
A Complete Waste of Money! Water Fluoridation Costs For England, 2013-2021
A Complete Waste of Money! Water Fluoridation Costs For England, 2013-2021
You might also like
- Scale SkillsDocument35 pagesScale Skillspengwang728100% (1)
- CPM - Guidant Corporation Shaping Culture Through Systems - ChristoperDocument19 pagesCPM - Guidant Corporation Shaping Culture Through Systems - ChristoperChrisNaga86% (7)
- Pollution Case StudiesDocument6 pagesPollution Case Studieslekha1997No ratings yet
- EAGLE LSAR Product GuideDocument26 pagesEAGLE LSAR Product Guidejaved iqbal0% (1)
- Tradersworld GannDocument91 pagesTradersworld Gannnicolas arias100% (3)
- Flouride in Dentistry by Ammar MohammedDocument10 pagesFlouride in Dentistry by Ammar Mohammedعمار محمد عباسNo ratings yet
- FluoridesDocument83 pagesFluoridesdr parveen bathlaNo ratings yet
- Nut FluorideDocument12 pagesNut FluorideBrandan SahnkovichNo ratings yet
- UntitledDocument19 pagesUntitledArtemisisNo ratings yet
- Systemic FluorideDocument7 pagesSystemic FluoridemaryamfaidelNo ratings yet
- Manju Arora PDFDocument8 pagesManju Arora PDFSunil ChandraNo ratings yet
- Dr. Ali Fahad Al-Fatlawi Community Dentistry LEC: 6Document3 pagesDr. Ali Fahad Al-Fatlawi Community Dentistry LEC: 6مؤمل رياض سعد كاظمNo ratings yet
- House of Commons Fluoride Thyroid Cancer RiskDocument14 pagesHouse of Commons Fluoride Thyroid Cancer Riskmary engNo ratings yet
- Flouridation of WaterDocument3 pagesFlouridation of WaternareshbalajiNo ratings yet
- Water Fluoridation: A Review of Recent Research and Actions: Joel M. Kauffman, Ph. DDocument7 pagesWater Fluoridation: A Review of Recent Research and Actions: Joel M. Kauffman, Ph. DJack NachamkinNo ratings yet
- Pol LickDocument8 pagesPol LickCesar LeonidasNo ratings yet
- TOXICITY of FLOURIDESDocument45 pagesTOXICITY of FLOURIDESNavneet KaurNo ratings yet
- Defluoridation TechniquesDocument7 pagesDefluoridation TechniquesS Bharadwaj Reddy100% (1)
- Dye-Assisted Analysis of Fluorine in Water Using Uv-Visible Spectrophotometry Chapter One 1.0 1.1 Background To The StudyDocument38 pagesDye-Assisted Analysis of Fluorine in Water Using Uv-Visible Spectrophotometry Chapter One 1.0 1.1 Background To The Studyogundoro kehindeNo ratings yet
- Fluoride Toothpastes and Fluoride Mouthrinses For Home UseDocument11 pagesFluoride Toothpastes and Fluoride Mouthrinses For Home UsePînzariu GeorgeNo ratings yet
- Fluorides in Caries Prevention: Vian Al-JafDocument54 pagesFluorides in Caries Prevention: Vian Al-JafShanaz ShaxawanNo ratings yet
- Systemic FluoridesDocument18 pagesSystemic FluoridesLilly PaulNo ratings yet
- Study of Fluoride ConcentrationDocument5 pagesStudy of Fluoride ConcentrationvoyicoNo ratings yet
- Fluoride in Dentistry: Systemic FluoridationDocument7 pagesFluoride in Dentistry: Systemic FluoridationHaider F YehyaNo ratings yet
- FluoriosisDocument73 pagesFluoriosisnathanielge19No ratings yet
- A Review On Effect of Fluoride Concentration in Drinking Water.Document4 pagesA Review On Effect of Fluoride Concentration in Drinking Water.Anonymous HXZigeNo ratings yet
- You Decide!: Fair WarningDocument4 pagesYou Decide!: Fair WarningMando CondeNo ratings yet
- 07 Chapter 2Document43 pages07 Chapter 2Nitya KrishnaNo ratings yet
- ABCs of FluoridationDocument9 pagesABCs of FluoridationgreenbeeNo ratings yet
