Download as pdf or txt
You might also like
- List of IDMA Members 2023Document46 pagesList of IDMA Members 2023Saddam Hussain50% (4)
- Confirmation of Satanding PDFDocument3 pagesConfirmation of Satanding PDFDavidForloyoNo ratings yet
- Cephalometrics For Orthognathic SurgeryDocument11 pagesCephalometrics For Orthognathic SurgeryGowri ShankarNo ratings yet
- Horizontal Condylar AngleDocument2 pagesHorizontal Condylar Angleسلمى صلاح100% (2)
- NHO Code of Practice For Healthcare Records Management Version 2 0Document370 pagesNHO Code of Practice For Healthcare Records Management Version 2 0Khirod SahuNo ratings yet
- Astrazeneca Strategy Is Targeted On Innovation With 3 Strategic PrioritiesDocument3 pagesAstrazeneca Strategy Is Targeted On Innovation With 3 Strategic PrioritiesAhmedAdnanNo ratings yet
- Discrepancies Between Arbitrary and True Hinge AxesDocument7 pagesDiscrepancies Between Arbitrary and True Hinge AxesNitin H.c.No ratings yet
- Variatm3Nsinlocalw3Nofam?Itwryand Truehingeaxispoints G. D.D.S., H. D.M.DDocument6 pagesVariatm3Nsinlocalw3Nofam?Itwryand Truehingeaxispoints G. D.D.S., H. D.M.DjaymitpatelNo ratings yet
- The Gothic Arch (Needle Point) Tracing and Condylar InclinationDocument5 pagesThe Gothic Arch (Needle Point) Tracing and Condylar InclinationPraveen KumarNo ratings yet
- Stoney-1988-American Journal of Physical AnthropologyDocument10 pagesStoney-1988-American Journal of Physical AnthropologyEmrah ÇAMNo ratings yet
- The Effect of Head Rotation On Cephalometric RadiographsDocument7 pagesThe Effect of Head Rotation On Cephalometric RadiographsDearma KhairunnisaNo ratings yet
- Lundeen, An Evaluation of Mandibular Border MovementsDocument11 pagesLundeen, An Evaluation of Mandibular Border MovementsFreddy BenalcázarNo ratings yet
- C of Spee RevisitedDocument5 pagesC of Spee RevisitedIndu SivakumarNo ratings yet
- Beck (1959)Document13 pagesBeck (1959)jorefe12No ratings yet
- Preston. A Reassessment of The Mandibular Transverse Horizontal Axis Theory. (1979)Document9 pagesPreston. A Reassessment of The Mandibular Transverse Horizontal Axis Theory. (1979)Jose Enrique AvilaNo ratings yet
- Podesser 2004Document7 pagesPodesser 2004Tien Li AnNo ratings yet
- Articularis Genus: An Anatomic and MRI Study in CadaversDocument9 pagesArticularis Genus: An Anatomic and MRI Study in CadaversFelipe SánchezNo ratings yet
- Operative Oral SurgeryDocument10 pagesOperative Oral SurgeryManuel Saúl Vicente CoasacaNo ratings yet
- Biomechanical PropertiesDocument5 pagesBiomechanical PropertiesMenthor555No ratings yet
- Cephalometric Appraisal of Antero-Posterior Skeletal Discrepancy: An OverviewDocument8 pagesCephalometric Appraisal of Antero-Posterior Skeletal Discrepancy: An OverviewAaditya MallikNo ratings yet
- The Effect of Projection Errors On Cephalometric Length MeasurementsDocument8 pagesThe Effect of Projection Errors On Cephalometric Length MeasurementsNeeraj AroraNo ratings yet
- The Effect of Projection Errors On Cephalometric Length MeasurementsDocument8 pagesThe Effect of Projection Errors On Cephalometric Length MeasurementsNeeraj AroraNo ratings yet
- Purcutaneous PinningDocument6 pagesPurcutaneous PinningGunjan PatilNo ratings yet
