Download as pdf or txt
You might also like
- AACR 2022 Proceedings: Part A Online-Only and April 10From EverandAACR 2022 Proceedings: Part A Online-Only and April 10No ratings yet
- NCP For Geriatric by Mikki Kaio LimDocument1 pageNCP For Geriatric by Mikki Kaio LimJeffrey MarianoNo ratings yet
- Detection of Yersinia Pestis in Sputum by Real-Time PCRDocument3 pagesDetection of Yersinia Pestis in Sputum by Real-Time PCRverNo ratings yet
- Identification of Pathogenic Bacteria IranDocument8 pagesIdentification of Pathogenic Bacteria Iranfaraz.mirza1No ratings yet
- Rambabu NarvaneniDocument4 pagesRambabu NarvaneniS291991No ratings yet
- TBC y PCRDocument5 pagesTBC y PCRMayra Castillo CórdovaNo ratings yet
- Rapid Identification of Staphylococcus Aureus: FISH Versus PCR MethodsDocument5 pagesRapid Identification of Staphylococcus Aureus: FISH Versus PCR Methodscoleen paraynoNo ratings yet
- LEPTOSPIRA PCR 1992 Merien FDocument6 pagesLEPTOSPIRA PCR 1992 Merien FMaria Victoria Torres AlvarezNo ratings yet
- PCR PublishedDocument8 pagesPCR PublishedMotikooNo ratings yet
- Quantitative-PCR Assessment of Cryptosporidium Parvum Cell Culture InfectionDocument6 pagesQuantitative-PCR Assessment of Cryptosporidium Parvum Cell Culture InfectionRodolfo Graña ArrospideNo ratings yet
- Especificidad de 100 para Cultivo y PCR en VigilanciaDocument5 pagesEspecificidad de 100 para Cultivo y PCR en VigilanciaCarlos Daniel BraeckmanNo ratings yet
- Prevalence of Enterotoxigenic Clostridium Perfringens in Meats in San Luis, ArgentinaDocument6 pagesPrevalence of Enterotoxigenic Clostridium Perfringens in Meats in San Luis, Argentinamauro manfrediNo ratings yet
- 938 FullDocument5 pages938 FullDiana ElamNo ratings yet
- Anal BiochemDocument7 pagesAnal BiochemRonna Selomenio AlarconNo ratings yet
- Tuberculose TaqmanDocument5 pagesTuberculose TaqmanMarcio Alexandre CustodioNo ratings yet
- Differentiation of Enterotoxigenic and Enteropathogenic Escherichia Coli Isolated From Humans and Calves by rep-PCRDocument6 pagesDifferentiation of Enterotoxigenic and Enteropathogenic Escherichia Coli Isolated From Humans and Calves by rep-PCRArdika AnandaNo ratings yet
- A Simple and Sensitive Method To Extract Bacterial, Yeast and Fungal DNA From Blood Culture MaterialDocument9 pagesA Simple and Sensitive Method To Extract Bacterial, Yeast and Fungal DNA From Blood Culture MaterialAnwar AliNo ratings yet
- Journal of Global Pharma Technology: Research PaperDocument15 pagesJournal of Global Pharma Technology: Research PaperAAANo ratings yet
- Effect of Antibodies On The Expression of Plasmodium Falciparum Circumsporozoite Protein GeneDocument4 pagesEffect of Antibodies On The Expression of Plasmodium Falciparum Circumsporozoite Protein Genereza gomaNo ratings yet
- Peptostreptococcus Micros: Detection of DNA in Clinical Samples by PCRDocument6 pagesPeptostreptococcus Micros: Detection of DNA in Clinical Samples by PCRjorgeNo ratings yet
- 10.33073 - PJM 2022 023Document6 pages10.33073 - PJM 2022 023Andy SetiawanNo ratings yet
- Urinary Tract Infection: Detection of Antigens in Human Urine With An ELIEDA Immunoenzymatic AssayDocument6 pagesUrinary Tract Infection: Detection of Antigens in Human Urine With An ELIEDA Immunoenzymatic AssayEman AyNo ratings yet
