
Immunopathogenesis of Pulmonary Granulomas
Immunopathogenesis of Pulmonary Granulomas
You might also like
- Amoeba Sisters Video Recap: ATPDocument2 pagesAmoeba Sisters Video Recap: ATPCaptain Marvel33% (3)
- Coronavirus Replication and Reverse Genetics (Current Topics in Microbiology and Immunology) PDFDocument261 pagesCoronavirus Replication and Reverse Genetics (Current Topics in Microbiology and Immunology) PDFasmonovNo ratings yet
- Embryology MCQsDocument7 pagesEmbryology MCQsSafiya James100% (2)
- Granuloma TuberculosisDocument9 pagesGranuloma TuberculosisÁlvaro Alexandro Morales JiménezNo ratings yet
- Cambier 2014Document13 pagesCambier 2014chaudhurysandip18No ratings yet
- Research Papers On KlebsiellaDocument8 pagesResearch Papers On Klebsiellagzrvpcvnd100% (1)
- Jciinsight 5 136937Document18 pagesJciinsight 5 136937Nur AnisaNo ratings yet
- Sporulation in MycobacteriaDocument6 pagesSporulation in MycobacteriaGUIDO ERNESTO VILLOTA CALVACHINo ratings yet
- Genoma TBDocument14 pagesGenoma TBMARIO CASTRONo ratings yet
- Lophomonas Blattarum Infection or Just The Movement of Ciliated Epithelial Cells?Document4 pagesLophomonas Blattarum Infection or Just The Movement of Ciliated Epithelial Cells?AxelWarnerNo ratings yet
- A Mouse Model of Ovalbumin Allergen Accumulation of Peribronchial Mast Cells inDocument9 pagesA Mouse Model of Ovalbumin Allergen Accumulation of Peribronchial Mast Cells inEduardo MendesNo ratings yet
- Lung Involvement in Childhood Measles: Severe Immune Dysfunction Revealed by Quantitative ImmunohistochemistryDocument10 pagesLung Involvement in Childhood Measles: Severe Immune Dysfunction Revealed by Quantitative Immunohistochemistryapi-286128974No ratings yet
- Ni Hms 747150Document26 pagesNi Hms 747150nydiacastillom2268No ratings yet
- Infections of M. PneumoniaeDocument18 pagesInfections of M. PneumoniaeAndrés Nicolás Beltrán SeguraNo ratings yet
- Canan 2014 JLBDocument1 pageCanan 2014 JLBNandan GokhaleNo ratings yet
- Blrincon - Bacterias Inmune ResponseDocument9 pagesBlrincon - Bacterias Inmune ResponseDavidf VillabonaNo ratings yet
- Basic Concepts in Lung Immunology: System ThatDocument6 pagesBasic Concepts in Lung Immunology: System ThatAnailil MoralesNo ratings yet
- Pathophysiology of Tuberculosis: An Update Review: January 2018Document8 pagesPathophysiology of Tuberculosis: An Update Review: January 2018Dedi IdNo ratings yet
- Pathophysiology of Tuberculosis: An Update Review: Pharmatutor January 2018Document8 pagesPathophysiology of Tuberculosis: An Update Review: Pharmatutor January 2018Michael HusainNo ratings yet
- Coronaviruses - Medical Microbiology - NCBI BookshelfDocument4 pagesCoronaviruses - Medical Microbiology - NCBI BookshelfMudoogoEdgarNo ratings yet
- Crossm: The Brief Case: Disseminated Histoplasma Capsulatum in A Patient With Newly Diagnosed HIV Infection/AIDSDocument5 pagesCrossm: The Brief Case: Disseminated Histoplasma Capsulatum in A Patient With Newly Diagnosed HIV Infection/AIDSanggoenzNo ratings yet
- MSX 173Document18 pagesMSX 173utpalmtbiNo ratings yet
- Helmintos TisularesDocument8 pagesHelmintos TisularesValentina Arenas RNo ratings yet
