Download as pdf or txt
You might also like
- Envision Math Homework Workbook Grade 4Document6 pagesEnvision Math Homework Workbook Grade 4afnafqbjjlapla100% (1)
- Owners Handbook - BUKH DV 24 RMEDocument24 pagesOwners Handbook - BUKH DV 24 RMELeonid Kolesnikov50% (2)
- WNG Upright Action ProcedureDocument31 pagesWNG Upright Action ProcedureChris HsiaoNo ratings yet
- SF-HC30A3 Manual Sensor de AlturaDocument35 pagesSF-HC30A3 Manual Sensor de AlturaRoberto Medina100% (3)
- Tutorial 4 - Business AnalyticsDocument14 pagesTutorial 4 - Business AnalyticsRobin RichardsonNo ratings yet
- AVEVA E3D Tutorial Equipment Modeling With Practical ExampleDocument8 pagesAVEVA E3D Tutorial Equipment Modeling With Practical ExampleRamon Alejandro Porras Hernandez100% (1)
- Chaffee Et Al 2015 Feeding Practices and Caries Incidence in Early Childhood CDOEDocument11 pagesChaffee Et Al 2015 Feeding Practices and Caries Incidence in Early Childhood CDOENajara RodriguesNo ratings yet
- Early Childhood Caries and Body Mass Index in Young Children From Low Income FamiliesDocument12 pagesEarly Childhood Caries and Body Mass Index in Young Children From Low Income FamiliesAmandeep ChopraNo ratings yet
- Nutritional Status of School Age Children in Private Elementary Schools: Basis For A Proposed Meal Management PlanDocument5 pagesNutritional Status of School Age Children in Private Elementary Schools: Basis For A Proposed Meal Management PlanIjaems JournalNo ratings yet
- Association Between Breastfeeding and Dental Caries in Japanese ChildrenDocument6 pagesAssociation Between Breastfeeding and Dental Caries in Japanese ChildrenSusi susiNo ratings yet
- 1-S2.0-S0002916522010693-Main InterDocument8 pages1-S2.0-S0002916522010693-Main InterAlimah PutriNo ratings yet
- Long-Term Effectiveness of A Nutritional Program in Reducing Early Childhood Caries: A Randomized TrialDocument9 pagesLong-Term Effectiveness of A Nutritional Program in Reducing Early Childhood Caries: A Randomized Trialtitah rahayuNo ratings yet
- Flavio Art2art08 PDFDocument7 pagesFlavio Art2art08 PDFAngie EspinozaNo ratings yet
- 06 Original 02Document7 pages06 Original 02normanahmad92No ratings yet
- 31993436Document11 pages31993436Cattleya TanosseloNo ratings yet
- Beneficios de Prologar La LM Entre 30 59 Meses para El Correcto Desarrollo OrofacialDocument6 pagesBeneficios de Prologar La LM Entre 30 59 Meses para El Correcto Desarrollo OrofacialCésar Augusto Gamarra SantamariaNo ratings yet
- An Obesity Risk Assessment Tool For Young Childr 2018 Journal of Nutrition EDocument13 pagesAn Obesity Risk Assessment Tool For Young Childr 2018 Journal of Nutrition EErik agustioNo ratings yet
- Infant Dietary Patterns and Early Childhood Caries in A Multi-Ethnic Asian CohortDocument8 pagesInfant Dietary Patterns and Early Childhood Caries in A Multi-Ethnic Asian CohortRasciusNo ratings yet
- Research Revised March 22 2024Document39 pagesResearch Revised March 22 2024amandigNo ratings yet
- Ref KalsiumDocument10 pagesRef KalsiumAMALIA REZKI ANANDA D4 2018No ratings yet
- Medicion Del Nivel de AF y HA en Niños PARTE 1Document13 pagesMedicion Del Nivel de AF y HA en Niños PARTE 1Ricardo ArteagaNo ratings yet
- Bacterial Contamination of The Lacteal Contents of Feeding BottlesDocument9 pagesBacterial Contamination of The Lacteal Contents of Feeding BottlesOyNo ratings yet
