Download as pdf or txt
You might also like
- CC1 CC3Document26 pagesCC1 CC3pikachuNo ratings yet
- Ekhart2009 Article CarboplatinDosingInOverweightADocument8 pagesEkhart2009 Article CarboplatinDosingInOverweightAJesse Helmut Hansen-Bartel100% (1)
- Standardization of Chemotherapy and Individual Dosing of Platinum CompoundsDocument6 pagesStandardization of Chemotherapy and Individual Dosing of Platinum CompoundsJesse Helmut Hansen-BartelNo ratings yet
- Appendix 5 Calculation of Estimated Creatinine Clearance (CRCL)Document4 pagesAppendix 5 Calculation of Estimated Creatinine Clearance (CRCL)Erin FlowersNo ratings yet
- 10-Valproic AcidDocument49 pages10-Valproic AcidAli AmerNo ratings yet
- Hartmann 2003Document13 pagesHartmann 2003David Felipe Rojas DiazNo ratings yet
- Carboplatin DosingDocument3 pagesCarboplatin Dosinggentleman4891No ratings yet
- AinsworthDocument9 pagesAinsworthJesse Helmut Hansen-BartelNo ratings yet
- Contoh PresentasiDocument27 pagesContoh PresentasiNisadiyah Faridatus ShahihNo ratings yet
- CANT3 Onco-Nephrology - Core Curriculum 2015Document15 pagesCANT3 Onco-Nephrology - Core Curriculum 2015alam25No ratings yet
- Week 6 Facilitator Copy Week 06 Renal Failure PDFDocument7 pagesWeek 6 Facilitator Copy Week 06 Renal Failure PDFoxyc0n999No ratings yet
- ch3 2019 PDFDocument15 pagesch3 2019 PDFMohammed AbdNo ratings yet
- Appendix B PDFDocument2 pagesAppendix B PDFYunistya Dwi CahyaniNo ratings yet
- Study 1Document9 pagesStudy 1Jesse Helmut Hansen-BartelNo ratings yet
- CLC 4960230910Document7 pagesCLC 4960230910walnut21No ratings yet
- Assessment of Elevated CreatinineDocument10 pagesAssessment of Elevated CreatinineSheryl Ann PedinesNo ratings yet
- University of Duhok College of Science Department of Biology Second StageDocument26 pagesUniversity of Duhok College of Science Department of Biology Second StageSadeq PeeroNo ratings yet
- Prospective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaDocument8 pagesProspective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaJesse Helmut Hansen-BartelNo ratings yet
- 0002-9645-Ajvr 65 11 1502Document6 pages0002-9645-Ajvr 65 11 1502Ioana SanduNo ratings yet
- 1.1. Adv. Biopharma.-A-Dose Adjustment in Renal & Hepatic Failure - by M.firoz KhanDocument38 pages1.1. Adv. Biopharma.-A-Dose Adjustment in Renal & Hepatic Failure - by M.firoz KhanRaju NiraulaNo ratings yet
- Review: Platinum Neurotoxicity PharmacogeneticsDocument8 pagesReview: Platinum Neurotoxicity PharmacogeneticsAndreea TudurachiNo ratings yet
- Pharmacology of OxaliplatinDocument16 pagesPharmacology of OxaliplatinAliza JafriNo ratings yet
- Clozapina 3Document16 pagesClozapina 3Robert MovileanuNo ratings yet
- Vita B12 ElevadaDocument8 pagesVita B12 ElevadamaryNo ratings yet
- Colistin Dosing in Continuous Renal Replacement TherapyDocument6 pagesColistin Dosing in Continuous Renal Replacement Therapykade silabanNo ratings yet
- Lec - No.12 (Carbamazipine)Document13 pagesLec - No.12 (Carbamazipine)phd0780No ratings yet
- Biochemistry Acute Fatty Liver in Pregnancy Final PPT 1Document21 pagesBiochemistry Acute Fatty Liver in Pregnancy Final PPT 1Gracia Dela CruzNo ratings yet
- Phase I Studies With Carboplatin at The Royal Marsden HospitalDocument7 pagesPhase I Studies With Carboplatin at The Royal Marsden HospitalArun GargNo ratings yet
- Cholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfDocument30 pagesCholesterol, Triglycerides, and Associated Lipoproteins - Clinical Methods - NCBI BookshelfNeha MasarkarNo ratings yet
- Cockcroft & Gault V4 4.13Document2 pagesCockcroft & Gault V4 4.13Audrey BridgesNo ratings yet
- CPT 109 1224Document8 pagesCPT 109 1224RobsonNo ratings yet