- Review On Tuber CL Us Is Pharma TutorDocument8 pagesReview On Tuber CL Us Is Pharma TutorBrilian WulansariNo ratings yet
- Jurnal Vaksin BCG 2Document9 pagesJurnal Vaksin BCG 2niken ambarNo ratings yet
- Pathophysiology of Tuberculosis: An Update Review: January 2018Document8 pagesPathophysiology of Tuberculosis: An Update Review: January 2018Arvin AlfariziNo ratings yet
- Meningitis Por Angiostrongilus Cantonensis 12974 - 2018 - Article - 1071Document13 pagesMeningitis Por Angiostrongilus Cantonensis 12974 - 2018 - Article - 1071Cristhian RuizNo ratings yet
- Development of The Avian Immune System: October 2013Document20 pagesDevelopment of The Avian Immune System: October 2013Ferdinand Prayogo Cahyo SantosoNo ratings yet
- Chapter 56Document57 pagesChapter 56Rahmat MuliaNo ratings yet
- Within-Host Microevolution of Streptococcus Pneumoniae Is Rapid and Adaptive During Natural Colonisation - 2020 Nature ResearchDocument14 pagesWithin-Host Microevolution of Streptococcus Pneumoniae Is Rapid and Adaptive During Natural Colonisation - 2020 Nature ResearchTony NgNo ratings yet
- Aspergillus Fumigatus Triggers Inflammatory Response in Stage Specific Beta Glucan DisplayDocument9 pagesAspergillus Fumigatus Triggers Inflammatory Response in Stage Specific Beta Glucan Displaymumu_sukiNo ratings yet
- Journal Ppat 1008404 PDFDocument18 pagesJournal Ppat 1008404 PDFVictoria AceboNo ratings yet
- Streptococcus Pneumoniae: Invasion and in Ammation: Allister J. Loughran, Carlos J. Orihuela, and Elaine I. TuomanenDocument18 pagesStreptococcus Pneumoniae: Invasion and in Ammation: Allister J. Loughran, Carlos J. Orihuela, and Elaine I. TuomanenSantiago Basto CruzNo ratings yet
- State of The Art: A Brave New World: The Lung Microbiota in An Era of ChangeDocument7 pagesState of The Art: A Brave New World: The Lung Microbiota in An Era of ChangeImha MikanersandsmashblastNo ratings yet
- Flynn Et Al 2013 Interaction of Mycobacterium Leprae With Human Airway Epithelial Cells Adherence Entry Survival andDocument15 pagesFlynn Et Al 2013 Interaction of Mycobacterium Leprae With Human Airway Epithelial Cells Adherence Entry Survival anddamayantiwenny24No ratings yet
- Vet Pathol 2013 Delaney 172 6 DolphinDocument6 pagesVet Pathol 2013 Delaney 172 6 DolphinKhairul Ihsan Pengusaha MudaNo ratings yet
- Pneumocystis Pneumonia: CariniiDocument10 pagesPneumocystis Pneumonia: CariniiDiana GhawaNo ratings yet
- Salmonella Typhi: From A Human Pathogen To A Vaccine Vector: Cellular & Molecular Immunology May 2008Document8 pagesSalmonella Typhi: From A Human Pathogen To A Vaccine Vector: Cellular & Molecular Immunology May 2008noordin MukasaNo ratings yet
- PatogenesisDocument28 pagesPatogenesisOka WidyaningsihNo ratings yet
- J Immunol 2002 Greenwell Wild 6286 97Document13 pagesJ Immunol 2002 Greenwell Wild 6286 97noork85No ratings yet
- Pa Tho Genesis and Immunology of Avian InfluenzaDocument9 pagesPa Tho Genesis and Immunology of Avian InfluenzaHengki FerdiantoNo ratings yet
- NEJMcibr 0902539Document3 pagesNEJMcibr 0902539Karen CatariNo ratings yet
