Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- PMP Cheat Sheet PDFDocument1 pagePMP Cheat Sheet PDFthouartu77% (35)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Italian Music Terms ListDocument18 pagesItalian Music Terms ListJoven MagbanuaNo ratings yet
- Visual Acuity ConversionDocument1 pageVisual Acuity Conversionreza arlasNo ratings yet
- Westborg 2017Document6 pagesWestborg 2017reza arlasNo ratings yet
- Wang-Douglas2020 ReferenceWorkEntry ThyroidEyeDiseaseDocument21 pagesWang-Douglas2020 ReferenceWorkEntry ThyroidEyeDiseasereza arlasNo ratings yet
- Lau 2018Document4 pagesLau 2018reza arlasNo ratings yet
- Thyroid Eye DiseaseDocument162 pagesThyroid Eye Diseasereza arlasNo ratings yet
- Flynn 2017Document17 pagesFlynn 2017reza arlasNo ratings yet
- Green 2018Document6 pagesGreen 2018reza arlasNo ratings yet
- Corneal Colagen PDFDocument185 pagesCorneal Colagen PDFreza arlasNo ratings yet
- Rose K2 XL Special OptionsDocument4 pagesRose K2 XL Special Optionsreza arlasNo ratings yet
- Introduction About Activated CarbonDocument46 pagesIntroduction About Activated CarbonPam Adriano DumasNo ratings yet
- Machine Design - INHOUSE 3Document28 pagesMachine Design - INHOUSE 3Pia May Torres PablicoNo ratings yet
- ParacetamolDocument2 pagesParacetamolDanielle PayneNo ratings yet
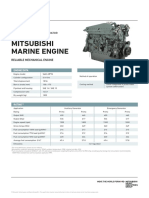
- Mitsubishi Marine Engine - S6A3-MPTADocument2 pagesMitsubishi Marine Engine - S6A3-MPTAEsmaeil RahmaniNo ratings yet
- Multi-Objective Design Optimization of Five-Phase Fractional-Slot Concentrated-Winding Surface-Mounted Permanent-Magnet MachineDocument17 pagesMulti-Objective Design Optimization of Five-Phase Fractional-Slot Concentrated-Winding Surface-Mounted Permanent-Magnet MachineNguyen Van QuyenNo ratings yet
- Roller Coaster SImulationDocument75 pagesRoller Coaster SImulationSAMEER ALI KHANNo ratings yet
- Master Thesis Low Noise AmplifierDocument8 pagesMaster Thesis Low Noise Amplifierdwfp5m7d100% (2)
- C136W14E2Document18 pagesC136W14E2diamono794No ratings yet
- HSDPA MC Inter DU Joint Scheduling: User GuideDocument59 pagesHSDPA MC Inter DU Joint Scheduling: User GuideNadira Chikh100% (1)
- Astm B688 (1996)Document6 pagesAstm B688 (1996)ElmerNo ratings yet
- M1 Chap-4 Supporting MaterialDocument11 pagesM1 Chap-4 Supporting MaterialRocketNo ratings yet
- GM 1927-16b Exhaust Pipe Bending Process AuditDocument4 pagesGM 1927-16b Exhaust Pipe Bending Process AuditJOHNNo ratings yet
- Electrical Equipment-Circuit DiagramDocument2 pagesElectrical Equipment-Circuit DiagramatitntNo ratings yet
- Light Sources - Basics of Lighting Technologies and Applications, Second EditionDocument296 pagesLight Sources - Basics of Lighting Technologies and Applications, Second EditionSébastien MichaudNo ratings yet
- BSC Data Science Syllabus V6 - 20190528061619 PDFDocument116 pagesBSC Data Science Syllabus V6 - 20190528061619 PDFSahil FarazNo ratings yet
- 3dsmax9 sp1 ReadmeDocument10 pages3dsmax9 sp1 ReadmefresscoNo ratings yet
- RFX 4000071727 Expansion of Ar Rass PV Bsp#9095 - Post Bid ClarificationsDocument40 pagesRFX 4000071727 Expansion of Ar Rass PV Bsp#9095 - Post Bid ClarificationsHaniegrace Lopez SandroNo ratings yet
- Chapter 9 Coal Properties PDFDocument26 pagesChapter 9 Coal Properties PDFAudhinna ZuffyNo ratings yet
- Gold-Rich Porphyry Deposits Descriptive and Genetic Models and Their Role in Exploration and DiscoveryDocument26 pagesGold-Rich Porphyry Deposits Descriptive and Genetic Models and Their Role in Exploration and DiscoveryHellspawn.GeoNo ratings yet
- Parallelizing Particle-In-Cell Codes With Openmp and Mpi: Nils Magnus LarsgårdDocument74 pagesParallelizing Particle-In-Cell Codes With Openmp and Mpi: Nils Magnus LarsgårdqutfizikNo ratings yet
- Module 2Document78 pagesModule 2MANAS DUTTANo ratings yet
- Hokaido Oil-Free Rotary Vane Pump HKD-V Series: Product SpecificationsDocument6 pagesHokaido Oil-Free Rotary Vane Pump HKD-V Series: Product SpecificationsSharath BogaNo ratings yet
- A Proof of The Cayley-Hamilton TheoremDocument4 pagesA Proof of The Cayley-Hamilton TheoremalirNo ratings yet
- Mathematics ReviewDocument5 pagesMathematics ReviewkayNo ratings yet
- ADD103B - Delphi - Folheto PDFDocument2 pagesADD103B - Delphi - Folheto PDFLuiz Claudio Martins FreireNo ratings yet
- Module 4 - Data ManagementDocument38 pagesModule 4 - Data ManagementKobeNo ratings yet
- Automatic Transfer Switch ATS104DMSDocument2 pagesAutomatic Transfer Switch ATS104DMSJabir QuadriNo ratings yet
- 20 Mvar Capacitor BankDocument9 pages20 Mvar Capacitor BankFarah Diba Pos-PosNo ratings yet