarrisNo ratings yet
- AinsworthDocument9 pagesAinsworthJesse Helmut Hansen-BartelNo ratings yet
- Bosl 1988Document8 pagesBosl 1988Bruno AlanNo ratings yet
- 8235.full AACRDocument9 pages8235.full AACRMohammed Khair BashirNo ratings yet
- 1 s2.0 S0302283818300198 MainDocument7 pages1 s2.0 S0302283818300198 MainM Rizqi FiryalNo ratings yet
- Drug Dosing and Estimates of Kidney Function: Michael P Bosomworth and Jonathan AT SandoeDocument3 pagesDrug Dosing and Estimates of Kidney Function: Michael P Bosomworth and Jonathan AT SandoeJesse Helmut Hansen-BartelNo ratings yet
- CKD - Drug DosingDocument7 pagesCKD - Drug DosingRafaelNo ratings yet
- NGS de Panel para CCR - JCO 2015 - Costo-EfectividadDocument12 pagesNGS de Panel para CCR - JCO 2015 - Costo-EfectividadSebas Barrionuevo VediaNo ratings yet
- Population Pharmacokinetic Comparison and Pharmacodynamic Breakpoints of Ceftazidime in Cystic Fibrosis Patients and Healthy VolunteersDocument8 pagesPopulation Pharmacokinetic Comparison and Pharmacodynamic Breakpoints of Ceftazidime in Cystic Fibrosis Patients and Healthy Volunteershailemicael mesfinNo ratings yet
- Jco 2016 71 7397Document9 pagesJco 2016 71 7397brasilianaraNo ratings yet
- Novel Diagnostic and Predictive Biomarkers in Pancreatic AdenocarcinomaDocument14 pagesNovel Diagnostic and Predictive Biomarkers in Pancreatic AdenocarcinomaChavdarNo ratings yet
- Overestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementDocument7 pagesOverestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementJesse Helmut Hansen-BartelNo ratings yet
- Cu Line 2007Document8 pagesCu Line 2007Bruno AlanNo ratings yet
- Prognostic Value of C Reactive Protein - AlbuminDocument8 pagesPrognostic Value of C Reactive Protein - AlbuminfernandallmagalhaesNo ratings yet
- Shi Et AlDocument7 pagesShi Et AlK. O.No ratings yet
- A Retrospective Analysis of Magnetic Resonance Cholangiopancreatography Investigating Gallstones in A Contemporary Surgical SettingDocument6 pagesA Retrospective Analysis of Magnetic Resonance Cholangiopancreatography Investigating Gallstones in A Contemporary Surgical SettingRupak GhimireNo ratings yet
- Estimating Glomerular Filtration Rate From Serum Creatinine and Cystatin CDocument10 pagesEstimating Glomerular Filtration Rate From Serum Creatinine and Cystatin CIsyfaun NisaNo ratings yet
- Fórmulas para El Cálculo de Filtración GlomerularDocument7 pagesFórmulas para El Cálculo de Filtración GlomerularNoel Saúl Argüello SánchezNo ratings yet
- 1 s2.0 S245210942100097X MainDocument7 pages1 s2.0 S245210942100097X MainhidayatullahhaqyaarNo ratings yet
- CRP 2 PDFDocument8 pagesCRP 2 PDFAdarsiya JayakumarNo ratings yet
- Does Obesity Impact Lymph Node Retrieval in Colon CancerDocument5 pagesDoes Obesity Impact Lymph Node Retrieval in Colon Cancersee yinNo ratings yet
- Jcav 07 P 1701Document10 pagesJcav 07 P 1701leehongkaiNo ratings yet
- Treatment of Advanced or Recurrent Cervical Cancer With Cisplatin or Cisplatin Containing Regimens: A Cost Effective AnalysisDocument5 pagesTreatment of Advanced or Recurrent Cervical Cancer With Cisplatin or Cisplatin Containing Regimens: A Cost Effective Analysisyahya restiNo ratings yet
- The Role of FDG-PET Scans in Patients With Lymphoma: Review in Translational HematologyDocument11 pagesThe Role of FDG-PET Scans in Patients With Lymphoma: Review in Translational HematologyPunam SinhaNo ratings yet
- Pros TataDocument8 pagesPros TataMartin ElenaNo ratings yet
- PIIS1548559517301738Document7 pagesPIIS1548559517301738Joseph BoatengNo ratings yet