- Jci 133 173156Document11 pagesJci 133 173156Dhivya l.sNo ratings yet
- Immunity Against Fungi: Michail S. Lionakis, Iliyan D. Iliev, and Tobias M. HohlDocument17 pagesImmunity Against Fungi: Michail S. Lionakis, Iliyan D. Iliev, and Tobias M. HohlFajar SukmajayaNo ratings yet
- Medical ImmunologyDocument10 pagesMedical ImmunologyPriyaatarishini ArumughamNo ratings yet
- 287 Current Topics in Microbiology and ImmunologyDocument8 pages287 Current Topics in Microbiology and ImmunologyKKNo ratings yet
- Proofs EuJMI 03 258Document10 pagesProofs EuJMI 03 258rizgah jawasNo ratings yet
- Jimmunol 1202354Document15 pagesJimmunol 1202354everton.monteiroNo ratings yet
- Journal of Virology-2010-Graham-3134.fullDocument13 pagesJournal of Virology-2010-Graham-3134.fullJohn WilliamsonNo ratings yet
- Fibrosis Quística y Enfermedad PulmonarDocument9 pagesFibrosis Quística y Enfermedad PulmonarMELERYN CRISTY VELASQUEZ MOSTACERONo ratings yet
- TB PDFDocument12 pagesTB PDFHana AshrafNo ratings yet
- TMP D096Document32 pagesTMP D096FrontiersNo ratings yet
- Presternal Scrofuloderma in A HIV Infected Patient Case Report and Discussion of The Literature DataDocument5 pagesPresternal Scrofuloderma in A HIV Infected Patient Case Report and Discussion of The Literature DataAthenaeum Scientific PublishersNo ratings yet
- Nanoparticle Adjuvant Sensing by Tlr7 Enhances Cd8 T Cell Mediated Protection From Listeria Monocytogenes InfectionDocument9 pagesNanoparticle Adjuvant Sensing by Tlr7 Enhances Cd8 T Cell Mediated Protection From Listeria Monocytogenes InfectionEverton MonteiroNo ratings yet
- Microevolution of Helicobacter Pylori During Prolonged Infection of Single Hosts and Within FamiliesDocument13 pagesMicroevolution of Helicobacter Pylori During Prolonged Infection of Single Hosts and Within FamiliesReza Panji SusantoNo ratings yet
- tmpBF53 TMPDocument6 pagestmpBF53 TMPFrontiersNo ratings yet
- Artculo1 PDFDocument15 pagesArtculo1 PDFRia Risca PratiwiNo ratings yet
- Scribd On AppstoreScribd On Google Play © Copyright 2015 Scribd Inc. Mobile Site Language English ScribdDocument33 pagesScribd On AppstoreScribd On Google Play © Copyright 2015 Scribd Inc. Mobile Site Language English ScribdMokhammad Faisol AbdullahNo ratings yet
- A Mathematical Model For Cellular Immunology of TuberculosisDocument15 pagesA Mathematical Model For Cellular Immunology of TuberculosisRia Risca PratiwiNo ratings yet
- Functional and Phenotypic Changes in Monocytes From Patients With Tuberculosis Are Reversed With TreatmentDocument9 pagesFunctional and Phenotypic Changes in Monocytes From Patients With Tuberculosis Are Reversed With TreatmentCecile E EcheverríaNo ratings yet
- M Gen 000102Document15 pagesM Gen 000102miaNo ratings yet
- Efectele Speciilor Reactive de Oxigen Asupra Sistemului de Reproducere FemininDocument8 pagesEfectele Speciilor Reactive de Oxigen Asupra Sistemului de Reproducere FemininLuminita HutanuNo ratings yet
- BIOCELLDocument81 pagesBIOCELLAchraf RbNo ratings yet
- CH19 Patho D&R AgamDocument21 pagesCH19 Patho D&R Agam062No ratings yet
