
PMC6986221
PMC6986221
You might also like
- Fluids and ElectrolytesDocument6 pagesFluids and ElectrolytesRizMarie100% (1)
- Human Rights Project - Prabjot KaurDocument14 pagesHuman Rights Project - Prabjot Kaurpraboooo100% (1)
- To-The-Points Paper4 Good-Governance-2 Print ManuallyDocument6 pagesTo-The-Points Paper4 Good-Governance-2 Print Manuallyxdpera8No ratings yet
- PPP Task Force Report-DraftDocument41 pagesPPP Task Force Report-DraftSudhir SinghNo ratings yet
- Elements of Good GovernanceDocument4 pagesElements of Good GovernancekennethNo ratings yet
- PPP Task Force Report DraftDocument48 pagesPPP Task Force Report DraftSavita HanamsagarNo ratings yet
- Examining The Influence of Regulatory Governance On Service Quality in Bwera District Hospital, Kasese District, Western Uganda.Document15 pagesExamining The Influence of Regulatory Governance On Service Quality in Bwera District Hospital, Kasese District, Western Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- Transparent - Accountable - Governance-One - World MUST PAPER 2 Topic 15Document15 pagesTransparent - Accountable - Governance-One - World MUST PAPER 2 Topic 15Arvind BoudhaNo ratings yet
- Community Health Workers Promote Civic Engagement and Organizational Capacity To Impact PolicyDocument13 pagesCommunity Health Workers Promote Civic Engagement and Organizational Capacity To Impact Policygujjar gujjarNo ratings yet
- Participation and Public Policies in Brazil: Chapter TwelveDocument11 pagesParticipation and Public Policies in Brazil: Chapter TwelveDeynerose PadonioNo ratings yet
- wg11 HeasysDocument44 pageswg11 Heasysasdf789456123No ratings yet
- Jurnal Nomor 17Document18 pagesJurnal Nomor 17Agusniko SinagaNo ratings yet
- Presentation1 NSTP Dimension of DevelopmentDocument19 pagesPresentation1 NSTP Dimension of Developmentjovelpaulo bautista100% (4)
- Group 1 QDocument18 pagesGroup 1 QCarlos SantosNo ratings yet
- Determining The Implementation Status of Benefits Under Magna Carta of Public Health Workers (RA 7305) in The PhilippinesDocument7 pagesDetermining The Implementation Status of Benefits Under Magna Carta of Public Health Workers (RA 7305) in The Philippineslea mae andoloyNo ratings yet
- Social Audit Is Proposed As A Supplement To Conventional Audit To HelpDocument6 pagesSocial Audit Is Proposed As A Supplement To Conventional Audit To HelpDipu SinghNo ratings yet
- Concept Note On Enhancing Social Accountability in Kenya's Health Sector ConferenceDocument3 pagesConcept Note On Enhancing Social Accountability in Kenya's Health Sector ConferencePower to Youth KenyaNo ratings yet
- Media and Good Governance (Ikejiofor Ifechukwu)Document50 pagesMedia and Good Governance (Ikejiofor Ifechukwu)Pst W C PetersNo ratings yet
- UntitledDocument7 pagesUntitledIvan HiragaNo ratings yet
- M S A E E S A: Ainstreaming Ocial Ccountability Xperiences Manating From Outh SIADocument12 pagesM S A E E S A: Ainstreaming Ocial Ccountability Xperiences Manating From Outh SIANaimur100% (1)
- Thailand Stakeholder Consultation 2008Document11 pagesThailand Stakeholder Consultation 2008Puput WahyuNo ratings yet
- Transform Health National Coordinator EcuadorDocument7 pagesTransform Health National Coordinator EcuadorClaudio GarcíaNo ratings yet
- Why Public Sector ReformDocument4 pagesWhy Public Sector ReformGebretsadik AwgichewNo ratings yet
- Pa 113 SG 3 1Document7 pagesPa 113 SG 3 1Roneil LaplanaNo ratings yet
