Download as pdf or txt
You might also like
- Outsmart Your Cancer - Tanya PierceDocument530 pagesOutsmart Your Cancer - Tanya PierceParallaxster100% (4)
- Clinical Skills Review: Scenarios Based on Standardized PatientsFrom EverandClinical Skills Review: Scenarios Based on Standardized PatientsRating: 4 out of 5 stars4/5 (10)
- Nac OsceDocument1,089 pagesNac OsceVikrantNo ratings yet
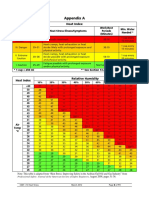
- Heat Index ChartDocument1 pageHeat Index ChartAnvarsha Sharafudheen100% (1)
- Form - Student Health Certificate-1Document2 pagesForm - Student Health Certificate-1hmhida33% (3)
- Apollo Fire Alarm Design Guide PDFDocument100 pagesApollo Fire Alarm Design Guide PDFlima muslih100% (3)
- Plattischemic Stroke Lesson PlanDocument18 pagesPlattischemic Stroke Lesson Planapi-216258123100% (3)
- Stamp Screening FormDocument3 pagesStamp Screening FormStefanie HonkkNo ratings yet
- Pfizer Analysis PDFDocument3 pagesPfizer Analysis PDFBhumika ChaubeNo ratings yet
- Physical ActivityDocument30 pagesPhysical ActivityMakisKingSamiotisNo ratings yet
- Scenario - CVA PATIENTDocument3 pagesScenario - CVA PATIENTfmNo ratings yet
- BMJ Present Clinical CasesDocument4 pagesBMJ Present Clinical CasesmehdNo ratings yet
- Research Proposal 1000 Copy 2Document6 pagesResearch Proposal 1000 Copy 2سعد الدوسريNo ratings yet
- AVYKDocument6 pagesAVYKMinh Thành Trí LêNo ratings yet
- Patient Education ToolkitDocument15 pagesPatient Education ToolkitI Nyoman Gede SemarajanaNo ratings yet
- Appendix B: Analysis Plan/Application Data/materialsDocument6 pagesAppendix B: Analysis Plan/Application Data/materialsOtieno MosesNo ratings yet
- Health HistoryDocument8 pagesHealth HistoryAhmed MohamedNo ratings yet
- Long Case Year 3 B2023Document41 pagesLong Case Year 3 B2023Mary AmeenNo ratings yet
- Well Built QuestionDocument2 pagesWell Built QuestiondnaritaNo ratings yet
- University of Nevada, Reno School of Medicine Syllabus: Internal Medicine Clerkship, Elko Imed 651 Elko, NevadaDocument29 pagesUniversity of Nevada, Reno School of Medicine Syllabus: Internal Medicine Clerkship, Elko Imed 651 Elko, NevadaAna CanastraNo ratings yet
- From Clinical Observations To Research: Dr. Dick Menzies June 10, 2005Document36 pagesFrom Clinical Observations To Research: Dr. Dick Menzies June 10, 2005Santi PadmasariNo ratings yet
- Stroke Risk Screening Scales (SRSS) : Identi Fication of Domain and Item GenerationDocument8 pagesStroke Risk Screening Scales (SRSS) : Identi Fication of Domain and Item Generationandi kurniawanNo ratings yet
- Functional Assessment in GeriatricsDocument26 pagesFunctional Assessment in GeriatricsAaliyah ShaikhNo ratings yet
- Medical Rotation Bridging ExercisesDocument8 pagesMedical Rotation Bridging ExercisesAaron AndreyiNo ratings yet
- MagatismDocument22 pagesMagatismJames MasomeNo ratings yet
- NAC OSCE - Basics UnderstandingDocument3 pagesNAC OSCE - Basics Understandingteena6506763No ratings yet
- Example Information Sheet and Consent Form (University of Edinburgh PREC)Document7 pagesExample Information Sheet and Consent Form (University of Edinburgh PREC)bpreger100% (1)
- Submission of Project SynopsisDocument3 pagesSubmission of Project SynopsisAji KoshyNo ratings yet
- Data Collection and Analysis in Obstetrics and GynecologyDocument47 pagesData Collection and Analysis in Obstetrics and Gynecologyapi-3705046No ratings yet
- TestDocument7 pagesTestgekwahyuNo ratings yet