- Cotton Production Guideline PDFDocument32 pagesCotton Production Guideline PDFEvans Katuta Mpundu Jr.No ratings yet
- Mcqs of PsychologyDocument45 pagesMcqs of PsychologyAHSAN JUTTNo ratings yet
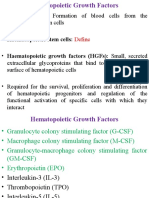
- Hematopoiesis and Growth FactorsDocument17 pagesHematopoiesis and Growth FactorsEmma Joel OtaiNo ratings yet
- Iponatic®: Portable Molecule Workstation (4 Modules)Document2 pagesIponatic®: Portable Molecule Workstation (4 Modules)abhinaya baskaranNo ratings yet
- GT134 DamsDocument119 pagesGT134 Damsসোমনাথ মহাপাত্র0% (1)
- RT-PCR Test Result SintuGuptaDocument1 pageRT-PCR Test Result SintuGuptaNitesh TiwariNo ratings yet
- Selina Solutions For Class 9 Biology Chapter 5 Pollination and FertilizationDocument10 pagesSelina Solutions For Class 9 Biology Chapter 5 Pollination and Fertilizationmovies gamesNo ratings yet
- Haa Nipa Question Bank (Proposed) - FinalDocument3 pagesHaa Nipa Question Bank (Proposed) - FinalZahidul HassanNo ratings yet
- MDRO A Review 2019Document9 pagesMDRO A Review 2019Muhammad Dody HermawanNo ratings yet
- Chapter 13 Section 1-2 Study StationsDocument9 pagesChapter 13 Section 1-2 Study StationsBao HoangNo ratings yet
- Pedigrees Lesson For November 9thDocument3 pagesPedigrees Lesson For November 9thnataNo ratings yet
- BG. 6 - Semester (Batch: 2018) : Session:2020-21: (Timetable: BSC-BSCN)Document2 pagesBG. 6 - Semester (Batch: 2018) : Session:2020-21: (Timetable: BSC-BSCN)Narayan BarmanNo ratings yet
- GDR - Poc Update (01.07.21)Document2 pagesGDR - Poc Update (01.07.21)Dr ThietNo ratings yet
- GPB 321 Crop Improvement Manual FinalDocument71 pagesGPB 321 Crop Improvement Manual FinalSultan AhmadNo ratings yet
- Unit 9 ReviewDocument4 pagesUnit 9 Reviewkarissamai24No ratings yet
- QCMDL 21 51393 Relata Leonardo NacionalDocument1 pageQCMDL 21 51393 Relata Leonardo NacionalAngel DetablanNo ratings yet
- Unit 7: Genes and Inheritance Lesson 7.1: Chromosomes, Genes and DNADocument44 pagesUnit 7: Genes and Inheritance Lesson 7.1: Chromosomes, Genes and DNAhypezakramNo ratings yet
- January 2022 (IAL) QPDocument28 pagesJanuary 2022 (IAL) QPMaria Shabbir PanjiwalaNo ratings yet
- Lume Screen-Ncov: 13814010 (Real Time Rt-Lamp Covid 19 Testing Kit)Document2 pagesLume Screen-Ncov: 13814010 (Real Time Rt-Lamp Covid 19 Testing Kit)N. K. MandilNo ratings yet
- Hematogones With Light Chain Restriction A Potential Diagnostic PitfallDocument9 pagesHematogones With Light Chain Restriction A Potential Diagnostic Pitfallimran ahmed siddiquiNo ratings yet
- The Human Machine by RL Bijlani, SK ManchandaDocument176 pagesThe Human Machine by RL Bijlani, SK ManchandaMUSKANNo ratings yet
- Introduction To Microbiology and ParasitologyDocument26 pagesIntroduction To Microbiology and ParasitologyORTUOSTE ARIELLE ANNNo ratings yet
- Epigenesis To EpigeneticsDocument38 pagesEpigenesis To EpigeneticsAditi DasNo ratings yet
- Psychology Mcqs Class 12 NewDocument5 pagesPsychology Mcqs Class 12 NewAkshita BatraNo ratings yet
- Evolutionary Biology A Plant Perspective Mitchell B Cruzan Full ChapterDocument67 pagesEvolutionary Biology A Plant Perspective Mitchell B Cruzan Full Chaptervivian.arriola772100% (3)
























































