- BRIEF 3 - What Are The Key Behaviors For Governance of Health Systems V3Document13 pagesBRIEF 3 - What Are The Key Behaviors For Governance of Health Systems V3Souheil DamajNo ratings yet
- Brown Aesthetic Group Project Presentation - 20240415 - 233535 - 0000Document42 pagesBrown Aesthetic Group Project Presentation - 20240415 - 233535 - 0000denise rosalesNo ratings yet
- 91 184 1 SM PDFDocument27 pages91 184 1 SM PDFAccounting SolmanNo ratings yet
- Models For Developing Community Organizations To Reinforce Health Management in Small BusinessesDocument11 pagesModels For Developing Community Organizations To Reinforce Health Management in Small BusinessesSoleil Sierra ReigoNo ratings yet
- Challenges and Prospects of Good Governance in Reduction of Poverty A Case Study of Buee Town 01 Kebele EthiopiaDocument15 pagesChallenges and Prospects of Good Governance in Reduction of Poverty A Case Study of Buee Town 01 Kebele EthiopiaBEALU GIRMAYENo ratings yet
- Good GovernanceDocument5 pagesGood GovernanceAndre Alexi GutierrezNo ratings yet
- 6 WHO 2010 Report Global CampaignDocument4 pages6 WHO 2010 Report Global CampaignAdenantera DwicaksonoNo ratings yet
- Good Governance PresentationDocument14 pagesGood Governance Presentationnoxbrown2No ratings yet
- Daab 064Document9 pagesDaab 064Getachew YematawNo ratings yet
- Rti and MediaDocument11 pagesRti and MediasamsthenimmaneNo ratings yet
- 2003 Orf GN15 enDocument2 pages2003 Orf GN15 enJawms DalaNo ratings yet
- Governance 2Document9 pagesGovernance 2Dena Flandez100% (1)
- Open and Inclusive Principles 2008Document2 pagesOpen and Inclusive Principles 2008EdwardAnderssonNo ratings yet
- Public Private Partnership: By: Ms. Priyanka Bansal Msc. Nursing-I Year Rufaida College of NursingDocument28 pagesPublic Private Partnership: By: Ms. Priyanka Bansal Msc. Nursing-I Year Rufaida College of NursingPriyanka BansalNo ratings yet
- Health Technology Assessment (HTA) - DevelopmentDocument7 pagesHealth Technology Assessment (HTA) - DevelopmentBoyIPNo ratings yet
- JHJHJJHDocument14 pagesJHJHJJHnur arifahNo ratings yet
- Saul-Policy Brief Part IIDocument8 pagesSaul-Policy Brief Part IIlizzieNo ratings yet
- Setting The Agenda For Global Governance - UNDocument7 pagesSetting The Agenda For Global Governance - UNfmwatkinsNo ratings yet
- Sexual Health in The Philippines Community Engagement ProposalDocument13 pagesSexual Health in The Philippines Community Engagement ProposalDensel MacalintalNo ratings yet
- Seminar On GovDocument19 pagesSeminar On GovKiestiko Sri SaptasariNo ratings yet
- Public Prosecutor's Office and Social Control in The National Unified Health System: A Systematic ReviewDocument10 pagesPublic Prosecutor's Office and Social Control in The National Unified Health System: A Systematic ReviewyutefupNo ratings yet
- Chapter 7Document9 pagesChapter 7Lawrence Ryan DaugNo ratings yet
- WP Civil Web RevFinDocument56 pagesWP Civil Web RevFinSumit Kumar YadavNo ratings yet
- Chapter 1Document7 pagesChapter 1Franz N. SyNo ratings yet
- Final Spring 2Document50 pagesFinal Spring 2Shaira Mae YecpotNo ratings yet
- BPAG 172 Solved AssignmentDocument6 pagesBPAG 172 Solved AssignmentDivyansh BajpaiNo ratings yet
- Role of Civil Society in RTI LAWDocument56 pagesRole of Civil Society in RTI LAWlalitdadwal100% (1)
- Applications of Telecommunications and Information Technology For Humanitarian Health InitiativesDocument11 pagesApplications of Telecommunications and Information Technology For Humanitarian Health InitiativesDinesh PudasainiNo ratings yet