- The Veterinary Journal: Jun Zhang, Gui-Hong Zhang, Lin Yang, Ren Huang, Yu Zhang, Kun Jia, Wen Yuan, Shou-Jun LiDocument4 pagesThe Veterinary Journal: Jun Zhang, Gui-Hong Zhang, Lin Yang, Ren Huang, Yu Zhang, Kun Jia, Wen Yuan, Shou-Jun LiEdgar DíazNo ratings yet
- Enterococcus Cecorum Using Three: Fingerprinting of Poultry Isolates of Molecular Typing MethodsDocument6 pagesEnterococcus Cecorum Using Three: Fingerprinting of Poultry Isolates of Molecular Typing MethodsKhoirul Anam 28No ratings yet
- 21 2011-21-IJPP Characterization of Resistant Isolates of M. TuberculosisDocument5 pages21 2011-21-IJPP Characterization of Resistant Isolates of M. TuberculosisDr. Taha NazirNo ratings yet
- Ijmicro2021 2145176Document5 pagesIjmicro2021 2145176cereb24567No ratings yet
- Molecular Detection of Resistance and Virulence Genes in Coagulase Negative Staphylococci Isolated From Blood Cultures at The University Teaching Hospital of BouakeDocument11 pagesMolecular Detection of Resistance and Virulence Genes in Coagulase Negative Staphylococci Isolated From Blood Cultures at The University Teaching Hospital of BouakeSambhavNo ratings yet
- Esc Pointers On The Diagnosis and Administration of Acute Pulmonary EmbolismDocument3 pagesEsc Pointers On The Diagnosis and Administration of Acute Pulmonary EmbolismgwaniegdnrNo ratings yet
- Comparative Diagnostic Methods For Canine EhrlichiosisDocument9 pagesComparative Diagnostic Methods For Canine EhrlichiosisNeny ChalondokterNo ratings yet
- Method: Prevalence and molecular characterization of extended-spectrum β-lactamase-producing Klebsiella pneumoniaeDocument4 pagesMethod: Prevalence and molecular characterization of extended-spectrum β-lactamase-producing Klebsiella pneumoniaeAnupa PokhrelNo ratings yet
- Sarcoid-TB LinkDocument3 pagesSarcoid-TB LinkmytriciallorinNo ratings yet
- 1 s2.0 S016770120500028X MainDocument11 pages1 s2.0 S016770120500028X Mainlouisehip UFCNo ratings yet
- 06 Micro6 12 OrtuDocument6 pages06 Micro6 12 OrtuyusufNo ratings yet
- 1-Eastern Mediterranean Health JournalDocument5 pages1-Eastern Mediterranean Health Journalreadyboy89No ratings yet
- Lembar Jawaban SoalDocument5 pagesLembar Jawaban SoalWahyuNo ratings yet
- Identification of A 200 - To 300-Fold Repetitive 529 BP DNA Fragment in Toxoplasma Gondii - ArtículoDocument7 pagesIdentification of A 200 - To 300-Fold Repetitive 529 BP DNA Fragment in Toxoplasma Gondii - Artículo0244761No ratings yet
- Microwave 1Document3 pagesMicrowave 1Nhe FirmansyahNo ratings yet
- Virulence Factors, Antibiotic Resistance Phenotypes and O-Serogroups of Escherichia Coli Strains Isolated From Community-Acquired Urinary Tract Infection Patients in MexicoDocument8 pagesVirulence Factors, Antibiotic Resistance Phenotypes and O-Serogroups of Escherichia Coli Strains Isolated From Community-Acquired Urinary Tract Infection Patients in MexicounicarpNo ratings yet
- Koo Ken 2014Document7 pagesKoo Ken 2014Perla Andrea Urriola AraosNo ratings yet
- Highly Sensitive and Specific Detection of SRY Gene For Non-Invasive Prenatal DiagnosisDocument6 pagesHighly Sensitive and Specific Detection of SRY Gene For Non-Invasive Prenatal DiagnosisJosue BarralNo ratings yet
- Proteus MirabilisDocument7 pagesProteus MirabilisAnonymous DxCBnr6o0% (1)
