Download as pdf or txt
You might also like
- Kink Negotiation Worksheet: Step One: What Do I Want?Document1 pageKink Negotiation Worksheet: Step One: What Do I Want?Amber Horton100% (1)
- NUR168 Project 031822Document11 pagesNUR168 Project 031822Rebecca RathburnNo ratings yet
- Nursing School Entrance Exams: HESI A2 / NLN PAX-RN / PSB-RN / RNEE / TEASFrom EverandNursing School Entrance Exams: HESI A2 / NLN PAX-RN / PSB-RN / RNEE / TEASNo ratings yet
- Transcript Format BHMS Old 220110Document4 pagesTranscript Format BHMS Old 220110Rathin Dholakia100% (2)
- Practical Research 2 SummativeDocument5 pagesPractical Research 2 SummativeColeen Mae Saluib100% (5)
- Application Form: Send This Form ToDocument2 pagesApplication Form: Send This Form ToKlaudia KonyaNo ratings yet
- MedDocument4 pagesMedMohamed AbbasNo ratings yet
- Career Cruising - Physical TherapistDocument6 pagesCareer Cruising - Physical Therapistapi-355293530No ratings yet
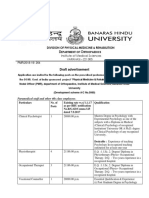
- Division OF Physical Medicine & Rehabilition: Draft AdvertisementDocument6 pagesDivision OF Physical Medicine & Rehabilition: Draft AdvertisementVeekeshGuptaNo ratings yet
- Learners Health Assessement FormDocument4 pagesLearners Health Assessement FormJAY-R MOLASENo ratings yet
- Senior Career Action Plan-Garrison Paige CareerDocument17 pagesSenior Career Action Plan-Garrison Paige Careerapi-510819871No ratings yet
- HSCP Telehealth Practice Examples 2021Document38 pagesHSCP Telehealth Practice Examples 2021AlinaNo ratings yet
- Glicken Hartnett Morisseau Interprofessional EducationDocument54 pagesGlicken Hartnett Morisseau Interprofessional EducationInges PSNo ratings yet
- List of Medical Professionals-SPADocument8 pagesList of Medical Professionals-SPANoemí GuzmartNo ratings yet
- Career Day AudDocument12 pagesCareer Day AudlNo ratings yet
- VSOB Application Form Tcm81 21876Document7 pagesVSOB Application Form Tcm81 21876J Fernand GasparNo ratings yet
- AudiologistDocument5 pagesAudiologistm afiq fahmiNo ratings yet
- Curriculum Vitae: Julie Ferlyn O. Acero, RNDocument3 pagesCurriculum Vitae: Julie Ferlyn O. Acero, RNKaren AceroNo ratings yet
- Past Simple or Present Perfect Which Is Appropriate For Diagnoses OETDocument1 pagePast Simple or Present Perfect Which Is Appropriate For Diagnoses OETRoxane PresbiteroNo ratings yet
- 1.4.a Prof Ramdan FOB IX - Genetics Counseling-Where Are WeDocument26 pages1.4.a Prof Ramdan FOB IX - Genetics Counseling-Where Are Wetepat rshsNo ratings yet
- OccupationDocument15 pagesOccupationapi-301581068No ratings yet
- OccupationDocument15 pagesOccupationapi-305727641No ratings yet
- Audiology and Speech PathologyDocument2 pagesAudiology and Speech PathologyErsya MusLih AnshoriNo ratings yet
- TgrgybhtDocument9 pagesTgrgybhtTECHNICAL SWAYAMNo ratings yet
- EJEP HRDP - OJT Application Form 1Document8 pagesEJEP HRDP - OJT Application Form 1Tagreed MeshrefNo ratings yet
- Health-10 Q4 WK3Document2 pagesHealth-10 Q4 WK3Gerald EscobalNo ratings yet
- VSO Application FormDocument7 pagesVSO Application Formapi-3807120100% (1)
- Mentor Mentee PROFORMADocument6 pagesMentor Mentee PROFORMAVivek LuckyNo ratings yet
- Hope Invitation Modified - March 2010Document1 pageHope Invitation Modified - March 2010Radhamani ArunNo ratings yet
- CurrryDocument18 pagesCurrryAkshay VasishtaNo ratings yet
- Adult Integrated Pre Procedure ScreeningDocument4 pagesAdult Integrated Pre Procedure ScreeningQRM CikarangNo ratings yet
- Audiology and Speech-Language Pathology: What Can I Do With This Major?Document3 pagesAudiology and Speech-Language Pathology: What Can I Do With This Major?So RimNo ratings yet
- Tuesday 9/15 Vocabulary Thursday 9/17 VocabularyDocument2 pagesTuesday 9/15 Vocabulary Thursday 9/17 VocabularyAshley SchmidtNo ratings yet