- Accountability ParticipatoryDocument2 pagesAccountability ParticipatoryShannon ElizaldeNo ratings yet
- "Good Governance": Distinction From Other Related ConceptDocument7 pages"Good Governance": Distinction From Other Related ConceptRio Albarico100% (1)
- Health Canada Public Health Agency Canada Guidelines Public EngagementDocument29 pagesHealth Canada Public Health Agency Canada Guidelines Public EngagementPaula NahasNo ratings yet
- Name: Veronica KandewoDocument9 pagesName: Veronica KandewoTakudzwa VerengeraNo ratings yet
- Demographic Surveillance: Call For Full ProposalsDocument11 pagesDemographic Surveillance: Call For Full ProposalsAmir MirNo ratings yet
- Tanzania Development PartnerDocument28 pagesTanzania Development PartnerBrenda HendryNo ratings yet
- The Private Sector,: Universal Health Coverage and Primary Health CareDocument12 pagesThe Private Sector,: Universal Health Coverage and Primary Health CareJohn Aries CabilingNo ratings yet
- The politics of health promotion: Case studies from Denmark and EnglandFrom EverandThe politics of health promotion: Case studies from Denmark and EnglandNo ratings yet
- Urban Health and Wellbeing Programme: Policy Briefs: Volume 1From EverandUrban Health and Wellbeing Programme: Policy Briefs: Volume 1Franz W. GatzweilerNo ratings yet
- G.R. Nos. 151983-84Document11 pagesG.R. Nos. 151983-84ghoudzNo ratings yet
- First Division (A.M. No. P-07-2363. July 31, 2008)Document4 pagesFirst Division (A.M. No. P-07-2363. July 31, 2008)ghoudzNo ratings yet
- The Experience of Generalized Anxiety Disorder Through The Lens oDocument42 pagesThe Experience of Generalized Anxiety Disorder Through The Lens oghoudzNo ratings yet
- Fdocuments - in - Labor Relations Azucena Vols1 2Document122 pagesFdocuments - in - Labor Relations Azucena Vols1 2ghoudzNo ratings yet
- W7 Lesson 7 The Structure of English Texts Part 1 ModuleDocument6 pagesW7 Lesson 7 The Structure of English Texts Part 1 ModuleghoudzNo ratings yet
- Investiture Ceremony TroopDocument4 pagesInvestiture Ceremony TroopghoudzNo ratings yet
- Borovsky v. Commissioner, 90 Phil 107Document8 pagesBorovsky v. Commissioner, 90 Phil 107ghoudzNo ratings yet
- First Division (G.R. No. 196015, June 27, 2018)Document9 pagesFirst Division (G.R. No. 196015, June 27, 2018)ghoudzNo ratings yet
- W6 Lesson 6 The Social Context of English Part 2 ModuleDocument11 pagesW6 Lesson 6 The Social Context of English Part 2 ModuleghoudzNo ratings yet
- VelascoDocument76 pagesVelascoghoudzNo ratings yet
- Bayan v. ZamoraDocument51 pagesBayan v. ZamorameowiskuletNo ratings yet
- Pharmaceutical v. Duque, 535 SCRA 265Document49 pagesPharmaceutical v. Duque, 535 SCRA 265ghoudzNo ratings yet
- Saguisag v. Ochoa, GR No. 212426 and 212444Document150 pagesSaguisag v. Ochoa, GR No. 212426 and 212444ghoudzNo ratings yet
- Pimintel V. Exec. Secretary, G.R. No. 158088Document8 pagesPimintel V. Exec. Secretary, G.R. No. 158088ghoudzNo ratings yet
- Method Statement For The Preparation of The Ground For Installation of Right of Way Fence at Marshy AreasDocument3 pagesMethod Statement For The Preparation of The Ground For Installation of Right of Way Fence at Marshy AreasKasun UdaraNo ratings yet
- Chris BoettcherDocument1 pageChris BoettcherKunal MehtaNo ratings yet
- Grasping The Donkey's Tail Unraveling Mysteries From The Classics of Oriental Medicine by Peter Eckman Charles BuckDocument154 pagesGrasping The Donkey's Tail Unraveling Mysteries From The Classics of Oriental Medicine by Peter Eckman Charles BuckLex ReisNo ratings yet