- PPT HiponatremiDocument9 pagesPPT HiponatremiArini NurlelaNo ratings yet
- MicrosDocument8 pagesMicrosduchess juliane mirambelNo ratings yet
- 483 jmm030387Document6 pages483 jmm030387rehanaNo ratings yet
- Journal of Clinical Microbiology-2002-Ferroni-3793.fullDocument5 pagesJournal of Clinical Microbiology-2002-Ferroni-3793.fullOgunleke AdebolaNo ratings yet
- Hartmeyer 2017, PCR en Parásitos.Document7 pagesHartmeyer 2017, PCR en Parásitos.planhigion06No ratings yet
- 01 Moore Eval BuccalDocument7 pages01 Moore Eval BuccalRoy WilsonNo ratings yet
- A Novel DNA Microarray For Rapid Diagnosis of Enteropathogenic Bacteria in Stool Specimens of Patients With DiarrheaDocument6 pagesA Novel DNA Microarray For Rapid Diagnosis of Enteropathogenic Bacteria in Stool Specimens of Patients With DiarrheaPritha BhuwapaksophonNo ratings yet
- Jurnal Yersinia1Document9 pagesJurnal Yersinia1Elsa YuniaNo ratings yet
- Direct and Sensitive Detection of Trypanosoma Evansi by Polymerase Chain ReactionDocument9 pagesDirect and Sensitive Detection of Trypanosoma Evansi by Polymerase Chain ReactionFernando RamiroNo ratings yet
- Microbiology of Bartholin's Gland Abscess in JapanDocument4 pagesMicrobiology of Bartholin's Gland Abscess in JapanAlfredo NicholsNo ratings yet
- 511 jmm000460Document6 pages511 jmm000460Nur LaylaNo ratings yet
- Ref 29 These LucDocument7 pagesRef 29 These LucDiariou BahNo ratings yet
- Malaria Paper 2 MANGOLDDocument6 pagesMalaria Paper 2 MANGOLDfajardianhNo ratings yet
- PCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative PathogensDocument7 pagesPCR-based Sepsis@ Quick Test Is Superior in Comparison With Blood Culture For Identification of Sepsis-Causative Pathogensfaraz.mirza1No ratings yet
- 2012 - Development of MPCR For DEC and Shigella SPP and Its EvaluationDocument20 pages2012 - Development of MPCR For DEC and Shigella SPP and Its EvaluationmotibaNo ratings yet
- 2017 Article 286Document9 pages2017 Article 286Idamelis Rodríguez GarcíaNo ratings yet
- Application and Evaluation of Loop Mediated IsotheDocument22 pagesApplication and Evaluation of Loop Mediated IsotheAliyi HassenNo ratings yet
- Diagnosis of Indian Visceral Leishmaniasis by Nucleic Acid Detection Using PCRDocument5 pagesDiagnosis of Indian Visceral Leishmaniasis by Nucleic Acid Detection Using PCRNirvi PorwalNo ratings yet
- 1 - Detection of Hemolysins in AeromonasDocument11 pages1 - Detection of Hemolysins in AeromonasandymicdNo ratings yet
- Development and Application of Nested PCR Assay For Detection of DairyDocument6 pagesDevelopment and Application of Nested PCR Assay For Detection of DairyWiwien HendrawanNo ratings yet
- Executive SummaryDocument3 pagesExecutive SummaryImran RazaNo ratings yet
- Exam First AidDocument2 pagesExam First AidAxmed MaxamedNo ratings yet
- 1st Prelim Exam Wellness MassageDocument2 pages1st Prelim Exam Wellness MassageAnnaVictory Tamse CrisolNo ratings yet
- TENS and EMS Unit (Item # 21010) - Instruction ManualDocument20 pagesTENS and EMS Unit (Item # 21010) - Instruction ManualM Reva Ryanda Reva RyanNo ratings yet
- Circulation 2 QPDocument10 pagesCirculation 2 QPAthenaNo ratings yet
- Acceptance LetterDocument1 pageAcceptance LetterJayzel LaureanoNo ratings yet
