Download as docx, pdf, or txt
You might also like
- Focus On Nursing Pharmacology 6th Edition Karch Test BankDocument16 pagesFocus On Nursing Pharmacology 6th Edition Karch Test BankElizabethGomezxepgk100% (17)
- Wilson Disease - Treatment and Prognosis - UpToDateDocument13 pagesWilson Disease - Treatment and Prognosis - UpToDatericanoy191No ratings yet
- RPN - Pharmacology (A)Document12 pagesRPN - Pharmacology (A)Ana BienneNo ratings yet
- Hematology, Immunology & OncologyDocument10 pagesHematology, Immunology & Oncologyjennaaahhh67% (3)
- Bios Alex NewDocument32 pagesBios Alex NewAhmed Hassan Ahmed100% (1)
- سموم نظري١Document9 pagesسموم نظري١مصطفى ابراهيم سعيدNo ratings yet
- PharmaDocument9 pagesPharmaemrm1994No ratings yet
- Abram Study NotesDocument6 pagesAbram Study Notesteeman2No ratings yet
- Goodman & Gilman's, The Pharmacological Basis of Therapeutics, 12 Edition, p-1538)Document6 pagesGoodman & Gilman's, The Pharmacological Basis of Therapeutics, 12 Edition, p-1538)Sandeep HavaleNo ratings yet
- Hyperbaric Oxygen Therapy Indications, Contraindictions and ComplicationsDocument5 pagesHyperbaric Oxygen Therapy Indications, Contraindictions and ComplicationsMark DingleNo ratings yet
- Case Study Question 29Document12 pagesCase Study Question 29api-532124328100% (2)
- Chronic Urticaria and Treatment Options: Cme ArticleDocument8 pagesChronic Urticaria and Treatment Options: Cme ArticleYogi SanjayaNo ratings yet
- Intravenous Radiographic Contrast Induced Adverse Reactions - Their Causes, Prevention and Relief MeasuresDocument7 pagesIntravenous Radiographic Contrast Induced Adverse Reactions - Their Causes, Prevention and Relief MeasuresSri HariNo ratings yet
- Symptoms: Cyanide Toxicity Is Often Associated With The Odor of Almonds On BreathDocument2 pagesSymptoms: Cyanide Toxicity Is Often Associated With The Odor of Almonds On BreathRyan PanNo ratings yet
- Calcium Channel BlockersDocument35 pagesCalcium Channel BlockersSufyan MirzaNo ratings yet
- EVMS Critical Care COVID-19 Protocol PDFDocument18 pagesEVMS Critical Care COVID-19 Protocol PDFGreyWolf1776No ratings yet
- Vitamin C, Hydrocortisone and Thiamine in Patients With Septic Shock (VITAMINS) Trial: Study Protocol and Statistical Analysis PlanDocument7 pagesVitamin C, Hydrocortisone and Thiamine in Patients With Septic Shock (VITAMINS) Trial: Study Protocol and Statistical Analysis Planjesus peñaNo ratings yet
- Orig 1 S 040 LBLDocument7 pagesOrig 1 S 040 LBLpatgarettNo ratings yet
- Cardiovascular Practice Questions Answers and RationalesFALL2019-1Document11 pagesCardiovascular Practice Questions Answers and RationalesFALL2019-1titilayo loveNo ratings yet
- Study File ImportantDocument12 pagesStudy File Importantsami khanNo ratings yet
- Efectoas Adversos AtbDocument13 pagesEfectoas Adversos AtbAgueda MaribelNo ratings yet
- Diphenhydramine Hydrochloride (Benadryl) 50mg/1mlDocument6 pagesDiphenhydramine Hydrochloride (Benadryl) 50mg/1ml'SheenMarkReal'No ratings yet
- Anaesthetic AwarenessDocument21 pagesAnaesthetic AwarenessPeter KamNo ratings yet
- Chem Inv ProjDocument15 pagesChem Inv Projsundaram kvNo ratings yet
- COVID-19 Protocol by EVMSDocument13 pagesCOVID-19 Protocol by EVMSKrishnamurthi CG100% (1)
- Medical Surgical Nursing Review Questions Part 3Document8 pagesMedical Surgical Nursing Review Questions Part 3angelfire23phNo ratings yet
- Approach To Mast Cell Activation SyndromeDocument15 pagesApproach To Mast Cell Activation SyndromeKiki sNo ratings yet
- COC Exercise-1Document9 pagesCOC Exercise-1Biyyaol AbiNo ratings yet