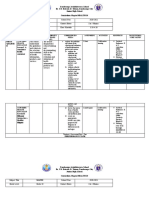
- Zamboanga Avalokitesvara School Dr. J.R. Estrada St. Tetuan, Zamboanga City Junior High School Curriculum Map in HEALTH 10Document8 pagesZamboanga Avalokitesvara School Dr. J.R. Estrada St. Tetuan, Zamboanga City Junior High School Curriculum Map in HEALTH 10Hermie Rose AlvarezNo ratings yet
- Writing A For and Against EssayDocument20 pagesWriting A For and Against EssayCozmina IlieNo ratings yet
- Sof LensDocument1 pageSof Lenspdxuser3390No ratings yet
- Medium Chain TriacylglyceridesDocument6 pagesMedium Chain Triacylglyceridesi love chubz100% (1)
- "Winning" The "Battle" and "Beating" The COVID-19 "Enemy": Leaders' Use of War Frames To Define The PandemicDocument10 pages"Winning" The "Battle" and "Beating" The COVID-19 "Enemy": Leaders' Use of War Frames To Define The PandemicJoaquín GallegoNo ratings yet
- Disaster ManagementDocument54 pagesDisaster Managementritikaritika100% (1)
- Anomalies of The Penies ...Document6 pagesAnomalies of The Penies ...Firas Abu-SamraNo ratings yet
- 2 Comparison Oc Different Drug Regimens For Osteoarthritic Population in Pakistan.Document5 pages2 Comparison Oc Different Drug Regimens For Osteoarthritic Population in Pakistan.muhammad ijazNo ratings yet
- Sugar - The White DeathDocument4 pagesSugar - The White DeathSyncOrSwimNo ratings yet
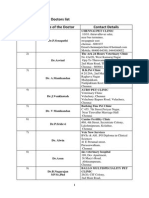
- Chennai Veterinary Doctors ListDocument7 pagesChennai Veterinary Doctors Listsrinivasa777100% (1)
- APLI News: Low Tech, High Touch - Palliative Care in IndiaDocument4 pagesAPLI News: Low Tech, High Touch - Palliative Care in IndiaJanet HsuNo ratings yet
- Open Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132Document3 pagesOpen Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132Ahmed Ben BellaNo ratings yet
- Bowel Prep MayoclinicDocument7 pagesBowel Prep MayoclinicrebeccaNo ratings yet
- Dentsply The Difference Edition 4Document24 pagesDentsply The Difference Edition 4AD TwentyOne DentalNo ratings yet
- Physical Development InfantsDocument36 pagesPhysical Development InfantsChrisel Joy Dela CruzNo ratings yet
- ECR201Document206 pagesECR201Vy KhánhNo ratings yet
- DOCUMENTARYDocument35 pagesDOCUMENTARYSuna SunaNo ratings yet
- ملف الوبائيات بعد التعديلDocument3 pagesملف الوبائيات بعد التعديلMustafa KhudhairNo ratings yet
- Cover LetterDocument2 pagesCover LetterAmos OnhanNo ratings yet
- Division of Leyte: Tabango Senior High School - Stand Alone Brgy. Poblacion, Tabango, LeyteDocument1 pageDivision of Leyte: Tabango Senior High School - Stand Alone Brgy. Poblacion, Tabango, LeyteTinTinNo ratings yet
- Cognitive Impairment Along The Course of Depression: Non-Pharmacological Treatment OptionsDocument11 pagesCognitive Impairment Along The Course of Depression: Non-Pharmacological Treatment OptionsCarolina PradoNo ratings yet
- The 1-Hour Pad Test 2005Document6 pagesThe 1-Hour Pad Test 2005dr. puspitasariNo ratings yet
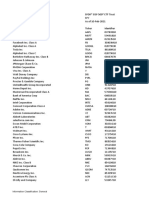
- Holdings Daily Us en SpyDocument32 pagesHoldings Daily Us en SpyAnonymous MF1enDO9No ratings yet
- Planning (Nursing Care Plans)Document10 pagesPlanning (Nursing Care Plans)Kier Jucar de GuzmanNo ratings yet
- ASSESMENT Cardiorespiratory FitnessDocument40 pagesASSESMENT Cardiorespiratory Fitnessmsalungin1313No ratings yet