- Floride HypothroidismDocument8 pagesFloride HypothroidismwealthandbeyondNo ratings yet
- Fluorides: General DescriptionDocument9 pagesFluorides: General DescriptionRamona MateiNo ratings yet
- Fluoride in DentistryDocument42 pagesFluoride in DentistryAbhishek SoniNo ratings yet
- Flourides and FluoridationDocument38 pagesFlourides and FluoridationmisdduaaNo ratings yet
- Systemic Water Fluoridation IncludeDocument6 pagesSystemic Water Fluoridation IncludeFlorida ManNo ratings yet
- Fluoride and Public Health: The Irish Expert Body On Fluorides and HealthDocument6 pagesFluoride and Public Health: The Irish Expert Body On Fluorides and HealthRizka aulianaNo ratings yet
- Lec 9 PDFDocument7 pagesLec 9 PDFFlorida ManNo ratings yet
- Fluoride Water in New ZealandDocument7 pagesFluoride Water in New ZealandMisbah Sajid ChaudhryNo ratings yet
- FluoridesDocument52 pagesFluoridesRahel CharikarNo ratings yet
- Opp All ChaptersDocument31 pagesOpp All ChaptersAnah Maureen AquinoNo ratings yet
- Systemic FluoridesDocument58 pagesSystemic FluoridesShalakha BhardwajNo ratings yet
- Dental FluorosisDocument70 pagesDental Fluorosiskaran89No ratings yet
- Fluoride Book Chapter PDFDocument28 pagesFluoride Book Chapter PDFBrentt Louis DavidNo ratings yet
- Consumer Health Articles - Fluoride, The Silent KillerDocument4 pagesConsumer Health Articles - Fluoride, The Silent KillershakeymacNo ratings yet
- Defluorination of Drinking WaterDocument6 pagesDefluorination of Drinking WaterEditor IJTSRDNo ratings yet
- FluoridesDocument54 pagesFluoridesNAUMAN SHAHNo ratings yet
- Hidden Dangers in ToothpasteDocument14 pagesHidden Dangers in Toothpastexup88No ratings yet
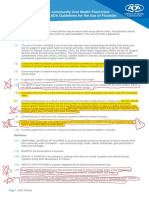
- 1 ADA Fluoride - UseDocument5 pages1 ADA Fluoride - UseTalat SultanaNo ratings yet
- ARTICULO AMERICAN ACADEMY OF PEDIATRIC Fluoride TherapyDocument7 pagesARTICULO AMERICAN ACADEMY OF PEDIATRIC Fluoride TherapykbladimirzmNo ratings yet
- Who Ced PheDocument8 pagesWho Ced PheMuhammad RizwanNo ratings yet
- IAOMT Comprehensive Review On Fluoride in Drugs SupplementsDocument29 pagesIAOMT Comprehensive Review On Fluoride in Drugs SupplementsFelipe LazzarottoNo ratings yet
- Fluoride: To Achieve Credit, You MUST TAKE THIS TEST ONLINE ATDocument5 pagesFluoride: To Achieve Credit, You MUST TAKE THIS TEST ONLINE ATDavidNo ratings yet
- Flouride Map PDFDocument1 pageFlouride Map PDFTesfa AkliluNo ratings yet
- Journal of Dental Research: Topical Fluoride Therapy: Discussion of Some Aspects of Toxicology, Safety, and EfficacyDocument4 pagesJournal of Dental Research: Topical Fluoride Therapy: Discussion of Some Aspects of Toxicology, Safety, and EfficacyBob BobersonNo ratings yet
- Fluoride ReviewDocument5 pagesFluoride ReviewAbelia ABNo ratings yet
- Community Water Fluoridation MythbustersDocument36 pagesCommunity Water Fluoridation MythbustersDavid BriggsNo ratings yet
- BP FluorideTherapyDocument4 pagesBP FluorideTherapyKavana SrinivasNo ratings yet
- Fluoride Therapy: Latest RevisionDocument4 pagesFluoride Therapy: Latest RevisionLaura ZahariaNo ratings yet
- Fluoride in Groundwater: Causes, Implications and Mitigation MeasuresDocument28 pagesFluoride in Groundwater: Causes, Implications and Mitigation MeasuresThao LyNo ratings yet
