Download as docx, pdf, or txt
You might also like
- Strategic Considerations in Treatment Planning Deciding When To Treat, Extract, or Replace A Questionable Tooth PDFDocument12 pagesStrategic Considerations in Treatment Planning Deciding When To Treat, Extract, or Replace A Questionable Tooth PDFItzel Marquez100% (1)
- OSCE - Health PromotionDocument13 pagesOSCE - Health PromotionbabukanchaNo ratings yet
- Nursing Home Lesson PlanDocument13 pagesNursing Home Lesson Planapi-353466401100% (1)
- Multiple Myeloma Case StudyDocument42 pagesMultiple Myeloma Case StudyHope Serquiña100% (2)
- Cesarean Delivery Case Presentation ConceptualDocument57 pagesCesarean Delivery Case Presentation ConceptualHope Serquiña67% (3)
- Clinical Case PresentationDocument20 pagesClinical Case PresentationدرالجمانNo ratings yet
- Oral Care Conscious and Unconscious ClientDocument24 pagesOral Care Conscious and Unconscious ClientJojo JoestarNo ratings yet
- Oral Hygiene InstructionsDocument21 pagesOral Hygiene InstructionsmisdduaaNo ratings yet
- Oral Health: Steps To A Healthy MouthDocument12 pagesOral Health: Steps To A Healthy MouthAnonymous KDv8d0zNo ratings yet
- Pamantasan NG Lungsod NG MaynilaDocument15 pagesPamantasan NG Lungsod NG MaynilaAlex HollandNo ratings yet
- Careplanexample 073Document2 pagesCareplanexample 073Rena Jane B. DandanNo ratings yet
- Oral HygieneDocument9 pagesOral Hygienesuman guptaNo ratings yet
- Treatment Plan 3Document10 pagesTreatment Plan 3api-315001017No ratings yet
- Treatment Plan Assignment 2 Kylie Hill Kirkwood Community CollegeDocument7 pagesTreatment Plan Assignment 2 Kylie Hill Kirkwood Community Collegeapi-510470035No ratings yet
- Treatment Plan 1Document4 pagesTreatment Plan 1api-657970549No ratings yet
- Oral Care ProtocolDocument8 pagesOral Care ProtocolQonitaNurMiladiNo ratings yet
- Treatment Plan 1Document4 pagesTreatment Plan 1api-662638224No ratings yet
- Oral Health-WPS OfficeDocument34 pagesOral Health-WPS OfficeChief ArisaNo ratings yet
- Oral and Dental HealthDocument21 pagesOral and Dental HealthMaricor OnateNo ratings yet
- Oral Health 09Document20 pagesOral Health 09Mirza AryantoNo ratings yet
- Community Presentation 1Document22 pagesCommunity Presentation 1api-305705699No ratings yet
- Hmole NCPDocument4 pagesHmole NCPBettina Chua100% (1)
- Oral CareDocument5 pagesOral CareMelody Lim DayagNo ratings yet
- Post Insertion InstructionsDocument23 pagesPost Insertion InstructionsAnkita Reddy VallapNo ratings yet
- Information About GingivitisDocument4 pagesInformation About GingivitisazifattahNo ratings yet
- AssessmentDocument2 pagesAssessmentMark LedesmaNo ratings yet
- TCP For Oral HygieneDocument5 pagesTCP For Oral HygieneEnrico IgamaNo ratings yet
- A Guide To Oral Hygiene.: by Morna Wallace, Oral HygienistDocument25 pagesA Guide To Oral Hygiene.: by Morna Wallace, Oral HygienisthamamhamamNo ratings yet
- Teaching PlanDocument22 pagesTeaching Planapi-564432337No ratings yet
- Special Needs Treatment PlanDocument6 pagesSpecial Needs Treatment Planapi-742616973No ratings yet
- GINGIVITISDocument43 pagesGINGIVITISRamyaNo ratings yet
