
Aung 2017
Aung 2017
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Human Sexuality 4Th Edition Hock Test Bank Full Chapter PDFDocument36 pagesHuman Sexuality 4Th Edition Hock Test Bank Full Chapter PDFMelissaHodgeoxpj100% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Sex Positions Guide and Dirty Talk The Beginners Guide To Discovering New Emotions and Increasing Intimacy Through 29 Exciting Positions. Spice Up (Tantric Sex and Kamasutra Positions) by AshleyDocument342 pagesSex Positions Guide and Dirty Talk The Beginners Guide To Discovering New Emotions and Increasing Intimacy Through 29 Exciting Positions. Spice Up (Tantric Sex and Kamasutra Positions) by Ashleysiddharth mohanty100% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sex Games: 52 Bedroom Challenges To Spice Up Your Love LifeDocument61 pagesSex Games: 52 Bedroom Challenges To Spice Up Your Love LifeCBalcom38% (42)
- Porn and SexDocument10 pagesPorn and SexCleisaxolocolvtwo AndersonNo ratings yet
- The Master PlanDocument8 pagesThe Master PlanCuriousnessify100% (1)
- Sex Christian For MenDocument112 pagesSex Christian For Menjb1510100% (2)
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptSarif CassanovaNo ratings yet
- BouhnikDocument9 pagesBouhnikSarif CassanovaNo ratings yet
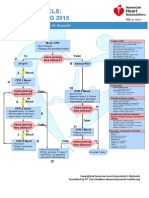
- Algoritma ACLS Bhs IndonesiaDocument6 pagesAlgoritma ACLS Bhs IndonesiaSarif CassanovaNo ratings yet
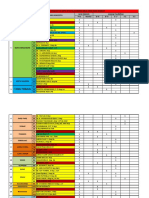
- Rekap Anggota DPD Ipai Sulawesi Selatan Dan Barat: Tana TorajaDocument3 pagesRekap Anggota DPD Ipai Sulawesi Selatan Dan Barat: Tana TorajaSarif CassanovaNo ratings yet
- Management of Foreskin ConditionsDocument26 pagesManagement of Foreskin ConditionsSarif CassanovaNo ratings yet
- HIV and AIDS LECTURE NOTESDocument106 pagesHIV and AIDS LECTURE NOTESMbogo AlexNo ratings yet
- Research RefDocument18 pagesResearch Refbibibebebaby leeleeNo ratings yet
- SexDocument9 pagesSexFlorina AndreiNo ratings yet
- Physical SelfDocument18 pagesPhysical SelfMark Francis SantoNo ratings yet
- "Playboy Isn't Playing," An Interview With Judith Bat-AdaDocument13 pages"Playboy Isn't Playing," An Interview With Judith Bat-AdaJudith Reisman, Ph.D.100% (1)
- Sexual TerminologyDocument2 pagesSexual TerminologyPam BelkevitzNo ratings yet
- Correlates of Sexual Behaviour of Rural College Youth in Maharashtra, IndiaDocument11 pagesCorrelates of Sexual Behaviour of Rural College Youth in Maharashtra, IndiarautyogeshNo ratings yet
- Rupp, Leila - Toward A Global History of Same-Sex Sexuality, (2001) 10 J Hist Sex 287Document16 pagesRupp, Leila - Toward A Global History of Same-Sex Sexuality, (2001) 10 J Hist Sex 287Alana CarrascoNo ratings yet
- Becoming A Master of Oral SexDocument12 pagesBecoming A Master of Oral Sexcharm_temptress0% (1)
- What Teenagers Are Learning From Online PornDocument24 pagesWhat Teenagers Are Learning From Online PornfolioxNo ratings yet
- People Vs CaoiliDocument8 pagesPeople Vs Caoilieunice demaclid100% (1)
- Recommendations For The Collection of Forensic Specimens Jul 22Document7 pagesRecommendations For The Collection of Forensic Specimens Jul 22Mohaaz AbdiNo ratings yet
- Porn AdolescentsDocument25 pagesPorn Adolescentsduyung100% (1)
- College Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeDocument12 pagesCollege Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeGlennKesslerWP100% (1)
- GuideDocument150 pagesGuideavulkNo ratings yet
- GayDocument15 pagesGayjulyerwanni100% (2)
- Kinsey's EducatorsDocument28 pagesKinsey's EducatorsJudith Reisman, Ph.D.No ratings yet
- Neg & ConsentDocument6 pagesNeg & ConsentAnonymous NGLyy3hnNo ratings yet
- The Journal of Sex ResearchDocument12 pagesThe Journal of Sex ResearchMr XNo ratings yet
- FetishDocument6 pagesFetishRedditReads100% (1)
- Internet Pornography A New Form of Vulnerability For The Youth-2019-01!09!09-34Document12 pagesInternet Pornography A New Form of Vulnerability For The Youth-2019-01!09!09-34Impact JournalsNo ratings yet
- Changing Facts SexDocument23 pagesChanging Facts SexAnonymous AhQuZIMNo ratings yet
- The Joys of Anal PDFDocument5 pagesThe Joys of Anal PDFchrisNo ratings yet
- Unit 3Document61 pagesUnit 3JessicaHaeNo ratings yet










































