- Artikel 4Document6 pagesArtikel 4Claudia BuheliNo ratings yet
- 7715 Article Text 54706 1 10 20220107Document9 pages7715 Article Text 54706 1 10 20220107jesusarlexlugofajardoNo ratings yet
- Situational Analysis of Nutritional Status Among 1989 Children Presenting With Cleft Lip Palate in IndonesiaDocument13 pagesSituational Analysis of Nutritional Status Among 1989 Children Presenting With Cleft Lip Palate in Indonesiacvdk8dc8sbNo ratings yet
- Associations of Childhood MaternaDocument15 pagesAssociations of Childhood MaternaNurlaili AlfisyahNo ratings yet
- Factors Associated With A Shorter Duration of Breastfeeding: Key Words Breastfeeding, Epidemiology, ChildDocument10 pagesFactors Associated With A Shorter Duration of Breastfeeding: Key Words Breastfeeding, Epidemiology, ChildyutefupNo ratings yet
- Bulan Madu Ala IslamDocument7 pagesBulan Madu Ala IslamAsror El-RomlyNo ratings yet
- Dietary Diversity at 6 Months of Age IsAssociated With Subsequent Growth Andmediates The Effect of Maternal Education Oninfant Growth in Urban ZambiaDocument8 pagesDietary Diversity at 6 Months of Age IsAssociated With Subsequent Growth Andmediates The Effect of Maternal Education Oninfant Growth in Urban ZambiaROSNINo ratings yet
- Megan Rollo ThesisDocument10 pagesMegan Rollo Thesistinamclellaneverett100% (1)
- BMC Public HealthDocument10 pagesBMC Public HealthPam Travezani MiyazakiNo ratings yet
- Fast FoodDocument8 pagesFast Foodkangna_sharma20No ratings yet
- Association of Breastfeeding Duration, NonnutritiveDocument5 pagesAssociation of Breastfeeding Duration, NonnutritiveIrma NovitasariNo ratings yet
- Prevalencia Amamentação Sul BrasilDocument8 pagesPrevalencia Amamentação Sul BrasilJulianaNo ratings yet
- J1 - 0104 0707 Tce 25 01 0220015Document8 pagesJ1 - 0104 0707 Tce 25 01 0220015أحمد نور الهدايةNo ratings yet
- EJCM - Volume 36 - Issue 1 - Pages 45-60-1Document16 pagesEJCM - Volume 36 - Issue 1 - Pages 45-60-1Yaumil FauziahNo ratings yet
- Breast-Feeding Performance Index - A Composite Index To Describe Overall Breast-Feeding Performance Among Infants Under 6 Months of AgeDocument9 pagesBreast-Feeding Performance Index - A Composite Index To Describe Overall Breast-Feeding Performance Among Infants Under 6 Months of AgeHuan VuongNo ratings yet
- Dietary Diversity Practice and Associated Factors Among Infants and Young Children in Haramaya Town, EthiopiaDocument8 pagesDietary Diversity Practice and Associated Factors Among Infants and Young Children in Haramaya Town, EthiopiaIJPHSNo ratings yet
- Belin2021 NutritionalScreeningDocument11 pagesBelin2021 NutritionalScreeningcaparrosolorena5No ratings yet
- Chen 2015Document9 pagesChen 2015Beatriz A GálvezNo ratings yet
- StuntingDocument9 pagesStuntingAnonymous q8VmTTtmXQNo ratings yet
- BurrowsDocument10 pagesBurrowsBenja NGNo ratings yet
- Exclusive Breastfeeding and Risk of Dental Malocclusion: ObjectivesDocument10 pagesExclusive Breastfeeding and Risk of Dental Malocclusion: ObjectivesingridspulerNo ratings yet
- Constipation in School-Aged Children at Public Schools in Rio de Janeiro, BrazilDocument7 pagesConstipation in School-Aged Children at Public Schools in Rio de Janeiro, BrazilZakia AmeliaNo ratings yet