- Técnicas de Higiene OralDocument2 pagesTécnicas de Higiene OralEvelyn Torres CapetilloNo ratings yet
- General DentistryDocument5 pagesGeneral DentistryVinnova Dental ThurgoonaNo ratings yet
- Treatment Plan Assignment Lauren Farmer Kylie Hill Mackenzie Digmann Callie Verschoore Kirkwood Community CollegeDocument5 pagesTreatment Plan Assignment Lauren Farmer Kylie Hill Mackenzie Digmann Callie Verschoore Kirkwood Community Collegeapi-510470035No ratings yet
- Nutrition and The Teeth For Patients Receiving Radiotherapy To The Head and NeckDocument19 pagesNutrition and The Teeth For Patients Receiving Radiotherapy To The Head and NeckFadhlan Indra SNo ratings yet
- Infant Oral Health and Ant - GuidanceDocument53 pagesInfant Oral Health and Ant - GuidanceSonam RawatNo ratings yet
- Oral Health Case Study 1Document9 pagesOral Health Case Study 1royroyalasadiNo ratings yet
- Age Related Changes in Oral MucousDocument13 pagesAge Related Changes in Oral MucousJoyce Blancaflor LoganNo ratings yet
- Nursing Management of Oral HygieneDocument40 pagesNursing Management of Oral HygieneMheanne RomanoNo ratings yet
- What Does It Mean To Be Nil by Mouth?Document2 pagesWhat Does It Mean To Be Nil by Mouth?Alexandra PlugarNo ratings yet
- Promote Oral Health To Eldery Patients (By XHENI KUQO)Document47 pagesPromote Oral Health To Eldery Patients (By XHENI KUQO)XheniNo ratings yet
- Final Group DraftDocument5 pagesFinal Group Draftapi-663276816No ratings yet
- Sierra Health ORAL CARE CardsDocument40 pagesSierra Health ORAL CARE CardsAngela ReyesNo ratings yet
- Oral Care Power PointDocument14 pagesOral Care Power Pointmotherlyfeline23No ratings yet
- Strategies For Improving Oral Health Status of Elderly in Kudan Local Government Area of Kaduna StateDocument32 pagesStrategies For Improving Oral Health Status of Elderly in Kudan Local Government Area of Kaduna StateYUSUF AMINUNo ratings yet
- TX Plan 2Document5 pagesTX Plan 2api-662638224No ratings yet
- ORAL HYGIENE FOR ELDERLYDocument43 pagesORAL HYGIENE FOR ELDERLYPradeep GinigeNo ratings yet
- Module 11 - Oral Health - FINALDocument12 pagesModule 11 - Oral Health - FINALKevin FloresNo ratings yet
- Dental Care and Oral HealthDocument13 pagesDental Care and Oral HealthNasroNo ratings yet
- Tarlac State University College of Science Nursing DepartmentDocument3 pagesTarlac State University College of Science Nursing DepartmentKlara DyNo ratings yet
- Periodontal Care Plan 2015Document16 pagesPeriodontal Care Plan 2015api-286720788No ratings yet
- Patient Case PresentatioinDocument7 pagesPatient Case Presentatioinapi-727430180No ratings yet
- Oral Health DemkoDocument27 pagesOral Health DemkoMagdalena RejmerNo ratings yet
- English Task Fitriani Manik-2A.docDocument3 pagesEnglish Task Fitriani Manik-2A.docfitriyani manikNo ratings yet
- Treatment PlanDocument7 pagesTreatment Planapi-509270104No ratings yet
- Prostho IV-Slides 2 - Assessment of The Edentulous PatientDocument60 pagesProstho IV-Slides 2 - Assessment of The Edentulous Patientبراءة أحمد السلاماتNo ratings yet
- Young Dentist August13Document3 pagesYoung Dentist August13RusevNo ratings yet
