Download as pdf or txt
You might also like
- Instant Download Ebook PDF Abnormal Psychology 9th Edition PDF ScribdDocument41 pagesInstant Download Ebook PDF Abnormal Psychology 9th Edition PDF Scribdvictor.lewis791100% (53)
- Vitamins VM0822Document57 pagesVitamins VM0822fdfsdfNo ratings yet
- Cutting HandlingDocument25 pagesCutting HandlingWalid AmdouniNo ratings yet
- Dentistry in Post COVIDDocument3 pagesDentistry in Post COVIDsagrika groverNo ratings yet
- Caries Experience Before and After COVID-19 Restrictions: An Observational StudyDocument14 pagesCaries Experience Before and After COVID-19 Restrictions: An Observational Studyed_mariachiNo ratings yet
- Leake2008 PDFDocument9 pagesLeake2008 PDFjhon killNo ratings yet
- Pattern and Factors Associated With Utilisation of Dental ServicesDocument13 pagesPattern and Factors Associated With Utilisation of Dental ServicesKaitwa MbuyaNo ratings yet
- How COVID-19 Has Affected DentistryDocument13 pagesHow COVID-19 Has Affected DentistryDeborah AnneNo ratings yet
- Impact of The COVID-19 Pandemic On The TimingDocument8 pagesImpact of The COVID-19 Pandemic On The TimingMichael PomaNo ratings yet
- Oral Diseases - 2023 - JainDocument7 pagesOral Diseases - 2023 - JainGita PratamaNo ratings yet
- Dental Utilization AlgsgsDocument2 pagesDental Utilization AlgsgsMustafaNo ratings yet
- Covid-19 Outbreak - Immediate and Long-Term Impacts On The Dental ProfessionDocument4 pagesCovid-19 Outbreak - Immediate and Long-Term Impacts On The Dental ProfessionYasir IsrarNo ratings yet
- Should NHS Dentistry Be FreeDocument4 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Intro To Biological DentistryDocument7 pagesIntro To Biological DentistryFelipe LazzarottoNo ratings yet
- COVID-19's Impact On Private Practice and Academic Dentistry in North AmericaDocument4 pagesCOVID-19's Impact On Private Practice and Academic Dentistry in North AmericaJoDaNo ratings yet
- Coronavirus Disease 2019 and Dental Care For Older Adults: CommentaryDocument4 pagesCoronavirus Disease 2019 and Dental Care For Older Adults: CommentaryDerya İçözNo ratings yet
- Dental Health AustraliaDocument8 pagesDental Health AustraliajohnmccauleyNo ratings yet
- Ijerph 17 09053Document13 pagesIjerph 17 09053ismupechNo ratings yet
- 2.1. HESC 2720 - UNIT 2 - Written Assignment - ZSDocument4 pages2.1. HESC 2720 - UNIT 2 - Written Assignment - ZSodjegbaonoriodeNo ratings yet
- Should NHS Dentistry Be FreeDocument3 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Access To Dental Care For Mentally and Physically Challenge Populati OnDocument18 pagesAccess To Dental Care For Mentally and Physically Challenge Populati Onapi-239990812No ratings yet
- Should NHS Dentistry Be FreeDocument3 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Dental-Spending 2016Document9 pagesDental-Spending 2016EstreLLA ValenciaNo ratings yet
- Endodontic Treatment During COVID-19 Pandemic - Economic Perception of Dental ProfessionalsDocument8 pagesEndodontic Treatment During COVID-19 Pandemic - Economic Perception of Dental Professionalsbobs_fisioNo ratings yet
- Ijerph 18 05889Document18 pagesIjerph 18 05889Febri YolandaNo ratings yet
- Assignment (Group 2)Document3 pagesAssignment (Group 2)Marwa MohassebNo ratings yet
- Assignment (Group 2)Document3 pagesAssignment (Group 2)Marwa MohassebNo ratings yet
- Annotated BibliographyDocument5 pagesAnnotated BibliographyMarielle Dale SolanoNo ratings yet
- Dental Caries PandemicDocument5 pagesDental Caries PandemicKarla González GNo ratings yet
- Cdha Position Paper-2Document10 pagesCdha Position Paper-2api-596913754No ratings yet
- Grand Challenges in Community Oral HealthDocument2 pagesGrand Challenges in Community Oral HealthOfelia ReyesNo ratings yet
- The Oral Health Information Suite (OHIS) : Its Use in The Management of Periodontal DiseaseDocument12 pagesThe Oral Health Information Suite (OHIS) : Its Use in The Management of Periodontal DiseasejemmysenseiNo ratings yet