Download as pdf or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5820)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Human Sexuality 4Th Edition Hock Test Bank Full Chapter PDFDocument36 pagesHuman Sexuality 4Th Edition Hock Test Bank Full Chapter PDFMelissaHodgeoxpj100% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Sex Positions Guide and Dirty Talk The Beginners Guide To Discovering New Emotions and Increasing Intimacy Through 29 Exciting Positions. Spice Up (Tantric Sex and Kamasutra Positions) by AshleyDocument342 pagesSex Positions Guide and Dirty Talk The Beginners Guide To Discovering New Emotions and Increasing Intimacy Through 29 Exciting Positions. Spice Up (Tantric Sex and Kamasutra Positions) by Ashleysiddharth mohanty100% (7)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Sex Games: 52 Bedroom Challenges To Spice Up Your Love LifeDocument61 pagesSex Games: 52 Bedroom Challenges To Spice Up Your Love LifeCBalcom38% (42)
- Porn and SexDocument10 pagesPorn and SexCleisaxolocolvtwo AndersonNo ratings yet
- The Master PlanDocument8 pagesThe Master PlanCuriousnessify100% (1)
- Sex Christian For MenDocument112 pagesSex Christian For Menjb1510100% (2)
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptSarif CassanovaNo ratings yet
- BouhnikDocument9 pagesBouhnikSarif CassanovaNo ratings yet
- Algoritma ACLS Bhs IndonesiaDocument6 pagesAlgoritma ACLS Bhs IndonesiaSarif CassanovaNo ratings yet
- Rekap Anggota DPD Ipai Sulawesi Selatan Dan Barat: Tana TorajaDocument3 pagesRekap Anggota DPD Ipai Sulawesi Selatan Dan Barat: Tana TorajaSarif CassanovaNo ratings yet
- Management of Foreskin ConditionsDocument26 pagesManagement of Foreskin ConditionsSarif CassanovaNo ratings yet
- HIV and AIDS LECTURE NOTESDocument106 pagesHIV and AIDS LECTURE NOTESMbogo AlexNo ratings yet
- Research RefDocument18 pagesResearch Refbibibebebaby leeleeNo ratings yet
- SexDocument9 pagesSexFlorina AndreiNo ratings yet
- Physical SelfDocument18 pagesPhysical SelfMark Francis SantoNo ratings yet
- "Playboy Isn't Playing," An Interview With Judith Bat-AdaDocument13 pages"Playboy Isn't Playing," An Interview With Judith Bat-AdaJudith Reisman, Ph.D.100% (1)
- Sexual TerminologyDocument2 pagesSexual TerminologyPam BelkevitzNo ratings yet
- Correlates of Sexual Behaviour of Rural College Youth in Maharashtra, IndiaDocument11 pagesCorrelates of Sexual Behaviour of Rural College Youth in Maharashtra, IndiarautyogeshNo ratings yet
- Rupp, Leila - Toward A Global History of Same-Sex Sexuality, (2001) 10 J Hist Sex 287Document16 pagesRupp, Leila - Toward A Global History of Same-Sex Sexuality, (2001) 10 J Hist Sex 287Alana CarrascoNo ratings yet
- Becoming A Master of Oral SexDocument12 pagesBecoming A Master of Oral Sexcharm_temptress0% (1)
- What Teenagers Are Learning From Online PornDocument24 pagesWhat Teenagers Are Learning From Online PornfolioxNo ratings yet
- People Vs CaoiliDocument8 pagesPeople Vs Caoilieunice demaclid100% (1)
- Recommendations For The Collection of Forensic Specimens Jul 22Document7 pagesRecommendations For The Collection of Forensic Specimens Jul 22Mohaaz AbdiNo ratings yet
- Porn AdolescentsDocument25 pagesPorn Adolescentsduyung100% (1)
- College Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeDocument12 pagesCollege Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeGlennKesslerWP100% (1)
- GuideDocument150 pagesGuideavulkNo ratings yet
- GayDocument15 pagesGayjulyerwanni100% (2)
- Kinsey's EducatorsDocument28 pagesKinsey's EducatorsJudith Reisman, Ph.D.No ratings yet
- Neg & ConsentDocument6 pagesNeg & ConsentAnonymous NGLyy3hnNo ratings yet
- The Journal of Sex ResearchDocument12 pagesThe Journal of Sex ResearchMr XNo ratings yet
- FetishDocument6 pagesFetishRedditReads100% (1)
- Internet Pornography A New Form of Vulnerability For The Youth-2019-01!09!09-34Document12 pagesInternet Pornography A New Form of Vulnerability For The Youth-2019-01!09!09-34Impact JournalsNo ratings yet
- Changing Facts SexDocument23 pagesChanging Facts SexAnonymous AhQuZIMNo ratings yet
- The Joys of Anal PDFDocument5 pagesThe Joys of Anal PDFchrisNo ratings yet
- Unit 3Document61 pagesUnit 3JessicaHaeNo ratings yet