- W3 Animal Raising Mod9Document28 pagesW3 Animal Raising Mod9alfredo pintoNo ratings yet





































































































Download as pdf or txt
You might also like
- Fluids and ElectrolytesDocument6 pagesFluids and ElectrolytesRizMarie100% (1)
- Human Rights Project - Prabjot KaurDocument14 pagesHuman Rights Project - Prabjot Kaurpraboooo100% (1)
- To-The-Points Paper4 Good-Governance-2 Print ManuallyDocument6 pagesTo-The-Points Paper4 Good-Governance-2 Print Manuallyxdpera8No ratings yet
- PPP Task Force Report-DraftDocument41 pagesPPP Task Force Report-DraftSudhir SinghNo ratings yet
- Elements of Good GovernanceDocument4 pagesElements of Good GovernancekennethNo ratings yet
- PPP Task Force Report DraftDocument48 pagesPPP Task Force Report DraftSavita HanamsagarNo ratings yet
- Examining The Influence of Regulatory Governance On Service Quality in Bwera District Hospital, Kasese District, Western Uganda.Document15 pagesExamining The Influence of Regulatory Governance On Service Quality in Bwera District Hospital, Kasese District, Western Uganda.KIU PUBLICATION AND EXTENSIONNo ratings yet
- Transparent - Accountable - Governance-One - World MUST PAPER 2 Topic 15Document15 pagesTransparent - Accountable - Governance-One - World MUST PAPER 2 Topic 15Arvind BoudhaNo ratings yet
- Community Health Workers Promote Civic Engagement and Organizational Capacity To Impact PolicyDocument13 pagesCommunity Health Workers Promote Civic Engagement and Organizational Capacity To Impact Policygujjar gujjarNo ratings yet
- Participation and Public Policies in Brazil: Chapter TwelveDocument11 pagesParticipation and Public Policies in Brazil: Chapter TwelveDeynerose PadonioNo ratings yet
- wg11 HeasysDocument44 pageswg11 Heasysasdf789456123No ratings yet
- Jurnal Nomor 17Document18 pagesJurnal Nomor 17Agusniko SinagaNo ratings yet
- Presentation1 NSTP Dimension of DevelopmentDocument19 pagesPresentation1 NSTP Dimension of Developmentjovelpaulo bautista100% (4)
- Group 1 QDocument18 pagesGroup 1 QCarlos SantosNo ratings yet
- Determining The Implementation Status of Benefits Under Magna Carta of Public Health Workers (RA 7305) in The PhilippinesDocument7 pagesDetermining The Implementation Status of Benefits Under Magna Carta of Public Health Workers (RA 7305) in The Philippineslea mae andoloyNo ratings yet
- Social Audit Is Proposed As A Supplement To Conventional Audit To HelpDocument6 pagesSocial Audit Is Proposed As A Supplement To Conventional Audit To HelpDipu SinghNo ratings yet
- Concept Note On Enhancing Social Accountability in Kenya's Health Sector ConferenceDocument3 pagesConcept Note On Enhancing Social Accountability in Kenya's Health Sector ConferencePower to Youth KenyaNo ratings yet
- Media and Good Governance (Ikejiofor Ifechukwu)Document50 pagesMedia and Good Governance (Ikejiofor Ifechukwu)Pst W C PetersNo ratings yet
- UntitledDocument7 pagesUntitledIvan HiragaNo ratings yet
- M S A E E S A: Ainstreaming Ocial Ccountability Xperiences Manating From Outh SIADocument12 pagesM S A E E S A: Ainstreaming Ocial Ccountability Xperiences Manating From Outh SIANaimur100% (1)
- Thailand Stakeholder Consultation 2008Document11 pagesThailand Stakeholder Consultation 2008Puput WahyuNo ratings yet
- Transform Health National Coordinator EcuadorDocument7 pagesTransform Health National Coordinator EcuadorClaudio GarcíaNo ratings yet
- Why Public Sector ReformDocument4 pagesWhy Public Sector ReformGebretsadik AwgichewNo ratings yet
