Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5825)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (903)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (541)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (823)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Java Programming AssignmentDocument2 pagesJava Programming Assignmentvikas_saini_4uNo ratings yet
- AS4041 ASME B31 - 3 Pipe Wall ThicknessDocument11 pagesAS4041 ASME B31 - 3 Pipe Wall Thicknessamini_mohiNo ratings yet
- Pipe Span ChartDocument1 pagePipe Span ChartazamshafiqNo ratings yet
- Hybrid Modeling of Complex Surfaces Using Catia V5Document4 pagesHybrid Modeling of Complex Surfaces Using Catia V5babrolNo ratings yet
- 1St Quarter Self Learning Modules Availability Status Report As Of: - DivisionDocument4 pages1St Quarter Self Learning Modules Availability Status Report As Of: - DivisionCatherine Ababon100% (1)
- 55 60 Manual Tilt SystemDocument38 pages55 60 Manual Tilt SystemRyan ActonNo ratings yet
- EnthalpyDocument11 pagesEnthalpyRosy PhutelaNo ratings yet
- T Chart WeeblyDocument1 pageT Chart Weeblyapi-449513893No ratings yet
- CRAN (2022) - Package 'Factoextra'Document84 pagesCRAN (2022) - Package 'Factoextra'Luciano BorgoglioNo ratings yet
- AFT Fathom12 Product HelpDocument804 pagesAFT Fathom12 Product HelpJoel CNo ratings yet
- Specification of Injection Moulding MachineDocument4 pagesSpecification of Injection Moulding MachineNIKHIL PATHADENo ratings yet
- Tea Stain Decolorization by Vinegar and Bleach (With Image Analysis) (Hester 2016)Document13 pagesTea Stain Decolorization by Vinegar and Bleach (With Image Analysis) (Hester 2016)login ackyipNo ratings yet
- Quick Contact BadgeDocument8 pagesQuick Contact Badgeamitl11794No ratings yet
- Essentials of Enthalpy and Hess's Law NotesDocument10 pagesEssentials of Enthalpy and Hess's Law NotesAndreaMarkham100% (1)
- Experiment 12: Simple Harmonic Motion: I. About The ExperimentDocument6 pagesExperiment 12: Simple Harmonic Motion: I. About The ExperimentAnurag SharmaNo ratings yet
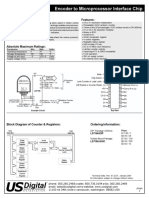
- Encoder To Microprocessor Interface Chip Chips: Features: DescriptionDocument3 pagesEncoder To Microprocessor Interface Chip Chips: Features: DescriptionasdNo ratings yet
- Quote CT PT Isolator VCB AB Switch Drop Out Fuse Set TPMO SMC LT Distribution Box HT PanelDocument11 pagesQuote CT PT Isolator VCB AB Switch Drop Out Fuse Set TPMO SMC LT Distribution Box HT PanelSharafatNo ratings yet
- Time and Work Shotcut 806ccc96Document4 pagesTime and Work Shotcut 806ccc96sanjay kumarNo ratings yet
- Calcaneal FracturesDocument39 pagesCalcaneal FracturesNavin ChandarNo ratings yet
- Non-Gazetted First ClassDocument48 pagesNon-Gazetted First ClasssharmalokrajNo ratings yet
- DG型高压锅炉给水泵说明书 tài liệu kỹ thuật bơm cấpDocument26 pagesDG型高压锅炉给水泵说明书 tài liệu kỹ thuật bơm cấpMạnh CườngNo ratings yet
- Introduction To Industrial Automation Topic 1Document13 pagesIntroduction To Industrial Automation Topic 1Vedant .ChavanNo ratings yet
- Integrated Circuits and Its Applications - Unit 5 - WWW - Rgpvnotes.inDocument28 pagesIntegrated Circuits and Its Applications - Unit 5 - WWW - Rgpvnotes.inShekhar Suman SoniNo ratings yet
- 05 12399 SGE BartosDocument13 pages05 12399 SGE BartosSanford SiegelNo ratings yet
- HTR India - Products - Wire Wound Resistors - Silicone Coated Resistors - HTA (English)Document3 pagesHTR India - Products - Wire Wound Resistors - Silicone Coated Resistors - HTA (English)crplzNo ratings yet
- Light 2022Document31 pagesLight 2022daley dailyNo ratings yet
- Articulo de Revision Unidad IIIDocument17 pagesArticulo de Revision Unidad IIIYeiru Azael RatmareNo ratings yet
- Lecture Notes 11-Euler Method-IIDocument59 pagesLecture Notes 11-Euler Method-IITesfaye Teferi ShoneNo ratings yet
- CyberAces Module1-Windows 1 InstallingWindowsDocument40 pagesCyberAces Module1-Windows 1 InstallingWindowsAbiodun AmusatNo ratings yet
- The Rafiki MapDocument72 pagesThe Rafiki MapAnonymous Y2qwEuANo ratings yet