- World of Work Worksheet-1Document2 pagesWorld of Work Worksheet-1api-266685207No ratings yet
- DLD JCPSLP Vol 20 No 1Document52 pagesDLD JCPSLP Vol 20 No 1jadeNo ratings yet
- Recommendation FormsDocument1 pageRecommendation FormsRezi Sabutanan AmerilaNo ratings yet
- Recommendation FormsDocument1 pageRecommendation FormsRezi Sabutanan AmerilaNo ratings yet
- Quiz Medical Proffesionals Fernanda AguirreDocument1 pageQuiz Medical Proffesionals Fernanda AguirreFernanda AmigoNo ratings yet
- NEET PG Syllabus 2024 - Detailed Subject-Wise TopicsDocument70 pagesNEET PG Syllabus 2024 - Detailed Subject-Wise Topicsmayur TNo ratings yet
- Final Results: Fourth Year First Trial 2019-2020Document110 pagesFinal Results: Fourth Year First Trial 2019-2020Sami AzizNo ratings yet
- Community Medicine Pro FormaDocument21 pagesCommunity Medicine Pro FormaD.p RamakrishnaNo ratings yet
- Dental Jurisprudence Periodontics Endodontics: Ethics and Practice ManagementDocument2 pagesDental Jurisprudence Periodontics Endodontics: Ethics and Practice ManagementMariz PepitoNo ratings yet
- All Luc Three in One ProgramDocument29 pagesAll Luc Three in One Programজে.এস. কন্সট্রাকশনNo ratings yet
- Ahs PPP CMHDocument12 pagesAhs PPP CMHTariq ManzoorNo ratings yet
- Janet Scott: About MeDocument1 pageJanet Scott: About Meapi-518809610No ratings yet
- Health Care StackableDocument1 pageHealth Care Stackableapi-253276786No ratings yet
- Faculty of Medicine: Permohonan Semester I Sesi 2020 /2021Document14 pagesFaculty of Medicine: Permohonan Semester I Sesi 2020 /2021HiddemNo ratings yet
- BRO06242021004Document6 pagesBRO06242021004shunanlatheefNo ratings yet
- Doctor of Dental SurgeryDocument6 pagesDoctor of Dental SurgeryOthman A. MughniNo ratings yet
- Center For Health Sciences BrochureDocument4 pagesCenter For Health Sciences BrochureGraduate School USANo ratings yet
- Guidelines Faculty CompleteDocument11 pagesGuidelines Faculty CompleteNienuk KusumawatiNo ratings yet
- Voice Disorders in TeachersDocument8 pagesVoice Disorders in TeachersDomenica AvilaNo ratings yet
- Don Nguyendac - Resume 2Document2 pagesDon Nguyendac - Resume 2sandeep yadav (sakhat londa)No ratings yet
- A Papachilleas Dds Europass Curriculum VitaeDocument6 pagesA Papachilleas Dds Europass Curriculum VitaeNur IbrahimNo ratings yet
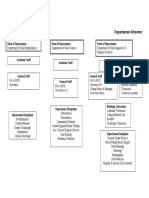
- Dental DepartmentDocument1 pageDental DepartmentBrian ShannyNo ratings yet
- Manual de Especialidades Medicas en InglesDocument117 pagesManual de Especialidades Medicas en InglesYobelkisNo ratings yet
- This Plan of Study Should Serve As A Guide, Along With Other Career Planning Materials, As You Continue Your Career Path. Courses Listed WithinDocument1 pageThis Plan of Study Should Serve As A Guide, Along With Other Career Planning Materials, As You Continue Your Career Path. Courses Listed WithinUr MomNo ratings yet
- Karir Dokter Di Ranah Pelayanan PrimerDocument17 pagesKarir Dokter Di Ranah Pelayanan PrimerSuyanto SuyantoNo ratings yet
- Professional CV Rasha Abu BakerDocument4 pagesProfessional CV Rasha Abu BakerHamed NazariNo ratings yet
- Fee Structure For Mds 2023 24Document2 pagesFee Structure For Mds 2023 24upma20ecNo ratings yet
- Ultra Flash CSFB 10dec2020Document15 pagesUltra Flash CSFB 10dec2020hamadashraf301No ratings yet
- CR DynamicCpich 08032021Document2 pagesCR DynamicCpich 08032021hamadashraf301No ratings yet
- ZTE UMTS UR15 Radio Connection Re-Establishment Feature GuideDocument56 pagesZTE UMTS UR15 Radio Connection Re-Establishment Feature Guidehamadashraf301100% (1)
- Adjusting The Sound: Adjust Various Sound SettingsDocument8 pagesAdjusting The Sound: Adjust Various Sound Settingshamadashraf301No ratings yet
- LTE Mobility LayeringDocument61 pagesLTE Mobility Layeringhamadashraf301No ratings yet