Download as pdf or txt
You might also like
- Amoeba Sisters Video Recap: ATPDocument2 pagesAmoeba Sisters Video Recap: ATPCaptain Marvel33% (3)
- Coronavirus Replication and Reverse Genetics (Current Topics in Microbiology and Immunology) PDFDocument261 pagesCoronavirus Replication and Reverse Genetics (Current Topics in Microbiology and Immunology) PDFasmonovNo ratings yet
- Embryology MCQsDocument7 pagesEmbryology MCQsSafiya James100% (2)
- Granuloma TuberculosisDocument9 pagesGranuloma TuberculosisÁlvaro Alexandro Morales JiménezNo ratings yet
- Cambier 2014Document13 pagesCambier 2014chaudhurysandip18No ratings yet
- Research Papers On KlebsiellaDocument8 pagesResearch Papers On Klebsiellagzrvpcvnd100% (1)
- Jciinsight 5 136937Document18 pagesJciinsight 5 136937Nur AnisaNo ratings yet
- Sporulation in MycobacteriaDocument6 pagesSporulation in MycobacteriaGUIDO ERNESTO VILLOTA CALVACHINo ratings yet
- Genoma TBDocument14 pagesGenoma TBMARIO CASTRONo ratings yet
- Lophomonas Blattarum Infection or Just The Movement of Ciliated Epithelial Cells?Document4 pagesLophomonas Blattarum Infection or Just The Movement of Ciliated Epithelial Cells?AxelWarnerNo ratings yet
- A Mouse Model of Ovalbumin Allergen Accumulation of Peribronchial Mast Cells inDocument9 pagesA Mouse Model of Ovalbumin Allergen Accumulation of Peribronchial Mast Cells inEduardo MendesNo ratings yet
- Lung Involvement in Childhood Measles: Severe Immune Dysfunction Revealed by Quantitative ImmunohistochemistryDocument10 pagesLung Involvement in Childhood Measles: Severe Immune Dysfunction Revealed by Quantitative Immunohistochemistryapi-286128974No ratings yet
- Ni Hms 747150Document26 pagesNi Hms 747150nydiacastillom2268No ratings yet
- Infections of M. PneumoniaeDocument18 pagesInfections of M. PneumoniaeAndrés Nicolás Beltrán SeguraNo ratings yet
- Canan 2014 JLBDocument1 pageCanan 2014 JLBNandan GokhaleNo ratings yet
- Blrincon - Bacterias Inmune ResponseDocument9 pagesBlrincon - Bacterias Inmune ResponseDavidf VillabonaNo ratings yet
- Basic Concepts in Lung Immunology: System ThatDocument6 pagesBasic Concepts in Lung Immunology: System ThatAnailil MoralesNo ratings yet
- Pathophysiology of Tuberculosis: An Update Review: January 2018Document8 pagesPathophysiology of Tuberculosis: An Update Review: January 2018Dedi IdNo ratings yet
- Pathophysiology of Tuberculosis: An Update Review: Pharmatutor January 2018Document8 pagesPathophysiology of Tuberculosis: An Update Review: Pharmatutor January 2018Michael HusainNo ratings yet
- Coronaviruses - Medical Microbiology - NCBI BookshelfDocument4 pagesCoronaviruses - Medical Microbiology - NCBI BookshelfMudoogoEdgarNo ratings yet
- Crossm: The Brief Case: Disseminated Histoplasma Capsulatum in A Patient With Newly Diagnosed HIV Infection/AIDSDocument5 pagesCrossm: The Brief Case: Disseminated Histoplasma Capsulatum in A Patient With Newly Diagnosed HIV Infection/AIDSanggoenzNo ratings yet
- MSX 173Document18 pagesMSX 173utpalmtbiNo ratings yet