- Self ManagementDocument12 pagesSelf Managementjustin_saneNo ratings yet
- SCIP Duaa - JSDocument9 pagesSCIP Duaa - JSOtieno MosesNo ratings yet
- 14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Document9 pages14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Danielcc Lee100% (1)
- Critical Appraisal of Prognostic Studies: Zwasta Pribadi MahardhikaDocument15 pagesCritical Appraisal of Prognostic Studies: Zwasta Pribadi MahardhikatiasyalitaNo ratings yet
- Course Outline NEPH201Document12 pagesCourse Outline NEPH201Jeffrey Ian M. KoNo ratings yet
- Descriptive StudiesDocument38 pagesDescriptive StudiesMai MaiNo ratings yet
- EBM - Critical Appraisal of Prognostic StudiesDocument24 pagesEBM - Critical Appraisal of Prognostic StudiesNabilla Sophia Sofyan100% (2)
- JournalDocument7 pagesJournalcarina adrianaNo ratings yet
- Stroke Research PaperDocument4 pagesStroke Research Paperegx124k2100% (1)
- Example Information Sheet and Consent Form (University of Edinburgh PREC)Document4 pagesExample Information Sheet and Consent Form (University of Edinburgh PREC)Pragathees RamamoorthiNo ratings yet
- M3A1 EHR Go Case Study Review (Associate)Document4 pagesM3A1 EHR Go Case Study Review (Associate)srgilbert01No ratings yet
- Anglais 2022Document25 pagesAnglais 2022manelkandolo0818851800No ratings yet
- Cebm Prognosis WorksheetDocument4 pagesCebm Prognosis WorksheetLinda Wdl IINo ratings yet
- Psychology Ethics Form - KKK - MSCDocument7 pagesPsychology Ethics Form - KKK - MSCSindujaa SelliahNo ratings yet
- COPD Secondaryto PTBDocument142 pagesCOPD Secondaryto PTBallexiscampaner100% (2)
- Optometric Case AnalysisDocument93 pagesOptometric Case AnalysisJoseph Israel100% (1)
- Unit 6 Case Presentation: 6.0 ObjectivesDocument10 pagesUnit 6 Case Presentation: 6.0 ObjectivesSatosh KapdiNo ratings yet
- Clerking PatientsDocument7 pagesClerking PatientsJx ChamNo ratings yet
- Orthodontics: History Taking and ExaminationDocument39 pagesOrthodontics: History Taking and ExaminationNingombam RobinsonNo ratings yet
- 2014 Coma StimualtionDocument5 pages2014 Coma Stimualtionvidyasagar pagillaNo ratings yet
- Basic EpidemiologyDocument16 pagesBasic EpidemiologyNeil Victor Ongco PajugotNo ratings yet
- Cebm Prognosis Worksheet PDFDocument3 pagesCebm Prognosis Worksheet PDFdian_c87No ratings yet
- Types of Study DesignDocument28 pagesTypes of Study DesignMina Mesri100% (1)
- Rle 106 ReqDocument10 pagesRle 106 Reqbeer_ettaaNo ratings yet
- Cebm Prognosis Worksheet PDFDocument3 pagesCebm Prognosis Worksheet PDFThalia KarampasiNo ratings yet
- Mustansiriyah Lecture Notes On Surgical History & Clinical ExaminationDocument57 pagesMustansiriyah Lecture Notes On Surgical History & Clinical Examinationنور الهدى ابراهيم خضير معيليNo ratings yet
- Medical Ethics 2023 FINALDocument56 pagesMedical Ethics 2023 FINALBelinda ELISHANo ratings yet
- Individual C.P Ns2 FinalDocument69 pagesIndividual C.P Ns2 FinalDonna RillonNo ratings yet
- 4th Year Ophthalmology Study Guide1430-31 (1) .Doc11-11-09Document33 pages4th Year Ophthalmology Study Guide1430-31 (1) .Doc11-11-09ishtiaqahmadgujjar100% (1)
- Patient History: Prof. Hoda ElguindyDocument14 pagesPatient History: Prof. Hoda Elguindyyahia salah100% (1)
- 02 Paed History Exam & Procedures-2010Document56 pages02 Paed History Exam & Procedures-2010AnastasiafynnNo ratings yet
- Guide To History TakingDocument55 pagesGuide To History TakingGabriella Hild100% (1)