- Fluoride RemovalDocument16 pagesFluoride RemovalSandeep_AjmireNo ratings yet
- Systemic FluoridesDocument49 pagesSystemic Fluoridesdrdeepikajoash16No ratings yet
- Municipal Water FluoridationDocument4 pagesMunicipal Water Fluoridationdevon0911No ratings yet
- Fluoride TherapyDocument4 pagesFluoride TherapyمعتزباللهNo ratings yet
- Fluoride: Drinking Ourselves to Death?: The Scientific Argument Against Water FluoridationFrom EverandFluoride: Drinking Ourselves to Death?: The Scientific Argument Against Water FluoridationNo ratings yet
- Harrison Chapter 1Document34 pagesHarrison Chapter 1Neha Sohani100% (2)
- Chemical HazardsDocument17 pagesChemical HazardsLloydy HemsworthNo ratings yet
- 9 PowerPoint 2013Document23 pages9 PowerPoint 2013Justz CollectsNo ratings yet
- Synthesis and Characterization of Cadmium Sulphide NanoparticlesDocument17 pagesSynthesis and Characterization of Cadmium Sulphide NanoparticlesHoneylyn IgnacioNo ratings yet
- Trade Marketing and Its EffectsDocument32 pagesTrade Marketing and Its EffectsTrân Trần Ngọc BảoNo ratings yet
- A Seminar On: Sensotronic Brake ControlDocument23 pagesA Seminar On: Sensotronic Brake ControlVed PrakashNo ratings yet
- Catadromoua and Anadromous FishesDocument20 pagesCatadromoua and Anadromous FishesVijay KarotiaNo ratings yet
- SSESP Sample Test PaperDocument4 pagesSSESP Sample Test PaperMuhammad YounisNo ratings yet
- Garia - Wikipedia, The Free EncyclopediaDocument9 pagesGaria - Wikipedia, The Free EncyclopediaPradip DattaNo ratings yet
- NH Màn Hình 2023-05-07 Lúc 09.44.12Document7 pagesNH Màn Hình 2023-05-07 Lúc 09.44.12lechidung072022No ratings yet
- Reading and Writing TOS With ExamDocument2 pagesReading and Writing TOS With Examjoy grace jaraNo ratings yet
- Salaries & Wages - Regular Payroll PERA . Due To BIRDocument7 pagesSalaries & Wages - Regular Payroll PERA . Due To BIRAyie RomeroNo ratings yet
- PeddimunnaDocument1 pagePeddimunnaShaik MunnaNo ratings yet
- Interim Report - SampleDocument34 pagesInterim Report - SampleRISHAV DUTTANo ratings yet
- PCG 30 September 2023 Quarterly Bursa AnnouncementDocument24 pagesPCG 30 September 2023 Quarterly Bursa AnnouncementoodidayooNo ratings yet
- Lab2 - Stereotaxic SurgeryDocument4 pagesLab2 - Stereotaxic SurgeryMichael Anthony BritoNo ratings yet
- Dav Gandhinagar Holiday HomeworkDocument8 pagesDav Gandhinagar Holiday Homeworkafodfexskdfrxb100% (1)
- HLGuide22 23Document38 pagesHLGuide22 23Luis Gerardo Aguilar CruzNo ratings yet
- Hit and Miss Brickwork: BDA Design Note 02Document2 pagesHit and Miss Brickwork: BDA Design Note 02SamNo ratings yet
- RuRecr05112008 PDFDocument14 pagesRuRecr05112008 PDFPrasad DeshpandeNo ratings yet
- 4Training-Material CATIA V5 Assembly Design Ch11 PDFDocument57 pages4Training-Material CATIA V5 Assembly Design Ch11 PDFMohammad Rizal RamlyNo ratings yet
- VX150 VX2 FMB T: 3: Troubleshooting ManualDocument105 pagesVX150 VX2 FMB T: 3: Troubleshooting ManualragiNo ratings yet
- GEZE - Installation Instructions - EN - 1105614Document20 pagesGEZE - Installation Instructions - EN - 1105614eng.rami.ghassanNo ratings yet
- Release NoteDocument10 pagesRelease NoteyusufNo ratings yet
- Mankind and Mother Earth - A Narrative History of The World (PDFDrive)Document680 pagesMankind and Mother Earth - A Narrative History of The World (PDFDrive)Naveen RNo ratings yet