- Helmintos TisularesDocument8 pagesHelmintos TisularesValentina Arenas RNo ratings yet
- Review On Tuber CL Us Is Pharma TutorDocument8 pagesReview On Tuber CL Us Is Pharma TutorBrilian WulansariNo ratings yet
- Jurnal Vaksin BCG 2Document9 pagesJurnal Vaksin BCG 2niken ambarNo ratings yet
- Pathophysiology of Tuberculosis: An Update Review: January 2018Document8 pagesPathophysiology of Tuberculosis: An Update Review: January 2018Arvin AlfariziNo ratings yet
- Meningitis Por Angiostrongilus Cantonensis 12974 - 2018 - Article - 1071Document13 pagesMeningitis Por Angiostrongilus Cantonensis 12974 - 2018 - Article - 1071Cristhian RuizNo ratings yet
- Development of The Avian Immune System: October 2013Document20 pagesDevelopment of The Avian Immune System: October 2013Ferdinand Prayogo Cahyo SantosoNo ratings yet
- Chapter 56Document57 pagesChapter 56Rahmat MuliaNo ratings yet
- Within-Host Microevolution of Streptococcus Pneumoniae Is Rapid and Adaptive During Natural Colonisation - 2020 Nature ResearchDocument14 pagesWithin-Host Microevolution of Streptococcus Pneumoniae Is Rapid and Adaptive During Natural Colonisation - 2020 Nature ResearchTony NgNo ratings yet
- Aspergillus Fumigatus Triggers Inflammatory Response in Stage Specific Beta Glucan DisplayDocument9 pagesAspergillus Fumigatus Triggers Inflammatory Response in Stage Specific Beta Glucan Displaymumu_sukiNo ratings yet
- Journal Ppat 1008404 PDFDocument18 pagesJournal Ppat 1008404 PDFVictoria AceboNo ratings yet
- Streptococcus Pneumoniae: Invasion and in Ammation: Allister J. Loughran, Carlos J. Orihuela, and Elaine I. TuomanenDocument18 pagesStreptococcus Pneumoniae: Invasion and in Ammation: Allister J. Loughran, Carlos J. Orihuela, and Elaine I. TuomanenSantiago Basto CruzNo ratings yet
- State of The Art: A Brave New World: The Lung Microbiota in An Era of ChangeDocument7 pagesState of The Art: A Brave New World: The Lung Microbiota in An Era of ChangeImha MikanersandsmashblastNo ratings yet
- Flynn Et Al 2013 Interaction of Mycobacterium Leprae With Human Airway Epithelial Cells Adherence Entry Survival andDocument15 pagesFlynn Et Al 2013 Interaction of Mycobacterium Leprae With Human Airway Epithelial Cells Adherence Entry Survival anddamayantiwenny24No ratings yet
- Vet Pathol 2013 Delaney 172 6 DolphinDocument6 pagesVet Pathol 2013 Delaney 172 6 DolphinKhairul Ihsan Pengusaha MudaNo ratings yet
- Pneumocystis Pneumonia: CariniiDocument10 pagesPneumocystis Pneumonia: CariniiDiana GhawaNo ratings yet
- Salmonella Typhi: From A Human Pathogen To A Vaccine Vector: Cellular & Molecular Immunology May 2008Document8 pagesSalmonella Typhi: From A Human Pathogen To A Vaccine Vector: Cellular & Molecular Immunology May 2008noordin MukasaNo ratings yet
- PatogenesisDocument28 pagesPatogenesisOka WidyaningsihNo ratings yet
- J Immunol 2002 Greenwell Wild 6286 97Document13 pagesJ Immunol 2002 Greenwell Wild 6286 97noork85No ratings yet
- Pa Tho Genesis and Immunology of Avian InfluenzaDocument9 pagesPa Tho Genesis and Immunology of Avian InfluenzaHengki FerdiantoNo ratings yet
- NEJMcibr 0902539Document3 pagesNEJMcibr 0902539Karen CatariNo ratings yet