- Group 5 Oral Hygiene Ncm109 LectureDocument6 pagesGroup 5 Oral Hygiene Ncm109 LectureShainaChescaEvansNo ratings yet
- Periodontal Care Plan - Thai HoangDocument21 pagesPeriodontal Care Plan - Thai Hoangapi-643588876No ratings yet
- Kindergarten Health Science Dental CareDocument4 pagesKindergarten Health Science Dental Carejanell edwardNo ratings yet
- Post-Perio Care PlanDocument8 pagesPost-Perio Care Planapi-663988238No ratings yet
- Patient EducationDocument22 pagesPatient EducationlbebberNo ratings yet
- Positive AttributesDocument2 pagesPositive AttributesHope SerquiñaNo ratings yet
- Critical Thinking Exercise 10Document3 pagesCritical Thinking Exercise 10Hope SerquiñaNo ratings yet
- Philippine Christian University: Bachelor of Science in Nursing (BSN)Document2 pagesPhilippine Christian University: Bachelor of Science in Nursing (BSN)Hope SerquiñaNo ratings yet
- NCP With ImplementationDocument4 pagesNCP With ImplementationHope SerquiñaNo ratings yet
- Vii. Risk Factors For Multiple Myeloma: Increasing AgeDocument8 pagesVii. Risk Factors For Multiple Myeloma: Increasing AgeHope SerquiñaNo ratings yet
- Case Sudy:: Thyroglossal Duct CystDocument21 pagesCase Sudy:: Thyroglossal Duct CystHope SerquiñaNo ratings yet
- Philippine Christian University: Mary Johnston College of NursingDocument2 pagesPhilippine Christian University: Mary Johnston College of NursingHope SerquiñaNo ratings yet
- LEARNING ACTIVITY 2 For RLE A Person With Acute Respiratory AcidosisDocument3 pagesLEARNING ACTIVITY 2 For RLE A Person With Acute Respiratory AcidosisHope SerquiñaNo ratings yet
- Episode 11 and 12Document4 pagesEpisode 11 and 12Hope SerquiñaNo ratings yet
- Episode 9 and 10Document4 pagesEpisode 9 and 10Hope SerquiñaNo ratings yet
- Learning Activity #1 For Related Learning Experience Nursing Care Plan For A Person With Fluid Volume ExcessDocument5 pagesLearning Activity #1 For Related Learning Experience Nursing Care Plan For A Person With Fluid Volume ExcessHope SerquiñaNo ratings yet
- Raven Yvonne Cleo Anne R. MolinaDocument2 pagesRaven Yvonne Cleo Anne R. MolinaHope SerquiñaNo ratings yet
- Mastectomy OutlineDocument6 pagesMastectomy OutlineHope SerquiñaNo ratings yet
- Episode 3 and 4Document4 pagesEpisode 3 and 4Hope SerquiñaNo ratings yet
- NizamazingDocument1 pageNizamazingHope SerquiñaNo ratings yet
- Serquina, Johniza Hope G. September 2, 2020 BSN 3A Pastor Janice Serafica A Living Sacrifice Romans 12:1-8Document1 pageSerquina, Johniza Hope G. September 2, 2020 BSN 3A Pastor Janice Serafica A Living Sacrifice Romans 12:1-8Hope SerquiñaNo ratings yet
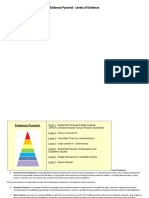
- Evidence Pyramid - Levels of EvidenceDocument3 pagesEvidence Pyramid - Levels of EvidenceHope SerquiñaNo ratings yet
- Pop MariellDocument6 pagesPop MariellHope SerquiñaNo ratings yet
- Moldez ExpectationsDocument1 pageMoldez ExpectationsHope SerquiñaNo ratings yet
- Pop DawnDocument5 pagesPop DawnHope SerquiñaNo ratings yet
- Reflection PaperDocument8 pagesReflection PaperHope SerquiñaNo ratings yet
- Pop TinDocument5 pagesPop TinHope SerquiñaNo ratings yet