- Pharma 2016Document48 pagesPharma 2016backupuoload85No ratings yet
- Case Report-Acquired Melanonychia and Mucocutaneous Hyperpigmentation With Hydroxyurea Therapy-FinalDocument6 pagesCase Report-Acquired Melanonychia and Mucocutaneous Hyperpigmentation With Hydroxyurea Therapy-FinalAtiquzzaman RinkuNo ratings yet
- PDF Abrams Clinical Drug Therapy Rationales For Nursing Practice 11Th Edition Test Bank Online Ebook Full ChapterDocument31 pagesPDF Abrams Clinical Drug Therapy Rationales For Nursing Practice 11Th Edition Test Bank Online Ebook Full Chapterlawrence.sanchez207100% (11)
- Pharmacology For Nurses: The Islamic UniversityDocument118 pagesPharmacology For Nurses: The Islamic UniversityRojina AdhikariNo ratings yet
- Clinical Toxicology-Poisoned Patient Cases W Answers/ExplanationsDocument7 pagesClinical Toxicology-Poisoned Patient Cases W Answers/ExplanationsMarc Imhotep Cray, M.D.100% (3)
- Cancer QuizDocument7 pagesCancer QuizJoshua Flores Fernan100% (1)
- Electrolyte Disturbances Causes and ManagementDocument19 pagesElectrolyte Disturbances Causes and Managementsuci triana putriNo ratings yet
- Pharma QuestionsDocument21 pagesPharma QuestionsCésar HelenoNo ratings yet
- Referat 2Document30 pagesReferat 2kevinNo ratings yet
- 3 TestDocument5 pages3 Testhelianthusannus1997No ratings yet
- Cyanide Poisoning - UpToDateDocument1 pageCyanide Poisoning - UpToDate0087 นันทิชาNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument29 pagesEVMS Critical Care COVID-19 ProtocolJonathan LadinoNo ratings yet
- Consortium ProtocolDocument16 pagesConsortium Protocolthe kingfishNo ratings yet
- Ibandronic Acid Accord Epar Product Information - enDocument56 pagesIbandronic Acid Accord Epar Product Information - enamostafa.betaNo ratings yet
- EVMS Critical Care COVID-19 ProtocolDocument23 pagesEVMS Critical Care COVID-19 ProtocoldarwinNo ratings yet
- Contrast Induced NephropatyDocument4 pagesContrast Induced NephropatySandroLaoNo ratings yet
- Q 4 Consumer ChemistryDocument9 pagesQ 4 Consumer Chemistryeulaliecatherinevegas2No ratings yet
- Amlodipine-10mg TabletDocument7 pagesAmlodipine-10mg TabletMd. Abdur RahmanNo ratings yet
- Clinical Pharmacy QuizDocument3 pagesClinical Pharmacy QuizRoirajiv QuinNo ratings yet
- Clinical Pearls in NephrologyDocument5 pagesClinical Pearls in NephrologyEdmilson R. LimaNo ratings yet
- Cleocin HCL Clindamycin Hydrochloride Capsules, USP: Reference ID: 4092165Document14 pagesCleocin HCL Clindamycin Hydrochloride Capsules, USP: Reference ID: 4092165krizelNo ratings yet
- Peptic Ulcer DiseaseDocument4 pagesPeptic Ulcer DiseaseHikufe JesayaNo ratings yet
- PHARMACY MCQ Quiz 1Document18 pagesPHARMACY MCQ Quiz 1Noah MrjNo ratings yet
- Vit CDocument10 pagesVit C3/2 no.34 สรัญญากร สีหาราชNo ratings yet
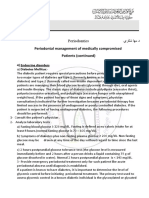
- Periodontal Management of Medically Compromised Patients (Continued)Document11 pagesPeriodontal Management of Medically Compromised Patients (Continued)Yehya Al KhashabNo ratings yet
- Chapter 1: IntroductionDocument27 pagesChapter 1: IntroductionkevinNo ratings yet
- Andreucci 2014Document21 pagesAndreucci 2014NithishNo ratings yet
- Pharmacology 2 14.05.2021Document3 pagesPharmacology 2 14.05.2021VIJAY BHILWADENo ratings yet
- Op ManagmentDocument3 pagesOp ManagmentThevaprathapan ChellathuraiNo ratings yet
- RPN Pharmacology Test (Questions)Document12 pagesRPN Pharmacology Test (Questions)jyselle domingoNo ratings yet
- NP3 RatioDocument17 pagesNP3 RatioArnie Jude CaridoNo ratings yet
- NCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!From EverandNCLEX: Pharmacology for Nurses: 100 Practice Questions with Rationales to help you Pass the NCLEX!Rating: 5 out of 5 stars5/5 (4)
- Complementary and Alternative Medical Lab Testing Part 19: MiscellaneousFrom EverandComplementary and Alternative Medical Lab Testing Part 19: MiscellaneousNo ratings yet
- Oxygen Transport - Regulation of Tissue OxygenationDocument2 pagesOxygen Transport - Regulation of Tissue OxygenationdikshaNo ratings yet
- Metahemoglobinemia - UpToDateDocument66 pagesMetahemoglobinemia - UpToDateYoysi AlvaradoNo ratings yet
- Ulse Ximetry: Steven J. BarkerDocument17 pagesUlse Ximetry: Steven J. BarkerBRYAN RAFAEL ALEMAN HERNANDEZNo ratings yet
- Methemoglobin Reductase PathwayDocument2 pagesMethemoglobin Reductase PathwayinshNo ratings yet
- Pharmacokinetics and Pharmacodynamics of Chlorine Dioxide: July 2021Document25 pagesPharmacokinetics and Pharmacodynamics of Chlorine Dioxide: July 2021Angeles SuarezNo ratings yet
- Forensic and Toxicology NotesDocument31 pagesForensic and Toxicology NotesAspher Ian GummongNo ratings yet
- DyshemoglobinemiasDocument30 pagesDyshemoglobinemiasowlscowlNo ratings yet
- Hematology Must Knows-Converted-1 PDFDocument13 pagesHematology Must Knows-Converted-1 PDFJeffrey LimNo ratings yet
- Drug Induced Hematological Disorders-A Review: June 2019Document8 pagesDrug Induced Hematological Disorders-A Review: June 2019AbiNo ratings yet
- Epidemiological: of Nitrates and Nitrites in TheDocument8 pagesEpidemiological: of Nitrates and Nitrites in TheAndrés MartínezNo ratings yet
- Cyanmethemoglobin Refers To A Relatively NonDocument5 pagesCyanmethemoglobin Refers To A Relatively NonZahir Jayvee Gayak IINo ratings yet
- Abg Final CoachingDocument44 pagesAbg Final CoachingCharmaine LingdasNo ratings yet
- Hypoxia: Peter Dombrovský, Oliver Rácz Peter Dombrovský, Oliver RáczDocument12 pagesHypoxia: Peter Dombrovský, Oliver Rácz Peter Dombrovský, Oliver RáczJulian LondoñoNo ratings yet
- Metode Advia 120Document24 pagesMetode Advia 120IndahNo ratings yet
- Analysis of Polyethylene-Glycol-Polylactide Nano-Dimension Artificial Red Blood Cells in Maintaining Systemic Hemoglobin Levels and Prevention of Methemoglobin FormationDocument19 pagesAnalysis of Polyethylene-Glycol-Polylactide Nano-Dimension Artificial Red Blood Cells in Maintaining Systemic Hemoglobin Levels and Prevention of Methemoglobin FormationIstván PortörőNo ratings yet
- Case Study Blue PeopleDocument4 pagesCase Study Blue Peoplekendall knightNo ratings yet
- Manuale Radiometer OSM3Document5 pagesManuale Radiometer OSM3assistenza tecnicaNo ratings yet
- Ow Q 1-50 (20 - 28.10.09)Document90 pagesOw Q 1-50 (20 - 28.10.09)PradeepNo ratings yet
- MTAP Hema 1 W7 FINALDocument28 pagesMTAP Hema 1 W7 FINALCaleb Joshua MendozaNo ratings yet
- Zlott 2010Document5 pagesZlott 2010dana40018256No ratings yet
- RNS Haematinics Poison AstringentsDocument33 pagesRNS Haematinics Poison AstringentsVaibhav PatilNo ratings yet
- Tatalaksana Keracunan SianidaDocument3 pagesTatalaksana Keracunan SianidanadiaramadaniNo ratings yet
- Hemoglobin and Iron Metabolism: Transport of Respiratory GasesDocument6 pagesHemoglobin and Iron Metabolism: Transport of Respiratory GasesAnusuya SNo ratings yet
- Management of Patients Receiving Local Anaesthesia 2021Document76 pagesManagement of Patients Receiving Local Anaesthesia 2021Micheal ShawkyNo ratings yet
- Human Impact On Ecosystems: ReasonsDocument31 pagesHuman Impact On Ecosystems: ReasonsAsif qaisraniNo ratings yet