- The Role of Hypofractionated Radiotherapy in ProstDocument10 pagesThe Role of Hypofractionated Radiotherapy in ProstАнастасия АнохинаNo ratings yet
- Qi 2022Document12 pagesQi 2022Jonathan Billy ChristianNo ratings yet
- Clinical Laboratory Analysis - 2012 - Hashad - Free Circulating Tumor DNA As A Diagnostic Marker For Breast CancerDocument6 pagesClinical Laboratory Analysis - 2012 - Hashad - Free Circulating Tumor DNA As A Diagnostic Marker For Breast Cancerfaraz.mirza1No ratings yet
- Beriwal 2006Document5 pagesBeriwal 2006Bruno MendesNo ratings yet
- 10 1016@j Critrevonc 2020 102962Document16 pages10 1016@j Critrevonc 2020 102962bouh aichetouNo ratings yet
- 10 1200@jco 2001 19 6 1629Document12 pages10 1200@jco 2001 19 6 1629Bruno AlanNo ratings yet
- Pooled Rates of Adenoma Detection by ColonosDocument29 pagesPooled Rates of Adenoma Detection by ColonoscarolinaNo ratings yet
- CreatinineDocument7 pagesCreatinineLintang SuroyaNo ratings yet
- 1 s2.0 S0167814016000736 MainDocument7 pages1 s2.0 S0167814016000736 MainOkky HusainNo ratings yet
- CMW 051Document4 pagesCMW 051Laila Kurnia PramonoNo ratings yet
- New Creatinine-And Cystatin C-Based Equations To Estimate GFR Without RaceDocument13 pagesNew Creatinine-And Cystatin C-Based Equations To Estimate GFR Without RaceAlizaPinkyNo ratings yet
- Kenapa Pakai Formula SendiriDocument11 pagesKenapa Pakai Formula SendiriYoan RahmahNo ratings yet
- EeDocument8 pagesEeEstiPramestiningtyasNo ratings yet
- Ournal of Linical Ncology: PurposeDocument7 pagesOurnal of Linical Ncology: PurposeIvor Wiguna Hartanto WilopoNo ratings yet
- Clinical 88 (8620 CorrectionsDocument12 pagesClinical 88 (8620 CorrectionsLiv IuNo ratings yet
- Renal PhysiologyDocument7 pagesRenal PhysiologyLucas TheotonioNo ratings yet
- Role of Carbohydrate Antigen (Ca19-9) and Carcinoembryonic Antigen (Cea) As A Prognostic Factors in Pancreatic CarcinomaDocument6 pagesRole of Carbohydrate Antigen (Ca19-9) and Carcinoembryonic Antigen (Cea) As A Prognostic Factors in Pancreatic CarcinomaIJAR JOURNALNo ratings yet
- Aspirin and Colorectal DiagnosisDocument7 pagesAspirin and Colorectal DiagnosisErnesto PiconNo ratings yet
- ESR Vs CRPDocument6 pagesESR Vs CRPMuhammad Imran MirzaNo ratings yet
- ANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFDocument8 pagesANZ Journal of Surgery - 2021 - Yang - Outcomes of Patients With Metastatic Cutaneous Squamous Cell Carcinoma To The Axilla PDFRong LiuNo ratings yet
- Paper 2 Cancer DicoveryDocument18 pagesPaper 2 Cancer DicoverySuraj ShahNo ratings yet
- Kansal 2018Document1 pageKansal 2018Sheena Mae MansinadesNo ratings yet
- Kondagunta 2005Document5 pagesKondagunta 2005Bruno AlanNo ratings yet
- MainDocument8 pagesMainIoana CucuNo ratings yet
- Damit 2022 (KRAS)Document10 pagesDamit 2022 (KRAS)Healthcare Pro LearningNo ratings yet
- Cholong It As 2016Document2 pagesCholong It As 2016arieftamaNo ratings yet
- Kolagocarsinoma PDFDocument7 pagesKolagocarsinoma PDFBerlyan RuslanNo ratings yet
- Circulating Endothelial Cells and Other Angiogenesis Factors in Pancreatic Carcinoma Patients Receiving Gemcitabine ChemotherapyDocument10 pagesCirculating Endothelial Cells and Other Angiogenesis Factors in Pancreatic Carcinoma Patients Receiving Gemcitabine ChemotherapyftwNo ratings yet
- Hand RefractometerDocument5 pagesHand RefractometerAntigona2001No ratings yet
- Jeffrey L Carson Restrictive or Liberal TransfusionDocument11 pagesJeffrey L Carson Restrictive or Liberal Transfusionmiguel aghelNo ratings yet
- Articulo de HistologiaDocument6 pagesArticulo de HistologiaalexbowwNo ratings yet
- Faecal Occult Blood Screening Reduced The Incidence of Colorectal CancerDocument1 pageFaecal Occult Blood Screening Reduced The Incidence of Colorectal CancerAgus PraktyasaNo ratings yet