- 2trik20191018 2trik TemplateDocument15 pages2trik20191018 2trik Templatedini afrianiNo ratings yet
- Addressing Malnutrition in School-Aged Children With A Diet Recommender SystemDocument15 pagesAddressing Malnutrition in School-Aged Children With A Diet Recommender SystemInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Chapter 1Document6 pagesChapter 1Geralden Vinluan PingolNo ratings yet
- Literature Review Childhood ObesityDocument4 pagesLiterature Review Childhood Obesityc5j07dce100% (1)
- Association of Breastfeeding and Three-Dimensional Dental Arch Relationships in Primary DentitionDocument9 pagesAssociation of Breastfeeding and Three-Dimensional Dental Arch Relationships in Primary DentitionCristobal EscobarNo ratings yet
- Dietary Patterns Exhibit Sex-Specific 3Document9 pagesDietary Patterns Exhibit Sex-Specific 3Luiz Eduardo RodriguezNo ratings yet
- HS390 Group6 ResearchDocument6 pagesHS390 Group6 Researchjoseyalm2323No ratings yet
- Literature Review About Childhood ObesityDocument5 pagesLiterature Review About Childhood Obesityd0vidihujam3100% (1)
- Copia de admin,+587-Article+Text-2097-1-11-20201110Document13 pagesCopia de admin,+587-Article+Text-2097-1-11-20201110aner cristobal alonso alonsoNo ratings yet
- Early Obesity Prevention - A Randomized Trial ofDocument7 pagesEarly Obesity Prevention - A Randomized Trial ofClaudia Rodrigues DiasNo ratings yet
- Childhood Obesity Research Paper ExampleDocument5 pagesChildhood Obesity Research Paper Examplecakvaw0q100% (1)
- Ajcn/nqz 033Document10 pagesAjcn/nqz 033cahyanidewi322No ratings yet
- Timely Introduction of Complementary Feeding Among Caregivers of Children 612 Month Sodo Town EthiopiaDocument3 pagesTimely Introduction of Complementary Feeding Among Caregivers of Children 612 Month Sodo Town EthiopiaProdi S1- 1BNo ratings yet
- Pacifier and Bottle Nipples: The Targets For Poor Breastfeeding OutcomesDocument3 pagesPacifier and Bottle Nipples: The Targets For Poor Breastfeeding Outcomesbeleg100% (1)
- Association of Picky Eating With Growth, Nutritional Status, Development, Physical Activity, and Health in Preschool ChildrenDocument9 pagesAssociation of Picky Eating With Growth, Nutritional Status, Development, Physical Activity, and Health in Preschool Childrenyeremias setyawanNo ratings yet
- Randomized Controlled Trial of A Primary Care-Based Child Obesity Prevention Intervention On Infant Feeding PracticesDocument9 pagesRandomized Controlled Trial of A Primary Care-Based Child Obesity Prevention Intervention On Infant Feeding PracticesSardono WidinugrohoNo ratings yet
- Nutrient Intakes of Infants and Toddlers: Objectives DesignDocument8 pagesNutrient Intakes of Infants and Toddlers: Objectives Designrehan ehanNo ratings yet
- Association of Exclusive Breastfeeding Duration With Consumption of Ultra-Processed Foods, Fruit and Vegetables in Brazilian ChildrenDocument8 pagesAssociation of Exclusive Breastfeeding Duration With Consumption of Ultra-Processed Foods, Fruit and Vegetables in Brazilian ChildrenYesi Pratama Aprilia NingrumNo ratings yet
- Knowledge and Attitudes Towards Baby-Led-Weaning by Health Professionals and Parents A Cross-Sectional Study.Document7 pagesKnowledge and Attitudes Towards Baby-Led-Weaning by Health Professionals and Parents A Cross-Sectional Study.myjesa07No ratings yet