- Proprotein Convertase Subtilisin Kexin 9 InhibitorsDocument16 pagesProprotein Convertase Subtilisin Kexin 9 InhibitorsTony Miguel Saba SabaNo ratings yet
- Estimating Renal Function For Drug Dosing Decisions: Mini-ReviewDocument8 pagesEstimating Renal Function For Drug Dosing Decisions: Mini-ReviewnegarayeniNo ratings yet
- Hidrolisis of CapecitabineDocument6 pagesHidrolisis of CapecitabineJUAN JESÚSNo ratings yet
- HDL - C Methods: Preparative UltracentrifugationDocument13 pagesHDL - C Methods: Preparative UltracentrifugationanggaririnNo ratings yet
- Captopril: Determination in Blood and Pharmacokinetics After Single Oral DoseDocument6 pagesCaptopril: Determination in Blood and Pharmacokinetics After Single Oral DoseKhintan Risky FadhilaNo ratings yet
- The Warburg EffectDocument10 pagesThe Warburg EffectLauris TorresNo ratings yet
- Metabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsDocument33 pagesMetabolism, Excretion, and Pharmacokinetics of Selumetinib, An MEK1/2 Inhibitor, in Healthy Adult Male SubjectsAndi wahyuniNo ratings yet
- CreatinineDocument39 pagesCreatinineMustafa Khandgawi100% (1)
- Augmented Renal Clearance and How To AugmentDocument12 pagesAugmented Renal Clearance and How To Augmentlocal5.fsgNo ratings yet
- 1121-26 1.10 Kua Voon Fong PDFDocument6 pages1121-26 1.10 Kua Voon Fong PDFfaidgustisyarifNo ratings yet
- Overestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementDocument7 pagesOverestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementJesse Helmut Hansen-BartelNo ratings yet
- Jurnal MaglitinideDocument7 pagesJurnal MaglitinideWanda Novia P SNo ratings yet
- Jurnal Tugas BudianaDocument3 pagesJurnal Tugas BudianazizahNo ratings yet
- Indications For Initiation of DialysisDocument11 pagesIndications For Initiation of DialysisMilton BenevidesNo ratings yet
- Coreg: (Carvedilol) TabletsDocument19 pagesCoreg: (Carvedilol) TabletsThejeswarNo ratings yet
- Measurement of Renal Function in PracticeDocument5 pagesMeasurement of Renal Function in PracticeVijeyachandhar DorairajNo ratings yet
- LEUKERAN-chlorambucil Tablet, Film Coated Waylis Therapeutics LLCDocument12 pagesLEUKERAN-chlorambucil Tablet, Film Coated Waylis Therapeutics LLCAkoro SeraishiNo ratings yet
- Drug Use in Renal and Hepatic Disorders.: Chapter-VDocument30 pagesDrug Use in Renal and Hepatic Disorders.: Chapter-VBandameedi RamuNo ratings yet
- Effect of Hepatic and Renal Impairment On PharmacokineticDocument46 pagesEffect of Hepatic and Renal Impairment On PharmacokineticPURVI NEEMANo ratings yet
- Effectiveness and Safety of Low-Dose Pravastatin and Squalene, Alone and in Combination, in Elderly Patients With HypercholesterolemiaDocument6 pagesEffectiveness and Safety of Low-Dose Pravastatin and Squalene, Alone and in Combination, in Elderly Patients With HypercholesterolemiaeduardochocincoNo ratings yet
- GlucoseDocument5 pagesGlucosebagsouravNo ratings yet
- HW3 PharmacologyDocument8 pagesHW3 PharmacologyMICHAEL GABRIEL JIMENEZNo ratings yet
- CreatinineDocument5 pagesCreatininefathiyyahnurulNo ratings yet
- CKD - Drug DosingDocument7 pagesCKD - Drug DosingRafaelNo ratings yet
- Eligibility Criteria: Previous Sectionnext SectionDocument6 pagesEligibility Criteria: Previous Sectionnext Sectionbettzy21No ratings yet
- Formulation and Evaluation of Dsatinib TabletsDocument9 pagesFormulation and Evaluation of Dsatinib TabletsSyed Abdul Haleem AkmalNo ratings yet
- 2708Document6 pages2708ArjunaPamungkasNo ratings yet