- A Review of The Role of Carcinoembryonic Antigen IDocument12 pagesA Review of The Role of Carcinoembryonic Antigen IMarcellia AngelinaNo ratings yet
- Facta About Pediatric-Nasopharyngeal-CarcinomaDocument8 pagesFacta About Pediatric-Nasopharyngeal-CarcinomaJesse Helmut Hansen-BartelNo ratings yet
- Results of Proton ReirradiationDocument9 pagesResults of Proton ReirradiationJesse Helmut Hansen-BartelNo ratings yet
- Comparative Treatment Planning Study of Photons and ProtonsDocument15 pagesComparative Treatment Planning Study of Photons and ProtonsJesse Helmut Hansen-BartelNo ratings yet
- Pediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsDocument5 pagesPediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsJesse Helmut Hansen-BartelNo ratings yet
- JZareh Coarctation Aorta Case PresDocument13 pagesJZareh Coarctation Aorta Case PresJesse Helmut Hansen-BartelNo ratings yet
- SVC SyndromeDocument17 pagesSVC SyndromeJesse Helmut Hansen-BartelNo ratings yet
- Paediatric Trauma - DR Nicole WilliamsDocument36 pagesPaediatric Trauma - DR Nicole WilliamsJesse Helmut Hansen-BartelNo ratings yet
- Update in Inflammatory Bowel Disease: Graham MorrisonDocument6 pagesUpdate in Inflammatory Bowel Disease: Graham MorrisonJesse Helmut Hansen-BartelNo ratings yet
- Gestational Alloimmune Liver Disease: Ethan TangDocument14 pagesGestational Alloimmune Liver Disease: Ethan TangJesse Helmut Hansen-BartelNo ratings yet
- AinsworthDocument9 pagesAinsworthJesse Helmut Hansen-BartelNo ratings yet
- Carboplatin Dosing 2nd Draft DrLinkDocument4 pagesCarboplatin Dosing 2nd Draft DrLinkJesse Helmut Hansen-BartelNo ratings yet
- Filamin A Mutations: Jesse Hansen-BartelDocument8 pagesFilamin A Mutations: Jesse Hansen-BartelJesse Helmut Hansen-BartelNo ratings yet
- Mar FansDocument14 pagesMar FansJesse Helmut Hansen-BartelNo ratings yet
- Overestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementDocument7 pagesOverestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementJesse Helmut Hansen-BartelNo ratings yet
- Prospective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaDocument8 pagesProspective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaJesse Helmut Hansen-BartelNo ratings yet
- Should We Continue To Use The Cockcroft-Gault Formula?: MinireviewDocument15 pagesShould We Continue To Use The Cockcroft-Gault Formula?: MinireviewJesse Helmut Hansen-BartelNo ratings yet
- Validity of Prediction Models: When Is A Model Clinically Useful?Document20 pagesValidity of Prediction Models: When Is A Model Clinically Useful?Jesse Helmut Hansen-BartelNo ratings yet
- Ekhart2009 Article CarboplatinDosingInOverweightADocument8 pagesEkhart2009 Article CarboplatinDosingInOverweightAJesse Helmut Hansen-Bartel100% (1)
- Heart Failure Clinical Presentation PathwayDocument1 pageHeart Failure Clinical Presentation PathwayJesse Helmut Hansen-BartelNo ratings yet
- Study 3Document12 pagesStudy 3Jesse Helmut Hansen-BartelNo ratings yet
- How To Adjust Drug Doses in Chronic Kidney DiseaseDocument5 pagesHow To Adjust Drug Doses in Chronic Kidney DiseaseJesse Helmut Hansen-BartelNo ratings yet
- Chinkenl 2014 PHDDocument227 pagesChinkenl 2014 PHDJesse Helmut Hansen-BartelNo ratings yet
- Bsa 2Document4 pagesBsa 2Jesse Helmut Hansen-BartelNo ratings yet
- Study 1Document9 pagesStudy 1Jesse Helmut Hansen-BartelNo ratings yet
- For The Clinician: Estimation of Kidney Function in OncologyDocument9 pagesFor The Clinician: Estimation of Kidney Function in OncologyJesse Helmut Hansen-BartelNo ratings yet