- APS Dentists As Oral Physicians The Overlooked PrimaryDocument13 pagesAPS Dentists As Oral Physicians The Overlooked PrimaryANGIE LORENA TORRES GUALINo ratings yet
- Lancet2 2Document12 pagesLancet2 2vatankhahpooyaNo ratings yet
- (12-18) Targeting Poor Health Improving Oral Health For The Poor and The Under ServedDocument8 pages(12-18) Targeting Poor Health Improving Oral Health For The Poor and The Under ServedAlexander DeckerNo ratings yet
- Oral Health Disparities Among The Elderly: Interdisciplinary Challenges For The FutureDocument10 pagesOral Health Disparities Among The Elderly: Interdisciplinary Challenges For The FutureJASPREETKAUR0410No ratings yet
- 2020 Article 1180Document15 pages2020 Article 1180cdsd-2011No ratings yet
- Dentistry and Coronavirus (COVID-19) - Moral Decision-MakingDocument3 pagesDentistry and Coronavirus (COVID-19) - Moral Decision-MakingOTNo ratings yet
- Special Care Dentistry and COVID-19 Outbreak: What Lesson Should We Learn?Document3 pagesSpecial Care Dentistry and COVID-19 Outbreak: What Lesson Should We Learn?Febriani SerojaNo ratings yet
- Instrumentation For The Treatment of Periodontal DiseaseDocument11 pagesInstrumentation For The Treatment of Periodontal DiseaseEga Tubagus Aprian100% (2)
- Elective Care and Health Services Research in The COVID-19 EraDocument2 pagesElective Care and Health Services Research in The COVID-19 Erajames bondNo ratings yet
- 1group B - First Draft v6Document17 pages1group B - First Draft v6Abdullah AmjadNo ratings yet
- Should NHS Dentistry Be FreeDocument4 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- Substance Use Disorders and COVID 19 TheDocument7 pagesSubstance Use Disorders and COVID 19 TheIvan CastellanosNo ratings yet
- DraftDocument2 pagesDraftMustafaNo ratings yet
- Oral Health ElderlyDocument2 pagesOral Health ElderlyatikramadhaniNo ratings yet
- Corona Dentist Awareness PerceptionDocument7 pagesCorona Dentist Awareness PerceptionFirda IzzatiNo ratings yet
- Knowledge Dental Anxiety and Patient ExpectationsDocument9 pagesKnowledge Dental Anxiety and Patient ExpectationsbenjoscoliNo ratings yet
- Another Part3Document3 pagesAnother Part3CAJES NOLINo ratings yet
- JOHOE - Volume 11 - Issue 1 - Pages 1-4Document4 pagesJOHOE - Volume 11 - Issue 1 - Pages 1-4vatankhahpooyaNo ratings yet
- Personalisation and Pandemic An Unforeseen Collision CourseDocument7 pagesPersonalisation and Pandemic An Unforeseen Collision CourseSylvia ThohariNo ratings yet
- The Impact of The COVID-19 Epidemic On The Utilization of Emergency Dental ServicesDocument4 pagesThe Impact of The COVID-19 Epidemic On The Utilization of Emergency Dental ServicesMishellKarelisMorochoSegarraNo ratings yet
- Should NHS Dentistry Be FreeDocument4 pagesShould NHS Dentistry Be FreePranav SivakumarNo ratings yet
- 237 Sophia Gomes Literature Review PaperDocument8 pages237 Sophia Gomes Literature Review Paperapi-720120569No ratings yet
- Caries Process and Prevention StrategiesDocument12 pagesCaries Process and Prevention Strategiesblacknight_81No ratings yet
- Policy Healthcare ReformDocument3 pagesPolicy Healthcare Reformsonia_groff6256No ratings yet
- The Future Direction of The Dental Public Health in MalaysiaDocument3 pagesThe Future Direction of The Dental Public Health in Malaysiaqiao fenNo ratings yet
- Dent Update 2021 48 521-522Document2 pagesDent Update 2021 48 521-522Mehwish MunawarNo ratings yet
- How Has Covid 19 Affected The Sector and Dental Health?Document5 pagesHow Has Covid 19 Affected The Sector and Dental Health?api-643791617No ratings yet
- Dentist - Edited.edited DennowDocument6 pagesDentist - Edited.edited DennowMosesNo ratings yet
- Access To Dental Care and Differences of Barriers and Their Management Between Developing and Developed CountriesDocument7 pagesAccess To Dental Care and Differences of Barriers and Their Management Between Developing and Developed CountriesSadiaNo ratings yet
