Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- About Virgin Pussy URDUDocument7 pagesAbout Virgin Pussy URDUa0313660841166% (53)
- Complete Hydatidiform MoleDocument1 pageComplete Hydatidiform MoleWilliam BarreraNo ratings yet
- Form Pre Job MeetingDocument2 pagesForm Pre Job Meetingrian1099No ratings yet
- Nama Produk Per Rak Ethical 1Document74 pagesNama Produk Per Rak Ethical 1Akhmad “Billy Rafi” HambaliNo ratings yet
- Pricelist PT. DHS-KB PKLNGNDocument4 pagesPricelist PT. DHS-KB PKLNGNnur khasanahNo ratings yet
- The F Word-Feminism and Its DetractorsDocument46 pagesThe F Word-Feminism and Its DetractorsSibel UlusoyNo ratings yet
- Verbal Reasoning Tests Volume 2 DownloadDocument362 pagesVerbal Reasoning Tests Volume 2 DownloadAhmed FathyNo ratings yet
- Mini DramaDocument7 pagesMini DramaYuni AstutiNo ratings yet
- Eto General Catalogue 2013Document2 pagesEto General Catalogue 2013ophtho india incNo ratings yet
- PDF Spirituality in Nursing Standing On Holy Ground 6Th Edition Mary Elizabeth Obrien Ebook Full ChapterDocument53 pagesPDF Spirituality in Nursing Standing On Holy Ground 6Th Edition Mary Elizabeth Obrien Ebook Full Chaptercarl.jones252100% (1)
- Practice Guidelines For Telemental HealthDocument51 pagesPractice Guidelines For Telemental HealthNataanatiNo ratings yet
- 1.2 HSE Management System ManualDocument31 pages1.2 HSE Management System ManualkevinNo ratings yet
- Interrupted Time Series Analysis David Mcdowall Full ChapterDocument77 pagesInterrupted Time Series Analysis David Mcdowall Full Chapterdorene.baldwin751100% (7)
- A Qualitative Study: Campus Bullying in The Senior High SchoolDocument14 pagesA Qualitative Study: Campus Bullying in The Senior High SchoolHouston IbañezNo ratings yet
- Anterior Guidance: Group Function/canine Guidance. A Literature ReviewDocument4 pagesAnterior Guidance: Group Function/canine Guidance. A Literature ReviewAayushi Vaidya100% (1)
- Knowledge Series 8 - Mediclaim Insurance Policy With Oriental Insurance CompanyDocument8 pagesKnowledge Series 8 - Mediclaim Insurance Policy With Oriental Insurance CompanyRahul Rao MKNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaJessie NovaNo ratings yet
- Semen AnalysisDocument4 pagesSemen AnalysisCarlo AlvaradoNo ratings yet
- Intellectual Attributes of PersonalityDocument40 pagesIntellectual Attributes of PersonalitycedzmonderoNo ratings yet
- DR - 100e MobileDocument8 pagesDR - 100e MobileGlen CarvaloNo ratings yet
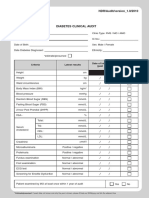
- Borang Diabetes Clinical AuditDocument2 pagesBorang Diabetes Clinical AuditHafizzah Mohd FirdausNo ratings yet
- Nutrition SurveyDocument18 pagesNutrition SurveyMogesNo ratings yet
- Topics For Reporting in NCM 116Document1 pageTopics For Reporting in NCM 116Sarmiento, Jovenal B.No ratings yet
- Ey e Commerce PharmacyDocument12 pagesEy e Commerce PharmacyAdi SudewaNo ratings yet
- Zambia v9 20190426 - 1230Document242 pagesZambia v9 20190426 - 1230Salim AbdulrahimNo ratings yet
- Learning Task 4Document3 pagesLearning Task 4Rz BorreroNo ratings yet
- Health and Safety Audit FormDocument2 pagesHealth and Safety Audit FormEngr Abdul Shakoor ShaikhNo ratings yet
- VA Emergency Care RulesDocument3 pagesVA Emergency Care RulesSunflower WilliamsNo ratings yet
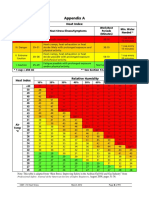
- Part I - 13 Heat Stress 8Document1 pagePart I - 13 Heat Stress 8SKH CultureNo ratings yet
- Nursing Care Plan-1idealDocument30 pagesNursing Care Plan-1idealSheila Mae PanisNo ratings yet