- Pa 113 SG 3 1Document7 pagesPa 113 SG 3 1Roneil LaplanaNo ratings yet
- BRIEF 3 - What Are The Key Behaviors For Governance of Health Systems V3Document13 pagesBRIEF 3 - What Are The Key Behaviors For Governance of Health Systems V3Souheil DamajNo ratings yet
- Brown Aesthetic Group Project Presentation - 20240415 - 233535 - 0000Document42 pagesBrown Aesthetic Group Project Presentation - 20240415 - 233535 - 0000denise rosalesNo ratings yet
- 91 184 1 SM PDFDocument27 pages91 184 1 SM PDFAccounting SolmanNo ratings yet
- Models For Developing Community Organizations To Reinforce Health Management in Small BusinessesDocument11 pagesModels For Developing Community Organizations To Reinforce Health Management in Small BusinessesSoleil Sierra ReigoNo ratings yet
- Challenges and Prospects of Good Governance in Reduction of Poverty A Case Study of Buee Town 01 Kebele EthiopiaDocument15 pagesChallenges and Prospects of Good Governance in Reduction of Poverty A Case Study of Buee Town 01 Kebele EthiopiaBEALU GIRMAYENo ratings yet
- Good GovernanceDocument5 pagesGood GovernanceAndre Alexi GutierrezNo ratings yet
- 6 WHO 2010 Report Global CampaignDocument4 pages6 WHO 2010 Report Global CampaignAdenantera DwicaksonoNo ratings yet
- Good Governance PresentationDocument14 pagesGood Governance Presentationnoxbrown2No ratings yet
- Daab 064Document9 pagesDaab 064Getachew YematawNo ratings yet
- Rti and MediaDocument11 pagesRti and MediasamsthenimmaneNo ratings yet
- 2003 Orf GN15 enDocument2 pages2003 Orf GN15 enJawms DalaNo ratings yet
- Governance 2Document9 pagesGovernance 2Dena Flandez100% (1)
- Open and Inclusive Principles 2008Document2 pagesOpen and Inclusive Principles 2008EdwardAnderssonNo ratings yet
- Public Private Partnership: By: Ms. Priyanka Bansal Msc. Nursing-I Year Rufaida College of NursingDocument28 pagesPublic Private Partnership: By: Ms. Priyanka Bansal Msc. Nursing-I Year Rufaida College of NursingPriyanka BansalNo ratings yet
- Health Technology Assessment (HTA) - DevelopmentDocument7 pagesHealth Technology Assessment (HTA) - DevelopmentBoyIPNo ratings yet
- JHJHJJHDocument14 pagesJHJHJJHnur arifahNo ratings yet
- Saul-Policy Brief Part IIDocument8 pagesSaul-Policy Brief Part IIlizzieNo ratings yet
- Setting The Agenda For Global Governance - UNDocument7 pagesSetting The Agenda For Global Governance - UNfmwatkinsNo ratings yet
- Sexual Health in The Philippines Community Engagement ProposalDocument13 pagesSexual Health in The Philippines Community Engagement ProposalDensel MacalintalNo ratings yet
- Seminar On GovDocument19 pagesSeminar On GovKiestiko Sri SaptasariNo ratings yet
- Public Prosecutor's Office and Social Control in The National Unified Health System: A Systematic ReviewDocument10 pagesPublic Prosecutor's Office and Social Control in The National Unified Health System: A Systematic ReviewyutefupNo ratings yet
- Chapter 7Document9 pagesChapter 7Lawrence Ryan DaugNo ratings yet
- WP Civil Web RevFinDocument56 pagesWP Civil Web RevFinSumit Kumar YadavNo ratings yet
- Chapter 1Document7 pagesChapter 1Franz N. SyNo ratings yet
- Final Spring 2Document50 pagesFinal Spring 2Shaira Mae YecpotNo ratings yet
- BPAG 172 Solved AssignmentDocument6 pagesBPAG 172 Solved AssignmentDivyansh BajpaiNo ratings yet
- Role of Civil Society in RTI LAWDocument56 pagesRole of Civil Society in RTI LAWlalitdadwal100% (1)