- The Investigation of Wound Healing DisordersDocument15 pagesThe Investigation of Wound Healing DisordersRadulescu IonelaNo ratings yet
- Usg Abdomen Pelvis MaleDocument2 pagesUsg Abdomen Pelvis MaleBhaktivedanta HospitalNo ratings yet
- Blood Pressure Regulation - SlidesDocument35 pagesBlood Pressure Regulation - Slidesمحمد السنجلاويNo ratings yet
- Excretion in Humans Igcse BiologyDocument26 pagesExcretion in Humans Igcse BiologyThe PassionNo ratings yet
- ICSE Sample Papers For Class 7 Biology Part 1 (2023-24)Document9 pagesICSE Sample Papers For Class 7 Biology Part 1 (2023-24)Dr. M. PrinceNo ratings yet
- Diuretics IDocument17 pagesDiuretics Iأمجد محمدNo ratings yet
- CPSP Demo Mcqs - 2022Document24 pagesCPSP Demo Mcqs - 2022Farhan AfzalNo ratings yet
- RENAL Nephrometry Scoring System: The Radiologist's PerspectiveDocument5 pagesRENAL Nephrometry Scoring System: The Radiologist's PerspectiveGaltieri OtavioNo ratings yet
- Exercise 9 Diet RX: 2000 Kcal CHO-325G Protein - 75G FATS - 44.4GDocument8 pagesExercise 9 Diet RX: 2000 Kcal CHO-325G Protein - 75G FATS - 44.4Gjho piangNo ratings yet
- Kidney and Liver FunctionDocument6 pagesKidney and Liver FunctionAhmad Ripani Musyaffa AhdanLabNo ratings yet
- Kidney Food RecipesDocument11 pagesKidney Food RecipesLouie Cedrick Camposano TriaNo ratings yet
- Pharmacokinetics of Clozapine and Its Metabolites in Psychiatric Patients: Plasma Protein Binding and Renal ClearanceDocument7 pagesPharmacokinetics of Clozapine and Its Metabolites in Psychiatric Patients: Plasma Protein Binding and Renal ClearancegowaryNo ratings yet
- Renal Effects of NSAIDDocument8 pagesRenal Effects of NSAIDtaner_soysurenNo ratings yet
- Anatomy and Physiology Module 2Document16 pagesAnatomy and Physiology Module 2JayR MendonesNo ratings yet
- ASN - Phenotype and Outcomes of Acute Kidney Injury Associated With COVID-19 in Urban New OrleansDocument1 pageASN - Phenotype and Outcomes of Acute Kidney Injury Associated With COVID-19 in Urban New OrleansCésar Hernández-ArroyoNo ratings yet
- Dr. Erlieza Roosdhania, SP - PD (CKD)Document38 pagesDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNo ratings yet
- Drug StudyDocument3 pagesDrug StudyKristine Faith AzcuetaNo ratings yet
- Doppler Ultrasound of The KidneysDocument23 pagesDoppler Ultrasound of The KidneysivoklarinNo ratings yet
- Potter Syndrome: A Case Study: August 2017Document6 pagesPotter Syndrome: A Case Study: August 2017rmysdsNo ratings yet
- Biology O Level 5090 SylllabusDocument35 pagesBiology O Level 5090 SylllabusBalakrishnan MarappanNo ratings yet
- Renal Function TestsDocument31 pagesRenal Function TestsPhysiology by Dr RaghuveerNo ratings yet
- Pex 09 01Document5 pagesPex 09 01Gerardien Elham AfifahNo ratings yet
- Blood Pressure in Early Autosomal Dominant Polycystic Kidney DiseaseDocument5 pagesBlood Pressure in Early Autosomal Dominant Polycystic Kidney DiseaseNancy MolinaNo ratings yet
- Urinalysis Practice QuizDocument4 pagesUrinalysis Practice QuizGrace GasconNo ratings yet
- Ion Transport, Osmoregulation, and Acid Base BalanceDocument54 pagesIon Transport, Osmoregulation, and Acid Base Balancefikriafis100% (1)
- Sulfonamides: (Veterinary-Systemic)Document17 pagesSulfonamides: (Veterinary-Systemic)Ursula HilleNo ratings yet
- Unit - V Chapter-22. Excretory Products and Their EliminationDocument15 pagesUnit - V Chapter-22. Excretory Products and Their EliminationBattuJayakrishnaNo ratings yet
- Fenofibrate-Associated Nephrotoxicity: A Review of Current EvidenceDocument8 pagesFenofibrate-Associated Nephrotoxicity: A Review of Current EvidencefevianaNo ratings yet