- Lipoic Acid Inhibits Cell Proliferation of Tumor Cells in Vitro and in VivoDocument11 pagesLipoic Acid Inhibits Cell Proliferation of Tumor Cells in Vitro and in VivosweetohmNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- Renal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysFrom EverandRenal Pharmacotherapy: Dosage Adjustment of Medications Eliminated by the KidneysNo ratings yet
- Results of Proton ReirradiationDocument9 pagesResults of Proton ReirradiationJesse Helmut Hansen-BartelNo ratings yet
- Pediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsDocument5 pagesPediatric Nasopharyngeal Carcinoma Treated With Proton Beam Therapy Two Case ReportsJesse Helmut Hansen-BartelNo ratings yet
- Comparative Treatment Planning Study of Photons and ProtonsDocument15 pagesComparative Treatment Planning Study of Photons and ProtonsJesse Helmut Hansen-BartelNo ratings yet
- Facta About Pediatric-Nasopharyngeal-CarcinomaDocument8 pagesFacta About Pediatric-Nasopharyngeal-CarcinomaJesse Helmut Hansen-BartelNo ratings yet
- Update in Inflammatory Bowel Disease: Graham MorrisonDocument6 pagesUpdate in Inflammatory Bowel Disease: Graham MorrisonJesse Helmut Hansen-BartelNo ratings yet
- SVC SyndromeDocument17 pagesSVC SyndromeJesse Helmut Hansen-BartelNo ratings yet
- Mar FansDocument14 pagesMar FansJesse Helmut Hansen-BartelNo ratings yet
- Paediatric Trauma - DR Nicole WilliamsDocument36 pagesPaediatric Trauma - DR Nicole WilliamsJesse Helmut Hansen-BartelNo ratings yet
- Gestational Alloimmune Liver Disease: Ethan TangDocument14 pagesGestational Alloimmune Liver Disease: Ethan TangJesse Helmut Hansen-BartelNo ratings yet
- JZareh Coarctation Aorta Case PresDocument13 pagesJZareh Coarctation Aorta Case PresJesse Helmut Hansen-BartelNo ratings yet
- Filamin A Mutations: Jesse Hansen-BartelDocument8 pagesFilamin A Mutations: Jesse Hansen-BartelJesse Helmut Hansen-BartelNo ratings yet
- Chinkenl 2014 PHDDocument227 pagesChinkenl 2014 PHDJesse Helmut Hansen-BartelNo ratings yet
- Study 3Document12 pagesStudy 3Jesse Helmut Hansen-BartelNo ratings yet
- Prospective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaDocument8 pagesProspective Evaluation of Carboplatin AUC Dosing in Patients With A BMI 27 or CachexiaJesse Helmut Hansen-BartelNo ratings yet
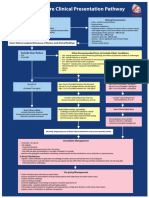
- Heart Failure Clinical Presentation PathwayDocument1 pageHeart Failure Clinical Presentation PathwayJesse Helmut Hansen-BartelNo ratings yet
- AinsworthDocument9 pagesAinsworthJesse Helmut Hansen-BartelNo ratings yet
- Should We Continue To Use The Cockcroft-Gault Formula?: MinireviewDocument15 pagesShould We Continue To Use The Cockcroft-Gault Formula?: MinireviewJesse Helmut Hansen-BartelNo ratings yet
- Study 4Document10 pagesStudy 4Jesse Helmut Hansen-BartelNo ratings yet
- Validity of Prediction Models: When Is A Model Clinically Useful?Document20 pagesValidity of Prediction Models: When Is A Model Clinically Useful?Jesse Helmut Hansen-BartelNo ratings yet
- Study 1Document9 pagesStudy 1Jesse Helmut Hansen-BartelNo ratings yet
- Bsa 2Document4 pagesBsa 2Jesse Helmut Hansen-BartelNo ratings yet
- Overestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementDocument7 pagesOverestimation of Carboplatin Doses Is Avoided by Radionuclide GFR MeasurementJesse Helmut Hansen-BartelNo ratings yet
- Ekhart2009 Article CarboplatinDosingInOverweightADocument8 pagesEkhart2009 Article CarboplatinDosingInOverweightAJesse Helmut Hansen-Bartel100% (1)
- How To Adjust Drug Doses in Chronic Kidney DiseaseDocument5 pagesHow To Adjust Drug Doses in Chronic Kidney DiseaseJesse Helmut Hansen-BartelNo ratings yet
- For The Clinician: Estimation of Kidney Function in OncologyDocument9 pagesFor The Clinician: Estimation of Kidney Function in OncologyJesse Helmut Hansen-BartelNo ratings yet