- Applications of Telecommunications and Information Technology For Humanitarian Health InitiativesDocument11 pagesApplications of Telecommunications and Information Technology For Humanitarian Health InitiativesDinesh PudasainiNo ratings yet
- Accountability ParticipatoryDocument2 pagesAccountability ParticipatoryShannon ElizaldeNo ratings yet
- "Good Governance": Distinction From Other Related ConceptDocument7 pages"Good Governance": Distinction From Other Related ConceptRio Albarico100% (1)
- Health Canada Public Health Agency Canada Guidelines Public EngagementDocument29 pagesHealth Canada Public Health Agency Canada Guidelines Public EngagementPaula NahasNo ratings yet
- Name: Veronica KandewoDocument9 pagesName: Veronica KandewoTakudzwa VerengeraNo ratings yet
- Demographic Surveillance: Call For Full ProposalsDocument11 pagesDemographic Surveillance: Call For Full ProposalsAmir MirNo ratings yet
- Tanzania Development PartnerDocument28 pagesTanzania Development PartnerBrenda HendryNo ratings yet
- The Private Sector,: Universal Health Coverage and Primary Health CareDocument12 pagesThe Private Sector,: Universal Health Coverage and Primary Health CareJohn Aries CabilingNo ratings yet
- The politics of health promotion: Case studies from Denmark and EnglandFrom EverandThe politics of health promotion: Case studies from Denmark and EnglandNo ratings yet
- Urban Health and Wellbeing Programme: Policy Briefs: Volume 1From EverandUrban Health and Wellbeing Programme: Policy Briefs: Volume 1Franz W. GatzweilerNo ratings yet
- G.R. Nos. 151983-84Document11 pagesG.R. Nos. 151983-84ghoudzNo ratings yet
- First Division (A.M. No. P-07-2363. July 31, 2008)Document4 pagesFirst Division (A.M. No. P-07-2363. July 31, 2008)ghoudzNo ratings yet
- The Experience of Generalized Anxiety Disorder Through The Lens oDocument42 pagesThe Experience of Generalized Anxiety Disorder Through The Lens oghoudzNo ratings yet
- Fdocuments - in - Labor Relations Azucena Vols1 2Document122 pagesFdocuments - in - Labor Relations Azucena Vols1 2ghoudzNo ratings yet
- W7 Lesson 7 The Structure of English Texts Part 1 ModuleDocument6 pagesW7 Lesson 7 The Structure of English Texts Part 1 ModuleghoudzNo ratings yet
- Investiture Ceremony TroopDocument4 pagesInvestiture Ceremony TroopghoudzNo ratings yet
- Borovsky v. Commissioner, 90 Phil 107Document8 pagesBorovsky v. Commissioner, 90 Phil 107ghoudzNo ratings yet
- First Division (G.R. No. 196015, June 27, 2018)Document9 pagesFirst Division (G.R. No. 196015, June 27, 2018)ghoudzNo ratings yet
- W6 Lesson 6 The Social Context of English Part 2 ModuleDocument11 pagesW6 Lesson 6 The Social Context of English Part 2 ModuleghoudzNo ratings yet
- VelascoDocument76 pagesVelascoghoudzNo ratings yet
- Bayan v. ZamoraDocument51 pagesBayan v. ZamorameowiskuletNo ratings yet
- Pharmaceutical v. Duque, 535 SCRA 265Document49 pagesPharmaceutical v. Duque, 535 SCRA 265ghoudzNo ratings yet
- Saguisag v. Ochoa, GR No. 212426 and 212444Document150 pagesSaguisag v. Ochoa, GR No. 212426 and 212444ghoudzNo ratings yet
- Pimintel V. Exec. Secretary, G.R. No. 158088Document8 pagesPimintel V. Exec. Secretary, G.R. No. 158088ghoudzNo ratings yet
- Method Statement For The Preparation of The Ground For Installation of Right of Way Fence at Marshy AreasDocument3 pagesMethod Statement For The Preparation of The Ground For Installation of Right of Way Fence at Marshy AreasKasun UdaraNo ratings yet
- Chris BoettcherDocument1 pageChris BoettcherKunal MehtaNo ratings yet