- Sdarticle 142 PDFDocument1 pageSdarticle 142 PDFRio Michelle CorralesNo ratings yet
- Nurturing a Healthy Generation of Children: Research Gaps and Opportunities: 91st Nestlé Nutrition Institute Workshop, Manila, March 2018From EverandNurturing a Healthy Generation of Children: Research Gaps and Opportunities: 91st Nestlé Nutrition Institute Workshop, Manila, March 2018No ratings yet
- Building Future Health and Well-Being of Thriving Toddlers and Young Children: 95th Nestlé Nutrition Institute Workshop, September 2020From EverandBuilding Future Health and Well-Being of Thriving Toddlers and Young Children: 95th Nestlé Nutrition Institute Workshop, September 2020No ratings yet
- EJMCM Volume 7 Issue 11 Pages 5269-5275Document7 pagesEJMCM Volume 7 Issue 11 Pages 5269-5275Putu WidiastriNo ratings yet
- Diskusi KuretaseDocument9 pagesDiskusi KuretasePutu Widiastri100% (1)
- Cavernous Sinus Thrombosis 2Document4 pagesCavernous Sinus Thrombosis 2Putu WidiastriNo ratings yet
- Ultrasonic Scaling TechniqueDocument3 pagesUltrasonic Scaling TechniquePutu WidiastriNo ratings yet
- Accurate Detection of Non-Cavitated Proximal Caries in Posterior Permanent Teeth: An in Vivo StudyDocument6 pagesAccurate Detection of Non-Cavitated Proximal Caries in Posterior Permanent Teeth: An in Vivo StudyPutu WidiastriNo ratings yet
- Treatment of Severe Chronic Periodontitis With Surgical and Prosthetic Intervention: A 9-Year Follow-Up Case ReportDocument10 pagesTreatment of Severe Chronic Periodontitis With Surgical and Prosthetic Intervention: A 9-Year Follow-Up Case ReportPutu WidiastriNo ratings yet
- Cavernous Sinus Thrombosis of Odontogenic Origin: March 2016Document8 pagesCavernous Sinus Thrombosis of Odontogenic Origin: March 2016Putu WidiastriNo ratings yet
- Pengawasan Oleh Balai Pengawasan Obat Dan Makanan (Bpom) Terhadap Kosmetik Bahan Berbahaya Di Kota Padang ArtikelDocument15 pagesPengawasan Oleh Balai Pengawasan Obat Dan Makanan (Bpom) Terhadap Kosmetik Bahan Berbahaya Di Kota Padang ArtikelPutu WidiastriNo ratings yet
- Pengawasan Oleh Balai Pengawasan Obat Dan Makanan (Bpom) Terhadap Kosmetik Bahan Berbahaya Di Kota Padang ArtikelDocument15 pagesPengawasan Oleh Balai Pengawasan Obat Dan Makanan (Bpom) Terhadap Kosmetik Bahan Berbahaya Di Kota Padang ArtikelPutu WidiastriNo ratings yet
- Fairy Tales: Sleeping BeautyDocument1 pageFairy Tales: Sleeping BeautyPutu WidiastriNo ratings yet
- Prevalence and Severity of Gingivitis in School Students Aged 6-11 Years in Tafelah Governorate, South Jordan: Results of The Survey Executed by National Woman's Health Care CenterDocument7 pagesPrevalence and Severity of Gingivitis in School Students Aged 6-11 Years in Tafelah Governorate, South Jordan: Results of The Survey Executed by National Woman's Health Care CenterPutu WidiastriNo ratings yet
- Influence of Active Reminders On Oral Hygiene Compliance in Orthodontic PatientsDocument6 pagesInfluence of Active Reminders On Oral Hygiene Compliance in Orthodontic PatientsPutu WidiastriNo ratings yet
- Local Plaque and Plaque Retentive Factors. 2013pptDocument90 pagesLocal Plaque and Plaque Retentive Factors. 2013pptPutu WidiastriNo ratings yet
- Sonex Pilot's OperatingDocument35 pagesSonex Pilot's Operatingemerson magnoNo ratings yet