- Clinical Profile of Stroke Patients Admitted in CMCTH: DR Deepak SarrafDocument31 pagesClinical Profile of Stroke Patients Admitted in CMCTH: DR Deepak SarrafajNo ratings yet
- Screening For Good Health: The Australian Guide To Health Screening And ImmunisationFrom EverandScreening For Good Health: The Australian Guide To Health Screening And ImmunisationNo ratings yet
- The Pearls of Communication, History Taking, and Physical Examination: The Road to Passing Clinical ExaminationsFrom EverandThe Pearls of Communication, History Taking, and Physical Examination: The Road to Passing Clinical ExaminationsRating: 5 out of 5 stars5/5 (1)
- Effective Discharge Planning PDFDocument2 pagesEffective Discharge Planning PDFL AzNo ratings yet
- Yokoten Accident - Dec'23Document1 pageYokoten Accident - Dec'23MTS EHSNo ratings yet
- Ebook Fundamentals of Pharmacognosy and Phytotherapy PDF Full Chapter PDFDocument59 pagesEbook Fundamentals of Pharmacognosy and Phytotherapy PDF Full Chapter PDFmary.rainey124100% (34)
- Material Safety Data Sheet Reotan LDocument4 pagesMaterial Safety Data Sheet Reotan Lfs1640No ratings yet
- Meditech Surgical: Group MembersDocument18 pagesMeditech Surgical: Group MembersPatxiAranaNo ratings yet
- Chalmers Stressful Life Events: Their Past and PresentDocument15 pagesChalmers Stressful Life Events: Their Past and PresentAna Rivera CastañonNo ratings yet
- 2011 99Document8 pages2011 99Agung GinanjarNo ratings yet
- Oxyblock DDocument13 pagesOxyblock DВиталий ВойкуNo ratings yet
- Mortuary ServicesDocument30 pagesMortuary ServicesYogesh ChandraNo ratings yet
- Pharmacology SlidesDocument114 pagesPharmacology Slidesbrandon15000100% (9)
- Kalpa CleanseDocument21 pagesKalpa CleanseCristina Cobzaru100% (1)
- Canterpene For Lifespan Healthspan AugmentationDocument41 pagesCanterpene For Lifespan Healthspan AugmentationMorris F. JohnsonNo ratings yet
- Articaine Vs LidocaineDocument25 pagesArticaine Vs LidocainecjoybensondmdNo ratings yet
- Acute PancreatitisDocument9 pagesAcute PancreatitisestefygomezsNo ratings yet
- Foot Reflexology: We Recommend That You Allocate at Least 30 Minutes To This WorksheetDocument5 pagesFoot Reflexology: We Recommend That You Allocate at Least 30 Minutes To This WorksheetAstro TriinityNo ratings yet
- Presented Before The Annual Meeting of The American Association of Orthodontists, Dal-Las, Texas, April, 1953Document13 pagesPresented Before The Annual Meeting of The American Association of Orthodontists, Dal-Las, Texas, April, 1953Paola LoloNo ratings yet
- Bach Flower PDFDocument7 pagesBach Flower PDFjosephNo ratings yet
- C.coek - Info Comprehensive Gynecology Review 4th EditionDocument1 pageC.coek - Info Comprehensive Gynecology Review 4th EditionCylyn Ann CabatinganNo ratings yet
- Intro To SoundDocument16 pagesIntro To SoundsnailbookNo ratings yet
- Observing Children-Notes From Montessori's 1921 London CourseDocument6 pagesObserving Children-Notes From Montessori's 1921 London CourseSally Morales de SayanNo ratings yet
- Aditya Birla - Claim - FormDocument9 pagesAditya Birla - Claim - FormSaransh KumarNo ratings yet
- Stellaris PC NewDocument16 pagesStellaris PC Newsandip shelakeNo ratings yet
- kAMUS by Assafik Poli JantungDocument11 pageskAMUS by Assafik Poli JantungassafikNo ratings yet
- Stemetil DCS SlideDocument31 pagesStemetil DCS SlideSanchit GargNo ratings yet
- Kapuno, Natalie EveDocument1 pageKapuno, Natalie EveVee KeeNo ratings yet