- Atlas c1Document5 pagesAtlas c1davorribicicNo ratings yet
- Jurnal 5Document7 pagesJurnal 5JAQUELINENo ratings yet
- Compressive Strength of Tibial Cancellous Bone Instron and Osteopenetrometer Measurements in An Autopsy MaterialDocument8 pagesCompressive Strength of Tibial Cancellous Bone Instron and Osteopenetrometer Measurements in An Autopsy MaterialsakhawatNo ratings yet
- Bare Olecranon PDFDocument6 pagesBare Olecranon PDFGhassen BouaouajaNo ratings yet
- Postgraduate Notes in Orthodontics-100-149Document50 pagesPostgraduate Notes in Orthodontics-100-149Mu'taz ArmanNo ratings yet
- 2004-Morphology of The Radial Head A Reverse Engineering Bases Evaluation Using Three-Dimensional Anatomical Data of Radial BoneDocument6 pages2004-Morphology of The Radial Head A Reverse Engineering Bases Evaluation Using Three-Dimensional Anatomical Data of Radial BonePongnarin JiamwatthanachaiNo ratings yet
- Aditya Tadinad Et Al: ResultsDocument1 pageAditya Tadinad Et Al: ResultsAPO KATNo ratings yet
- The Deltoid Muscle: An Anatomic Description of The Deltoid Insertion To The Proximal HumerusDocument3 pagesThe Deltoid Muscle: An Anatomic Description of The Deltoid Insertion To The Proximal HumerusDeepak NaiduNo ratings yet
- 1728 PDFDocument3 pages1728 PDFDeepak NaiduNo ratings yet
- Sub Men To VertexDocument10 pagesSub Men To Vertexvanefranco95No ratings yet
- Lauciello. Anatomic Comparison To Arbitrary Reference Notch On Hanau Articulators. (1978)Document6 pagesLauciello. Anatomic Comparison To Arbitrary Reference Notch On Hanau Articulators. (1978)Jose Enrique AvilaNo ratings yet
- A Method For Studying Knife Tool MarksDocument5 pagesA Method For Studying Knife Tool MarksWang EvanNo ratings yet
- Practical 3 FAO CRANIOMETRYDocument5 pagesPractical 3 FAO CRANIOMETRYparas.sharmaNo ratings yet
- Yochum and Rowe - Cap 2 PDFDocument119 pagesYochum and Rowe - Cap 2 PDFRICARDO LOPEZ FLORESNo ratings yet
- Screenshot 2023-04-15 at 6.21.50 PM PDFDocument22 pagesScreenshot 2023-04-15 at 6.21.50 PM PDFMustafa S. JaberNo ratings yet
- The Effect of Projection Errors On Angular Measurements in CephalometryDocument9 pagesThe Effect of Projection Errors On Angular Measurements in CephalometryNeeraj AroraNo ratings yet
- Ueki 2007Document7 pagesUeki 2007abhishekjha0082No ratings yet
- Hart N RoseDocument5 pagesHart N RoseRitika JangraNo ratings yet
- Approach To The Perpendicular Fixation of A Scaphoid Waist Fracture-A Computer Analyzed Cadaver ModelDocument10 pagesApproach To The Perpendicular Fixation of A Scaphoid Waist Fracture-A Computer Analyzed Cadaver ModelantoanetaNo ratings yet
- Ajo Agosto 06 Molares SupDocument6 pagesAjo Agosto 06 Molares SupHARITHA H.PNo ratings yet
- The Bennett Angle: Clinical Comparison of Different Recording MethodsDocument6 pagesThe Bennett Angle: Clinical Comparison of Different Recording MethodsFrank Bermeo100% (1)
- An Anatomical Study of The Acetabulum With Clinical Applications To Hip ArthrosDocument10 pagesAn Anatomical Study of The Acetabulum With Clinical Applications To Hip Arthrosharo.r9524No ratings yet
- Thomas Et Al-2013-Journal of Forensic SciencesDocument5 pagesThomas Et Al-2013-Journal of Forensic SciencesmacarenaNo ratings yet