- Dental Care During COVID-19 Outbreak: A Web-Based SurveyDocument7 pagesDental Care During COVID-19 Outbreak: A Web-Based SurveyDermatoLovers OficialNo ratings yet
- Infection Control in the Dental Office: A Global PerspectiveFrom EverandInfection Control in the Dental Office: A Global PerspectiveLouis G. DePaolaNo ratings yet
- Cuyahoga County Executive Armond Budish End of Term ReportDocument28 pagesCuyahoga County Executive Armond Budish End of Term ReportWKYC.comNo ratings yet
- IKDRC Class-II, III 03-2023Document4 pagesIKDRC Class-II, III 03-2023GudellikiritibabuNo ratings yet
- Alternative Work Scheme vs. On Site Labor PhilippinesDocument3 pagesAlternative Work Scheme vs. On Site Labor PhilippinesLayaDioknoNo ratings yet
- Fit For Frailty Part 1Document22 pagesFit For Frailty Part 1or1da2sa3No ratings yet
- Simulacro de Seguimiento Académico Simulacro de Seguimiento AcadémicoDocument6 pagesSimulacro de Seguimiento Académico Simulacro de Seguimiento Académicoalessa garciaNo ratings yet
- Rguhs Thesis Topics in PeriodonticsDocument5 pagesRguhs Thesis Topics in PeriodonticsSara Perez100% (2)
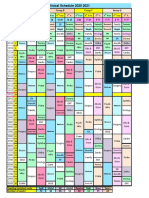
- R Schedule 2020 2021Document1 pageR Schedule 2020 2021Mohammed AhmedNo ratings yet
- Approaches To The Study of Hypnotic Dreams: Charles T. TartDocument1 pageApproaches To The Study of Hypnotic Dreams: Charles T. TartIno MoxoNo ratings yet
- Standards and Audit For Quality Assurance NURSING ADMINIDocument20 pagesStandards and Audit For Quality Assurance NURSING ADMINILIDIYA MOL P V100% (1)
- Historia de La OrtodonciaDocument9 pagesHistoria de La Ortodonciacarmonao.carina94No ratings yet
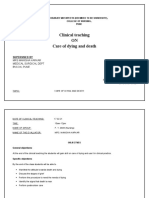
- Lesson Plan Death CareDocument19 pagesLesson Plan Death CareLoma Waghmare (Jadhav)No ratings yet
- Cat ReproductionDocument22 pagesCat ReproductionKatrina Ponce100% (1)
- IntrotoASD - Friendship PresentationDocument17 pagesIntrotoASD - Friendship PresentationasmaaaaltoumNo ratings yet
- Assignment Ni Ayang Sa TechnologyDocument2 pagesAssignment Ni Ayang Sa TechnologyJohn Mico MacatigbacNo ratings yet
- Types/Classification and Dichotomies: ResearchDocument21 pagesTypes/Classification and Dichotomies: ResearchAdrian Baguna MontemorNo ratings yet
- 8 - Case Studies in Ultrasonic Debridement - Pocket DentistryDocument7 pages8 - Case Studies in Ultrasonic Debridement - Pocket Dentistryfarahpasha16No ratings yet
- Sustainable Development Goal 2 - Zero HungerDocument11 pagesSustainable Development Goal 2 - Zero HungeralomerdenisNo ratings yet
- Metabolic Energy SystemsDocument9 pagesMetabolic Energy SystemsErwan Sha Habinullah100% (2)
- W Advantage VolunteerDocument2 pagesW Advantage VolunteerLinh Ngô ThịNo ratings yet
- The Joker Analysis QuestionsDocument2 pagesThe Joker Analysis Questionslettybadran2007No ratings yet
- Risk Factors of Anastomotic Leak in Intestinal Surgery AuthorDocument2 pagesRisk Factors of Anastomotic Leak in Intestinal Surgery AuthorluisNo ratings yet
- National Hospital Discharge SurveyDocument623 pagesNational Hospital Discharge SurveyadynopaldiNo ratings yet
- Key Components of Literature ReviewDocument8 pagesKey Components of Literature Reviewhinlcxtkg100% (1)
- dm2019-0365 Interim Guidelines On LNS SQDocument8 pagesdm2019-0365 Interim Guidelines On LNS SQMary Joy GaloloNo ratings yet
- DG Du Diabète Type 1Document1 pageDG Du Diabète Type 1Daoud IssaNo ratings yet
- Employees State Insurance Corporation Results of Computer Based Test/Examination (Online) Held On 26Th and 27Th February, 2019 Region Wise Merit List For All Candidates REGION: West BengalDocument55 pagesEmployees State Insurance Corporation Results of Computer Based Test/Examination (Online) Held On 26Th and 27Th February, 2019 Region Wise Merit List For All Candidates REGION: West BengalRanadeep PalNo ratings yet
- Journal Reading: "A Case of Hanging With Creeper in Secluded Place: Suicide or Homicide?"Document21 pagesJournal Reading: "A Case of Hanging With Creeper in Secluded Place: Suicide or Homicide?"Azam alausyNo ratings yet