- Renal Calculi IntroductionDocument4 pagesRenal Calculi IntroductionirysatherfinestNo ratings yet
- Part of The Team Art Therapy With Pre School Children With Developmental Delays and Disabilities in A Children S Treatment Centre SettingDocument11 pagesPart of The Team Art Therapy With Pre School Children With Developmental Delays and Disabilities in A Children S Treatment Centre SettingBusu AndreeaNo ratings yet
- Essential of Psychiatry For Asthenic and Dermatology PracticeDocument234 pagesEssential of Psychiatry For Asthenic and Dermatology PracticePsychiatry for ResidentsNo ratings yet
- PDF Endoscopic Third Ventriculostomy Classic Concepts and A State of The Art Guide Roberto Alexandre Dezena Ebook Full ChapterDocument53 pagesPDF Endoscopic Third Ventriculostomy Classic Concepts and A State of The Art Guide Roberto Alexandre Dezena Ebook Full Chapteralexander.george507100% (5)
- Prinsip Kedokteran Keluarga 2018Document57 pagesPrinsip Kedokteran Keluarga 2018BisukNo ratings yet
- Apotek Mega Medika: Kode Item Nama Item Jenis Rak Stok Harga Pokok SatuanDocument24 pagesApotek Mega Medika: Kode Item Nama Item Jenis Rak Stok Harga Pokok Satuanyuyun arlitaNo ratings yet
- Moderate SedationDocument39 pagesModerate SedationRiZqi Rufi100% (1)
- Diabetes InsipidusDocument2 pagesDiabetes InsipidusDanielle Ann ChiongNo ratings yet
- Sample CCS-P Exam - (Multiple-Choice Questions)Document5 pagesSample CCS-P Exam - (Multiple-Choice Questions)shyamsunder_nagula100% (1)
- IMCI CARE OF THE CHILD Topic 2Document10 pagesIMCI CARE OF THE CHILD Topic 2Hanna Evidente BakalNo ratings yet
- Levels of PreventionDocument53 pagesLevels of PreventionsunielgowdaNo ratings yet
- Clinical Enzymology 2Document55 pagesClinical Enzymology 2reuben kwotaNo ratings yet
- Social Media and Mental Health - Depression and Psychological EffectsDocument32 pagesSocial Media and Mental Health - Depression and Psychological EffectsShahriar MahmudNo ratings yet
- Week 3 - Topic 1 - Demonstration of Characteristics, Lab Diagnosis & Pathogenesis of StaphylococcusDocument24 pagesWeek 3 - Topic 1 - Demonstration of Characteristics, Lab Diagnosis & Pathogenesis of StaphylococcusTayyaba TahiraNo ratings yet
- Clinical Practice Guideline - Ménière's Disease PDFDocument56 pagesClinical Practice Guideline - Ménière's Disease PDFCarol Natalia Fonseca SalgadoNo ratings yet
- Diabetes CipDocument3 pagesDiabetes CipLlang LleavNo ratings yet
- My Haag 2018Document112 pagesMy Haag 2018Kishenthi KerisnanNo ratings yet
- Screening Tests For Thyroid Dysfunction Is TSH SufficientDocument12 pagesScreening Tests For Thyroid Dysfunction Is TSH SufficientGlobal Research and Development ServicesNo ratings yet
- 1 BiopsyDocument10 pages1 BiopsyDrashi NasirNo ratings yet
- Patient Assessment ToolDocument2 pagesPatient Assessment ToolRachael93% (41)
- Bahasa Inggris 1.13Document5 pagesBahasa Inggris 1.13Rizky AdiNo ratings yet
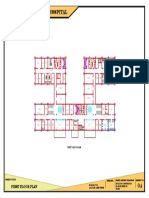
- 100 Bedded General Hospital: First Floor PlanDocument1 page100 Bedded General Hospital: First Floor PlanAshish chauhanNo ratings yet
- Association Food Allergy Dried Fish Complex Regional Pain SyndromeDocument5 pagesAssociation Food Allergy Dried Fish Complex Regional Pain SyndromeSSR-IIJLS JournalNo ratings yet