- Ajr 2Document3 pagesAjr 2anon_302681452No ratings yet
- 02 Stephens - The Orthodontic Center of Rotation of The Maxillary IncisorDocument9 pages02 Stephens - The Orthodontic Center of Rotation of The Maxillary Incisorhu.alshattiNo ratings yet
- Convexidade RadicularDocument8 pagesConvexidade RadicularAlin OdorNo ratings yet
- Infraorbital Foramen Location in Dry Human Skulls: Macedo, VC., Cabrini, RR. and Faig-Leite, H.Document4 pagesInfraorbital Foramen Location in Dry Human Skulls: Macedo, VC., Cabrini, RR. and Faig-Leite, H.Eni Yulvia YantiNo ratings yet
- Infleunce of Group Function Canine Guidance On Elevator MuscleDocument8 pagesInfleunce of Group Function Canine Guidance On Elevator MuscleHossam BarghashNo ratings yet
- Pantographic Tracing of MovementsDocument8 pagesPantographic Tracing of MovementsPavithra balasubramaniNo ratings yet
- Between Session Reliability of Opto Electronic Motion Capture - 2018 - Journal oDocument5 pagesBetween Session Reliability of Opto Electronic Motion Capture - 2018 - Journal oRyuNo ratings yet
- J Jhsa 2014 12 025Document9 pagesJ Jhsa 2014 12 025Izan BallesterosNo ratings yet
- Article in Press: Orthopaedics & Traumatology: Surgery & ResearchDocument6 pagesArticle in Press: Orthopaedics & Traumatology: Surgery & ResearchAren BizdikianNo ratings yet
- Intra Observer and Inter Observer VariatDocument5 pagesIntra Observer and Inter Observer VariatSEPTIA SRI EKA PUTRINo ratings yet
- Classification of Articulators: Awni Rihani, D.D.S., M.Sc.Document4 pagesClassification of Articulators: Awni Rihani, D.D.S., M.Sc.Shanna MitchellNo ratings yet
- Al-Kayat and BramliDocument13 pagesAl-Kayat and BramliAshish Dadhania100% (1)
- Automated Accurate and Three Dimensional Method For Calc - 2018 - Journal of BDocument6 pagesAutomated Accurate and Three Dimensional Method For Calc - 2018 - Journal of BRyuNo ratings yet
- DOIS Smidt 1973Document15 pagesDOIS Smidt 1973GERARDO TORRES RUIZNo ratings yet
- An Atlas and Manual of Cef Alometric Rad PDFDocument226 pagesAn Atlas and Manual of Cef Alometric Rad PDFMonica Marcillia100% (1)
- Hollow Needle Tissue Insertion Force ModelDocument4 pagesHollow Needle Tissue Insertion Force Modelmohammadreza hajialiNo ratings yet
- Morphological Variation in a Population of the Snake, Tantilla gracilis Baird and GirardFrom EverandMorphological Variation in a Population of the Snake, Tantilla gracilis Baird and GirardNo ratings yet
- Clinical Maxillary Sinus Elevation SurgeryFrom EverandClinical Maxillary Sinus Elevation SurgeryDaniel W. K. KaoNo ratings yet
- Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudyDocument9 pagesDynamic Navigation in Dental Implantology: The Influence of Surgical Experience On Implant Placement Accuracy and Operating Time. An in Vitro StudySahana RangarajanNo ratings yet
- Mandibular MovementDocument56 pagesMandibular MovementSahana RangarajanNo ratings yet
- Clinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorDocument4 pagesClinical Report Rehabilitation of Maxillary Surgical Defect With A Cast Partial Denture ObturatorSahana RangarajanNo ratings yet