- Jci 133 173156Document11 pagesJci 133 173156Dhivya l.sNo ratings yet
- Immunity Against Fungi: Michail S. Lionakis, Iliyan D. Iliev, and Tobias M. HohlDocument17 pagesImmunity Against Fungi: Michail S. Lionakis, Iliyan D. Iliev, and Tobias M. HohlFajar SukmajayaNo ratings yet
- Medical ImmunologyDocument10 pagesMedical ImmunologyPriyaatarishini ArumughamNo ratings yet
- 287 Current Topics in Microbiology and ImmunologyDocument8 pages287 Current Topics in Microbiology and ImmunologyKKNo ratings yet
- Proofs EuJMI 03 258Document10 pagesProofs EuJMI 03 258rizgah jawasNo ratings yet
- Jimmunol 1202354Document15 pagesJimmunol 1202354everton.monteiroNo ratings yet
- Journal of Virology-2010-Graham-3134.fullDocument13 pagesJournal of Virology-2010-Graham-3134.fullJohn WilliamsonNo ratings yet
- Fibrosis Quística y Enfermedad PulmonarDocument9 pagesFibrosis Quística y Enfermedad PulmonarMELERYN CRISTY VELASQUEZ MOSTACERONo ratings yet
- TB PDFDocument12 pagesTB PDFHana AshrafNo ratings yet
- TMP D096Document32 pagesTMP D096FrontiersNo ratings yet
- Presternal Scrofuloderma in A HIV Infected Patient Case Report and Discussion of The Literature DataDocument5 pagesPresternal Scrofuloderma in A HIV Infected Patient Case Report and Discussion of The Literature DataAthenaeum Scientific PublishersNo ratings yet
- Nanoparticle Adjuvant Sensing by Tlr7 Enhances Cd8 T Cell Mediated Protection From Listeria Monocytogenes InfectionDocument9 pagesNanoparticle Adjuvant Sensing by Tlr7 Enhances Cd8 T Cell Mediated Protection From Listeria Monocytogenes InfectionEverton MonteiroNo ratings yet
- Microevolution of Helicobacter Pylori During Prolonged Infection of Single Hosts and Within FamiliesDocument13 pagesMicroevolution of Helicobacter Pylori During Prolonged Infection of Single Hosts and Within FamiliesReza Panji SusantoNo ratings yet
- tmpBF53 TMPDocument6 pagestmpBF53 TMPFrontiersNo ratings yet
- Artculo1 PDFDocument15 pagesArtculo1 PDFRia Risca PratiwiNo ratings yet
- Scribd On AppstoreScribd On Google Play © Copyright 2015 Scribd Inc. Mobile Site Language English ScribdDocument33 pagesScribd On AppstoreScribd On Google Play © Copyright 2015 Scribd Inc. Mobile Site Language English ScribdMokhammad Faisol AbdullahNo ratings yet
- A Mathematical Model For Cellular Immunology of TuberculosisDocument15 pagesA Mathematical Model For Cellular Immunology of TuberculosisRia Risca PratiwiNo ratings yet
- Functional and Phenotypic Changes in Monocytes From Patients With Tuberculosis Are Reversed With TreatmentDocument9 pagesFunctional and Phenotypic Changes in Monocytes From Patients With Tuberculosis Are Reversed With TreatmentCecile E EcheverríaNo ratings yet
- M Gen 000102Document15 pagesM Gen 000102miaNo ratings yet
- Efectele Speciilor Reactive de Oxigen Asupra Sistemului de Reproducere FemininDocument8 pagesEfectele Speciilor Reactive de Oxigen Asupra Sistemului de Reproducere FemininLuminita HutanuNo ratings yet
- BIOCELLDocument81 pagesBIOCELLAchraf RbNo ratings yet
- CH19 Patho D&R AgamDocument21 pagesCH19 Patho D&R Agam062No ratings yet