- Saade 2015Document21 pagesSaade 2015divyaNo ratings yet
- Eed and Availability of Dentists and Specialists in Oral Medicine and Radiology A SurveyDocument5 pagesEed and Availability of Dentists and Specialists in Oral Medicine and Radiology A SurveyGede AnjasmaraNo ratings yet
- Consensus Report: Periodontic-Endodontic Lesions: Group MembersDocument2 pagesConsensus Report: Periodontic-Endodontic Lesions: Group MembersAlex Grande CancapaNo ratings yet
- DENTISTRYDocument15 pagesDENTISTRYKhanNo ratings yet
- 2080ISD - Isd 52 303Document6 pages2080ISD - Isd 52 303pyrockerNo ratings yet
- Crown LengtheningDocument54 pagesCrown LengtheningMehdi MoshaveriNo ratings yet
- Materi Tutor in EnglishDocument7 pagesMateri Tutor in EnglishDea RachnadewiNo ratings yet
- Essential Lines DR ChioderaDocument7 pagesEssential Lines DR ChioderaajiargoputroNo ratings yet
- Crash Course in PeriodonticsDocument115 pagesCrash Course in Periodonticsمعاذ العساف100% (1)
- Review Article: Mini-Implants in The Anchorage Armamentarium: New Paradigms in The OrthodonticsDocument9 pagesReview Article: Mini-Implants in The Anchorage Armamentarium: New Paradigms in The OrthodonticsDIANA PAOLA FONTECHA GONZÁLEZNo ratings yet
- Davis Nicholas C. An Artistic Approach To Smile Design.Document24 pagesDavis Nicholas C. An Artistic Approach To Smile Design.Trần Thị Như Ngọc100% (1)
- RelyX UnicemDocument2 pagesRelyX UnicemOral CareNo ratings yet
- Benevis Bankruptcy Doc 33 - Exhibit 1 PDFDocument57 pagesBenevis Bankruptcy Doc 33 - Exhibit 1 PDFDentist The MenaceNo ratings yet
- MurthyDocument4 pagesMurthyNADHIA NUR ALFIAHNo ratings yet
- Patients InvoiceDocument7 pagesPatients InvoiceVarenLagartoNo ratings yet
- Tangsripongkul2020 PDFDocument5 pagesTangsripongkul2020 PDFdrpriyanka patelNo ratings yet
- Pulpal PinsDocument8 pagesPulpal PinsGordana PuzovicNo ratings yet
- Making Occlusion 2Document7 pagesMaking Occlusion 2Ali QawasNo ratings yet
- Indices For Oral DiseasesDocument40 pagesIndices For Oral DiseaseskajdfaskNo ratings yet
- Dental BooklistDocument14 pagesDental Booklistالمكتبة المليونيةNo ratings yet
- Pain After Root Canal What To Expect, When To Get Help, and Why It HappensDocument7 pagesPain After Root Canal What To Expect, When To Get Help, and Why It Happensibrahim bataNo ratings yet
- Ada & AnsiDocument24 pagesAda & Ansikermink100% (3)
- Requisites of An Ideal Diagnostic ToolDocument2 pagesRequisites of An Ideal Diagnostic Tooljosefa lacanaNo ratings yet
- S20 Carbide Diamond BursDocument38 pagesS20 Carbide Diamond Bursvishali gejjeNo ratings yet
- Matricing and WedgingDocument19 pagesMatricing and Wedgingirfanuk69No ratings yet
- (20120228110933 Am) Samwumed Benefitsbrochure2012 WebDocument16 pages(20120228110933 Am) Samwumed Benefitsbrochure2012 WebsafinditNo ratings yet
- Rasmussen 2019Document13 pagesRasmussen 2019Lisdany BecerraNo ratings yet
- Currículo Profissional - Tamize InglesDocument7 pagesCurrículo Profissional - Tamize InglesTamize SILVA GONCALVESNo ratings yet
- Dental and Craniomaxillofacial Implant SurgeryDocument35 pagesDental and Craniomaxillofacial Implant SurgeryJean Carlos Barbosa FerreiraNo ratings yet