- Analysis and Design of Down-Aisle Pallet Rack StructuresDocument11 pagesAnalysis and Design of Down-Aisle Pallet Rack StructuresAbdalla Sharf EldienNo ratings yet
- Technical Guide Geotechnical Geologic ReportsDocument66 pagesTechnical Guide Geotechnical Geologic ReportsJulián Vargas ParraNo ratings yet
- PDF Algorithms Illuminated Part 3 Greedy Algorithms and Dynamic Programming 1St Edition Tim Roughgarden Ebook Full ChapterDocument53 pagesPDF Algorithms Illuminated Part 3 Greedy Algorithms and Dynamic Programming 1St Edition Tim Roughgarden Ebook Full Chapterkimberly.hawkins835100% (7)
- LEcture 14Document15 pagesLEcture 14asdsdNo ratings yet
- Use Nonextraction Treatment When Possihle: Assessment of Borderline PatientsDocument18 pagesUse Nonextraction Treatment When Possihle: Assessment of Borderline PatientsMonse Sanchez UrbinaNo ratings yet
- 6.hydrogen Its CompoundDocument17 pages6.hydrogen Its CompoundpjaindakNo ratings yet
- Esmm390 410S182Document2 pagesEsmm390 410S182Mulcue ProfeNo ratings yet
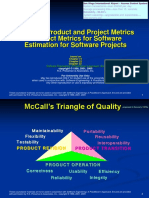
- Process, Product and Project Metrics Product Metrics For Software Estimation For Software ProjectsDocument46 pagesProcess, Product and Project Metrics Product Metrics For Software Estimation For Software ProjectsNassah AllaabNo ratings yet
- Additional Practice Questions - Structural IdealisationDocument9 pagesAdditional Practice Questions - Structural IdealisationXiuming ChenNo ratings yet
- ZIEHL ABEGG Operating Instructions ZAtop SM200 30C EnglishDocument56 pagesZIEHL ABEGG Operating Instructions ZAtop SM200 30C EnglishKely Bremm SchererNo ratings yet
- Cemb Data Sheet TR-26 Atex 06 GB PDFDocument2 pagesCemb Data Sheet TR-26 Atex 06 GB PDFhamzaNo ratings yet
- PPM Rebuild Unit Manual: Testing MethodDocument15 pagesPPM Rebuild Unit Manual: Testing MethodNGUYENTHEPHAT100% (2)
- Catalogo Bombas y Motores Vickers PDFDocument26 pagesCatalogo Bombas y Motores Vickers PDFIvanDarioGuerreroFajardoNo ratings yet
- Chloride Corrosion Threshold of Reinforcing Steel in Alkaline Solutions-Open-Circuit Immersion TestsDocument10 pagesChloride Corrosion Threshold of Reinforcing Steel in Alkaline Solutions-Open-Circuit Immersion TestsshameekaNo ratings yet
- 2 Circuit - Up To 6 Compressor Controllers: D: 10 DIN RailDocument4 pages2 Circuit - Up To 6 Compressor Controllers: D: 10 DIN RailJoséTorresNo ratings yet
- Pythagorean Theorem in BusinessDocument4 pagesPythagorean Theorem in BusinessDeelanshiNo ratings yet
- Ais 048Document18 pagesAis 048Sriram NarayanNo ratings yet
- Laboratory Methods For Analyzing Monoclonal Proteins - UpToDateDocument50 pagesLaboratory Methods For Analyzing Monoclonal Proteins - UpToDatechali90No ratings yet
- Database AssignmentDocument3 pagesDatabase AssignmentkaybNo ratings yet
- Design and Implementation of A Software Result Processing and Transcript Generation SystemDocument7 pagesDesign and Implementation of A Software Result Processing and Transcript Generation SystemDinomarshal PezumNo ratings yet
- Rev1 90a 32beda Technical Man PDFDocument136 pagesRev1 90a 32beda Technical Man PDFDouglas SobralNo ratings yet
- Principles of Cooking Eggs - RecipesDocument3 pagesPrinciples of Cooking Eggs - RecipesCristelle Joyce BallicudNo ratings yet
- Coterminal Angles and Reference AnglesDocument3 pagesCoterminal Angles and Reference AnglesRaycelyn Joy CaburnayNo ratings yet