- Support in Complete DentureDocument16 pagesSupport in Complete DentureSahana RangarajanNo ratings yet
- Support in Complete DentureDocument30 pagesSupport in Complete DentureSahana Rangarajan100% (2)
- Different Types of Tooth PreparationDocument56 pagesDifferent Types of Tooth PreparationSahana Rangarajan100% (1)
- Factors Affecting Shade of All Ceramic Restorations - A Literature ReviewDocument8 pagesFactors Affecting Shade of All Ceramic Restorations - A Literature ReviewSahana RangarajanNo ratings yet
- Mouth Guards in Dentistry-A Review: September 2018Document6 pagesMouth Guards in Dentistry-A Review: September 2018Sahana RangarajanNo ratings yet
- Fulltext - Jda v5 Id1107Document3 pagesFulltext - Jda v5 Id1107Sahana RangarajanNo ratings yet
- Frankel Appliance Certified Fixed Orthodontic Courses by Indian Dental AcademyDocument76 pagesFrankel Appliance Certified Fixed Orthodontic Courses by Indian Dental AcademySahana RangarajanNo ratings yet
- 7 Shreeprada Dash IJPHRDDecember 2018 IssueDocument7 pages7 Shreeprada Dash IJPHRDDecember 2018 IssueSahana RangarajanNo ratings yet
- Finishing and Polishing Agents: - Presented by DR Arpita DuttaDocument89 pagesFinishing and Polishing Agents: - Presented by DR Arpita DuttaSahana RangarajanNo ratings yet
- A Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientDocument6 pagesA Hollow Bulb Obturator For Maxillary Resection in A Completely Edentulous PatientSahana RangarajanNo ratings yet
- 6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothDocument6 pages6.clinical Case ReportMultidisciplinary Approach For Rehabilitation of Debilitated Anterior ToothSahana RangarajanNo ratings yet
- 7 RetainerinorthodonticsDocument6 pages7 RetainerinorthodonticsSahana RangarajanNo ratings yet
- 3D Printing Industry Roadmap - India (Aerospace) Summit DocumentDocument19 pages3D Printing Industry Roadmap - India (Aerospace) Summit DocumentSahana RangarajanNo ratings yet
- Sauser 1957Document9 pagesSauser 1957Sahana RangarajanNo ratings yet
- Long-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthDocument7 pagesLong-Term Follow-Up of Maxillary Fixed Retention: Survival Rate and Periodontal HealthSahana RangarajanNo ratings yet
- Review: Types of Finish Lines or Gingival Margins Intooth PreparationDocument6 pagesReview: Types of Finish Lines or Gingival Margins Intooth PreparationSahana RangarajanNo ratings yet
- Significance of Facebow For Dental RestorationsDocument5 pagesSignificance of Facebow For Dental RestorationsSahana RangarajanNo ratings yet
- Elegant Galaxy Background Breakthrough by SlidesgoDocument48 pagesElegant Galaxy Background Breakthrough by SlidesgoSahana RangarajanNo ratings yet
- Gothic Arch TrachingDocument7 pagesGothic Arch TrachingSahana RangarajanNo ratings yet
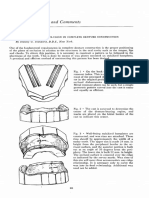
- Cases and Comments: by Stanley G. Standard, D.D.S., New YorkDocument3 pagesCases and Comments: by Stanley G. Standard, D.D.S., New YorkSahana RangarajanNo ratings yet
- Prosthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerDocument6 pagesProsthodontics Horizontal Jaw Relation: Dr. Firas AbdulameerSahana RangarajanNo ratings yet