- Gabriel Rodriguez Forensic Pathology ReportDocument4 pagesGabriel Rodriguez Forensic Pathology Reportapi-268624787No ratings yet
- Renal Function Test DiscussionDocument5 pagesRenal Function Test DiscussionMard SumalpongNo ratings yet
- Pancreatitis, Acute: Clinical PresentationDocument26 pagesPancreatitis, Acute: Clinical Presentationapi-19641337No ratings yet
- Ifcc 2011 Respons910 LowDocument1 pageIfcc 2011 Respons910 LowChethan s mNo ratings yet
- Nephrology For Medical StudentsDocument220 pagesNephrology For Medical StudentsAndre Sante100% (3)
- Crej2: Alkaline PHDocument7 pagesCrej2: Alkaline PHMadalina Cioroiu-AndronescuNo ratings yet
- Basic Clinical Chemistry PDFDocument72 pagesBasic Clinical Chemistry PDFJacc jaccNo ratings yet
- Ascorbic Acid Interference in The Measurement of Serum BiochemicalDocument8 pagesAscorbic Acid Interference in The Measurement of Serum BiochemicalCt Nur HanisNo ratings yet
- Laboratory Tests To Evaluate Fluid StatusDocument52 pagesLaboratory Tests To Evaluate Fluid StatusLester Exconde Alfonso0% (1)
- Wet Practical Frcpath2014Document7 pagesWet Practical Frcpath2014monday125No ratings yet
- Medicomama's Biochemistry QBDocument28 pagesMedicomama's Biochemistry QBbhageerathavmc98No ratings yet
- CCDocument23 pagesCCMarvin SimbulanNo ratings yet
- Product Monograph - Zoledronic Acid For Injection ConcentrateDocument58 pagesProduct Monograph - Zoledronic Acid For Injection ConcentrateMisgi Candra DasaNo ratings yet
- Insert Kit Kimia KlinikDocument1 pageInsert Kit Kimia Klinikdian saleh100% (1)
- Effectivity of Lumbrokinase in Reducing Proteinuria On Patients With Diabetic Kidney DiseaseDocument11 pagesEffectivity of Lumbrokinase in Reducing Proteinuria On Patients With Diabetic Kidney Diseasevedora angeliaNo ratings yet
- Rabdomiolisis EnfoqueDocument8 pagesRabdomiolisis EnfoqueLeidy Nayerli Garcia RodriguezNo ratings yet
- An Approach To CKD - FinalDocument98 pagesAn Approach To CKD - FinalDr Harihar KhanalNo ratings yet
- 11-124-1-PB (1) Vanc Neph PDFDocument7 pages11-124-1-PB (1) Vanc Neph PDFTheo PentoneNo ratings yet
- The Clinical Biochemistry of Kidney Functions: 2019 DR Boldizsár CZÉHDocument46 pagesThe Clinical Biochemistry of Kidney Functions: 2019 DR Boldizsár CZÉHJACOB FRANCISNo ratings yet
- Fundamentals of Pharmcology: Nursing Facts in BriefDocument4 pagesFundamentals of Pharmcology: Nursing Facts in Briefanne009No ratings yet
- VLD 411Document66 pagesVLD 411बनकर परिवाराचा लाडका गोट्याNo ratings yet
- SAALT2W Protocol 2Document8 pagesSAALT2W Protocol 2Getwel Clinic And HospitalNo ratings yet
- Questions About KidneysDocument30 pagesQuestions About KidneysKristine Mae AbrasaldoNo ratings yet
- Original Articles_ Comparison of Urinary Albumin-Creatinine Ratio and Albumin Excretion Rate in the Diabetes Control and Complications Trial_Epidemiology of Diabetes Interventions and Complications StudyDocument16 pagesOriginal Articles_ Comparison of Urinary Albumin-Creatinine Ratio and Albumin Excretion Rate in the Diabetes Control and Complications Trial_Epidemiology of Diabetes Interventions and Complications StudyM Dwi SuprayogiNo ratings yet
- CYSC2Document4 pagesCYSC2ARIF AHAMMED PNo ratings yet
- Chapter 15. Protein and Amino Acid MetabolismDocument42 pagesChapter 15. Protein and Amino Acid Metabolismrahul.kumar4504No ratings yet
- Chapter 7 - Biological VariationDocument16 pagesChapter 7 - Biological VariationChristian Cedrick OlmonNo ratings yet
- LOINC CodesDocument352 pagesLOINC CodesRajaRamNo ratings yet
- Fully Automated Lab Accurate Reports Reports Verified by PathologistDocument9 pagesFully Automated Lab Accurate Reports Reports Verified by PathologistJayshree BawaniyaNo ratings yet