- Grasping The Donkey's Tail Unraveling Mysteries From The Classics of Oriental Medicine by Peter Eckman Charles BuckDocument154 pagesGrasping The Donkey's Tail Unraveling Mysteries From The Classics of Oriental Medicine by Peter Eckman Charles BuckLex ReisNo ratings yet
- Zamboanga Avalokitesvara School Dr. J.R. Estrada St. Tetuan, Zamboanga City Junior High School Curriculum Map in HEALTH 10Document8 pagesZamboanga Avalokitesvara School Dr. J.R. Estrada St. Tetuan, Zamboanga City Junior High School Curriculum Map in HEALTH 10Hermie Rose AlvarezNo ratings yet
- Writing A For and Against EssayDocument20 pagesWriting A For and Against EssayCozmina IlieNo ratings yet
- Sof LensDocument1 pageSof Lenspdxuser3390No ratings yet
- Medium Chain TriacylglyceridesDocument6 pagesMedium Chain Triacylglyceridesi love chubz100% (1)
- "Winning" The "Battle" and "Beating" The COVID-19 "Enemy": Leaders' Use of War Frames To Define The PandemicDocument10 pages"Winning" The "Battle" and "Beating" The COVID-19 "Enemy": Leaders' Use of War Frames To Define The PandemicJoaquín GallegoNo ratings yet
- Disaster ManagementDocument54 pagesDisaster Managementritikaritika100% (1)
- Anomalies of The Penies ...Document6 pagesAnomalies of The Penies ...Firas Abu-SamraNo ratings yet
- 2 Comparison Oc Different Drug Regimens For Osteoarthritic Population in Pakistan.Document5 pages2 Comparison Oc Different Drug Regimens For Osteoarthritic Population in Pakistan.muhammad ijazNo ratings yet
- Sugar - The White DeathDocument4 pagesSugar - The White DeathSyncOrSwimNo ratings yet
- Chennai Veterinary Doctors ListDocument7 pagesChennai Veterinary Doctors Listsrinivasa777100% (1)
- APLI News: Low Tech, High Touch - Palliative Care in IndiaDocument4 pagesAPLI News: Low Tech, High Touch - Palliative Care in IndiaJanet HsuNo ratings yet
- Open Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132Document3 pagesOpen Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132Ahmed Ben BellaNo ratings yet
- Bowel Prep MayoclinicDocument7 pagesBowel Prep MayoclinicrebeccaNo ratings yet
- Dentsply The Difference Edition 4Document24 pagesDentsply The Difference Edition 4AD TwentyOne DentalNo ratings yet
- Physical Development InfantsDocument36 pagesPhysical Development InfantsChrisel Joy Dela CruzNo ratings yet
- ECR201Document206 pagesECR201Vy KhánhNo ratings yet
- DOCUMENTARYDocument35 pagesDOCUMENTARYSuna SunaNo ratings yet
- ملف الوبائيات بعد التعديلDocument3 pagesملف الوبائيات بعد التعديلMustafa KhudhairNo ratings yet
- Cover LetterDocument2 pagesCover LetterAmos OnhanNo ratings yet
- Division of Leyte: Tabango Senior High School - Stand Alone Brgy. Poblacion, Tabango, LeyteDocument1 pageDivision of Leyte: Tabango Senior High School - Stand Alone Brgy. Poblacion, Tabango, LeyteTinTinNo ratings yet
- Cognitive Impairment Along The Course of Depression: Non-Pharmacological Treatment OptionsDocument11 pagesCognitive Impairment Along The Course of Depression: Non-Pharmacological Treatment OptionsCarolina PradoNo ratings yet
- The 1-Hour Pad Test 2005Document6 pagesThe 1-Hour Pad Test 2005dr. puspitasariNo ratings yet
- Holdings Daily Us en SpyDocument32 pagesHoldings Daily Us en SpyAnonymous MF1enDO9No ratings yet
- Planning (Nursing Care Plans)Document10 pagesPlanning (Nursing Care Plans)Kier Jucar de GuzmanNo ratings yet
- ASSESMENT Cardiorespiratory FitnessDocument40 pagesASSESMENT Cardiorespiratory Fitnessmsalungin1313No ratings yet
- W3 Animal Raising Mod9Document28 pagesW3 Animal Raising Mod9alfredo pintoNo ratings yet