- Use of Spreading Factor 512 With UTRA FDDDocument4 pagesUse of Spreading Factor 512 With UTRA FDDhamadashraf301No ratings yet
- Csfallback 160728092728Document419 pagesCsfallback 160728092728hamadashraf301No ratings yet
- CoMP FeatureDocument111 pagesCoMP Featurehamadashraf301No ratings yet
- IRATDocument43 pagesIRAThamadashraf301No ratings yet
- The Use of Lemongrass As A Natural Glass CleanerDocument3 pagesThe Use of Lemongrass As A Natural Glass CleanerJc Charm-Vhil Arocena100% (1)
- 19 52 45 31 05 2018 Ms - 1774Document8 pages19 52 45 31 05 2018 Ms - 1774Kifah ZaidanNo ratings yet
- Prima 460 Sales en 1022Document6 pagesPrima 460 Sales en 1022antonios.medilonNo ratings yet
- Iron Deficiency and Congestive Heart FailureDocument3 pagesIron Deficiency and Congestive Heart FailureEnzoNo ratings yet
- IELTS 12 T5 Listening AnswerDocument1 pageIELTS 12 T5 Listening Answerphuonganhphmvu05No ratings yet
- The Probiotic PromiseDocument305 pagesThe Probiotic PromiseAmir addani100% (2)
- Jonnie Candito Strength-PowerDocument5 pagesJonnie Candito Strength-PowerRe BNo ratings yet
- Progresive Multiple Sclerosis Continuum 2022Document21 pagesProgresive Multiple Sclerosis Continuum 2022cuentoNo ratings yet
- UEC Workshop by Jane IreneDocument41 pagesUEC Workshop by Jane IrenePei ChengNo ratings yet
- Ojsadmin, Article 48Document6 pagesOjsadmin, Article 48Nilla Pramida IlyasNo ratings yet
- Lesson 1 R1 Homework Answer KeyDocument2 pagesLesson 1 R1 Homework Answer KeyПунцагноров Ц.No ratings yet
- Test-Taking Skills Booster: Summit Can Be Found in The Summit ActiveteachDocument10 pagesTest-Taking Skills Booster: Summit Can Be Found in The Summit ActiveteachBernoliNo ratings yet
- Epidemiology of Visual Impairment & BlindnessDocument17 pagesEpidemiology of Visual Impairment & BlindnessvaishnaviNo ratings yet
- MUCLecture 2022 32815285 PDFDocument15 pagesMUCLecture 2022 32815285 PDFobw 1408No ratings yet
- BSM - SOUTH - AFRICA - Brochure - 22Document26 pagesBSM - SOUTH - AFRICA - Brochure - 22Delta PayNo ratings yet
- The Story of Jerry and The Dr. ParrotDocument3 pagesThe Story of Jerry and The Dr. ParrotGrace BongabongNo ratings yet
- Separation Anxi-WPS OfficeDocument28 pagesSeparation Anxi-WPS Officedawit alemzewdNo ratings yet
- Management of Patients With Renal DisordersDocument29 pagesManagement of Patients With Renal DisordersokaciaNo ratings yet
- 2014.karimi Et Al. - Emotional Rescue - The Role of EmotionalDocument11 pages2014.karimi Et Al. - Emotional Rescue - The Role of EmotionalbomoyaNo ratings yet
- Aviation and healthcarervw-JRSM 2015Document10 pagesAviation and healthcarervw-JRSM 2015mnovemberNo ratings yet
- Air PollutionDocument19 pagesAir PollutionMika Hakimie100% (1)
- Prevalence and Characteristics of Women With Polycystic Ovary Syndrome in Bangladesh - A Narrative ReviewDocument10 pagesPrevalence and Characteristics of Women With Polycystic Ovary Syndrome in Bangladesh - A Narrative Reviewnanjiba.khanNo ratings yet
- Mbbs Admission 2022 Student StatusDocument122 pagesMbbs Admission 2022 Student StatusShreyasNo ratings yet
- Đề Thi HSG Số 1Document5 pagesĐề Thi HSG Số 1Trang NguyễnNo ratings yet
- Arc Flash Hazard Analysis Summary: The Objectives of This Chapter Are ToDocument11 pagesArc Flash Hazard Analysis Summary: The Objectives of This Chapter Are Tokartikay jhaNo ratings yet
- Potential of Cinnamon Cinnamomum Zeylanicum Powder and Lemongrass Cymbopogon Citratus Air Freshener and Fly RepellentDocument7 pagesPotential of Cinnamon Cinnamomum Zeylanicum Powder and Lemongrass Cymbopogon Citratus Air Freshener and Fly RepellentEdrian Cubon VillodresNo ratings yet
- Marketing Intermediaries in Channels of DistributiDocument5 pagesMarketing Intermediaries in Channels of DistributiLucia QuevedoNo ratings yet
- CLASS SHEET 21 Lyst9149 PDFDocument5 pagesCLASS SHEET 21 Lyst9149 PDFGireesh ParkerNo ratings yet