- Cotton Production Guideline PDFDocument32 pagesCotton Production Guideline PDFEvans Katuta Mpundu Jr.No ratings yet
- Mcqs of PsychologyDocument45 pagesMcqs of PsychologyAHSAN JUTTNo ratings yet
- Hematopoiesis and Growth FactorsDocument17 pagesHematopoiesis and Growth FactorsEmma Joel OtaiNo ratings yet
- Iponatic®: Portable Molecule Workstation (4 Modules)Document2 pagesIponatic®: Portable Molecule Workstation (4 Modules)abhinaya baskaranNo ratings yet
- GT134 DamsDocument119 pagesGT134 Damsসোমনাথ মহাপাত্র0% (1)
- RT-PCR Test Result SintuGuptaDocument1 pageRT-PCR Test Result SintuGuptaNitesh TiwariNo ratings yet
- Selina Solutions For Class 9 Biology Chapter 5 Pollination and FertilizationDocument10 pagesSelina Solutions For Class 9 Biology Chapter 5 Pollination and Fertilizationmovies gamesNo ratings yet
- Haa Nipa Question Bank (Proposed) - FinalDocument3 pagesHaa Nipa Question Bank (Proposed) - FinalZahidul HassanNo ratings yet
- MDRO A Review 2019Document9 pagesMDRO A Review 2019Muhammad Dody HermawanNo ratings yet
- Chapter 13 Section 1-2 Study StationsDocument9 pagesChapter 13 Section 1-2 Study StationsBao HoangNo ratings yet
- Pedigrees Lesson For November 9thDocument3 pagesPedigrees Lesson For November 9thnataNo ratings yet
- BG. 6 - Semester (Batch: 2018) : Session:2020-21: (Timetable: BSC-BSCN)Document2 pagesBG. 6 - Semester (Batch: 2018) : Session:2020-21: (Timetable: BSC-BSCN)Narayan BarmanNo ratings yet
- GDR - Poc Update (01.07.21)Document2 pagesGDR - Poc Update (01.07.21)Dr ThietNo ratings yet
- GPB 321 Crop Improvement Manual FinalDocument71 pagesGPB 321 Crop Improvement Manual FinalSultan AhmadNo ratings yet
- Unit 9 ReviewDocument4 pagesUnit 9 Reviewkarissamai24No ratings yet
- QCMDL 21 51393 Relata Leonardo NacionalDocument1 pageQCMDL 21 51393 Relata Leonardo NacionalAngel DetablanNo ratings yet
- Unit 7: Genes and Inheritance Lesson 7.1: Chromosomes, Genes and DNADocument44 pagesUnit 7: Genes and Inheritance Lesson 7.1: Chromosomes, Genes and DNAhypezakramNo ratings yet
- January 2022 (IAL) QPDocument28 pagesJanuary 2022 (IAL) QPMaria Shabbir PanjiwalaNo ratings yet
- Lume Screen-Ncov: 13814010 (Real Time Rt-Lamp Covid 19 Testing Kit)Document2 pagesLume Screen-Ncov: 13814010 (Real Time Rt-Lamp Covid 19 Testing Kit)N. K. MandilNo ratings yet
- Hematogones With Light Chain Restriction A Potential Diagnostic PitfallDocument9 pagesHematogones With Light Chain Restriction A Potential Diagnostic Pitfallimran ahmed siddiquiNo ratings yet
- The Human Machine by RL Bijlani, SK ManchandaDocument176 pagesThe Human Machine by RL Bijlani, SK ManchandaMUSKANNo ratings yet
- Introduction To Microbiology and ParasitologyDocument26 pagesIntroduction To Microbiology and ParasitologyORTUOSTE ARIELLE ANNNo ratings yet
- Epigenesis To EpigeneticsDocument38 pagesEpigenesis To EpigeneticsAditi DasNo ratings yet
- Psychology Mcqs Class 12 NewDocument5 pagesPsychology Mcqs Class 12 NewAkshita BatraNo ratings yet
- Evolutionary Biology A Plant Perspective Mitchell B Cruzan Full ChapterDocument67 pagesEvolutionary Biology A Plant Perspective Mitchell B Cruzan Full Chaptervivian.arriola772100% (3)