- Embryology Review QuestionsDocument8 pagesEmbryology Review QuestionsMuhammad Azeem KhanNo ratings yet
- Memory and The Self: Martin A. ConwayDocument4 pagesMemory and The Self: Martin A. ConwaygusgauNo ratings yet
- Phardose Lab (Prep 6-10)Document3 pagesPhardose Lab (Prep 6-10)Jan Aira Almazan100% (1)
- Ketac Universal Aplicap TDS LTR 144iOSDocument8 pagesKetac Universal Aplicap TDS LTR 144iOSjaneNo ratings yet
- Spirometry Report Group-14Document11 pagesSpirometry Report Group-14Mwanja MosesNo ratings yet
- MSDS Citrox Misting Fog Ver 01 RTUDocument4 pagesMSDS Citrox Misting Fog Ver 01 RTUJainil Panchal100% (1)
- Seinfeld Syncope'': To The EditorDocument1 pageSeinfeld Syncope'': To The EditorJason ChambersNo ratings yet
- Federal Register PostDocument4 pagesFederal Register PostThe Western JournalNo ratings yet
- Frontal Bone& Frontal Sinus FractureDocument51 pagesFrontal Bone& Frontal Sinus Fracturetegegnegenet2No ratings yet
- AOA PresentationDocument11 pagesAOA Presentationreeves_coolNo ratings yet
- Noise Pollution and Our HealthDocument9 pagesNoise Pollution and Our HealthlouloubebeNo ratings yet
- Fdar Charting and Discharge PlanningDocument2 pagesFdar Charting and Discharge PlanningFaine Angela Caones100% (1)
- Proposal - Technology Innovation Sandbox PDFDocument25 pagesProposal - Technology Innovation Sandbox PDFhadyan hafizhNo ratings yet
- Drilling Soal Unair TBI Day 2Document13 pagesDrilling Soal Unair TBI Day 2Shinta BeslyNo ratings yet
- Before I Blame Myself and Feel Guilty: Upgrade To A Paid Plan ForDocument4 pagesBefore I Blame Myself and Feel Guilty: Upgrade To A Paid Plan ForкаринаNo ratings yet
- Francisco Vs Bahia Shipping ServicesDocument4 pagesFrancisco Vs Bahia Shipping ServicesJanice F. Cabalag-De VillaNo ratings yet
- Co DiovanDocument8 pagesCo DiovanPeter Rey Tanio TeopeNo ratings yet
- Problem-Based Learning in Medicine and Beyond: A Brief: Howard S. BarrowsDocument11 pagesProblem-Based Learning in Medicine and Beyond: A Brief: Howard S. BarrowsRobby AgungNo ratings yet
- Depot-Ped: 3 Months: 11.25 MG or 30 MG Q12weeks. (SQ) Lupron: Children: Initially, 50Document3 pagesDepot-Ped: 3 Months: 11.25 MG or 30 MG Q12weeks. (SQ) Lupron: Children: Initially, 50thuey epeNo ratings yet
- NCSBN - Pharmacology and ParenteralDocument36 pagesNCSBN - Pharmacology and ParenteralKarissa May Cortez92% (12)
- UGC-Regulation Min Qualification Jul2018Document4 pagesUGC-Regulation Min Qualification Jul2018pundirv1993No ratings yet
- Module 4. Leadership in NursingDocument33 pagesModule 4. Leadership in NursingSang Hyun JungNo ratings yet
- Mark E. Locklear ResumeDocument5 pagesMark E. Locklear ResumeMark LocklearNo ratings yet
- Product Safety Data Sheet: Body Scrub Lulur Green Tea Issued: May 2019Document2 pagesProduct Safety Data Sheet: Body Scrub Lulur Green Tea Issued: May 2019emyNo ratings yet
- Clinical Profile and Outcome of Myasthenic CrisisDocument13 pagesClinical Profile and Outcome of Myasthenic CrisissyahriniNo ratings yet
- Hubungan Berat Badan Lahir Rendah (BBLR) Dengan Kejadian Stunting Pada Anak Usia 1-3 TahunDocument6 pagesHubungan Berat Badan Lahir Rendah (BBLR) Dengan Kejadian Stunting Pada Anak Usia 1-3 TahunMusdalifa IfhaaNo ratings yet