- Uruguay The Owners Manual 5th EdDocument240 pagesUruguay The Owners Manual 5th EdlinkgineerNo ratings yet






















































































Download as pdf or txt
You might also like
- Scale SkillsDocument35 pagesScale Skillspengwang728100% (1)
- CPM - Guidant Corporation Shaping Culture Through Systems - ChristoperDocument19 pagesCPM - Guidant Corporation Shaping Culture Through Systems - ChristoperChrisNaga86% (7)
- Pollution Case StudiesDocument6 pagesPollution Case Studieslekha1997No ratings yet
- EAGLE LSAR Product GuideDocument26 pagesEAGLE LSAR Product Guidejaved iqbal0% (1)
- Tradersworld GannDocument91 pagesTradersworld Gannnicolas arias100% (3)
- Flouride in Dentistry by Ammar MohammedDocument10 pagesFlouride in Dentistry by Ammar Mohammedعمار محمد عباسNo ratings yet
- FluoridesDocument83 pagesFluoridesdr parveen bathlaNo ratings yet
- Nut FluorideDocument12 pagesNut FluorideBrandan SahnkovichNo ratings yet
- UntitledDocument19 pagesUntitledArtemisisNo ratings yet
- Systemic FluorideDocument7 pagesSystemic FluoridemaryamfaidelNo ratings yet
- Manju Arora PDFDocument8 pagesManju Arora PDFSunil ChandraNo ratings yet
- Dr. Ali Fahad Al-Fatlawi Community Dentistry LEC: 6Document3 pagesDr. Ali Fahad Al-Fatlawi Community Dentistry LEC: 6مؤمل رياض سعد كاظمNo ratings yet
- House of Commons Fluoride Thyroid Cancer RiskDocument14 pagesHouse of Commons Fluoride Thyroid Cancer Riskmary engNo ratings yet
- Flouridation of WaterDocument3 pagesFlouridation of WaternareshbalajiNo ratings yet
- Water Fluoridation: A Review of Recent Research and Actions: Joel M. Kauffman, Ph. DDocument7 pagesWater Fluoridation: A Review of Recent Research and Actions: Joel M. Kauffman, Ph. DJack NachamkinNo ratings yet
- Pol LickDocument8 pagesPol LickCesar LeonidasNo ratings yet
- TOXICITY of FLOURIDESDocument45 pagesTOXICITY of FLOURIDESNavneet KaurNo ratings yet
- Defluoridation TechniquesDocument7 pagesDefluoridation TechniquesS Bharadwaj Reddy100% (1)
- Dye-Assisted Analysis of Fluorine in Water Using Uv-Visible Spectrophotometry Chapter One 1.0 1.1 Background To The StudyDocument38 pagesDye-Assisted Analysis of Fluorine in Water Using Uv-Visible Spectrophotometry Chapter One 1.0 1.1 Background To The Studyogundoro kehindeNo ratings yet
- Fluoride Toothpastes and Fluoride Mouthrinses For Home UseDocument11 pagesFluoride Toothpastes and Fluoride Mouthrinses For Home UsePînzariu GeorgeNo ratings yet
- Fluorides in Caries Prevention: Vian Al-JafDocument54 pagesFluorides in Caries Prevention: Vian Al-JafShanaz ShaxawanNo ratings yet
- Systemic FluoridesDocument18 pagesSystemic FluoridesLilly PaulNo ratings yet
- Study of Fluoride ConcentrationDocument5 pagesStudy of Fluoride ConcentrationvoyicoNo ratings yet
- Fluoride in Dentistry: Systemic FluoridationDocument7 pagesFluoride in Dentistry: Systemic FluoridationHaider F YehyaNo ratings yet
- FluoriosisDocument73 pagesFluoriosisnathanielge19No ratings yet
- A Review On Effect of Fluoride Concentration in Drinking Water.Document4 pagesA Review On Effect of Fluoride Concentration in Drinking Water.Anonymous HXZigeNo ratings yet
- You Decide!: Fair WarningDocument4 pagesYou Decide!: Fair WarningMando CondeNo ratings yet
- 07 Chapter 2Document43 pages07 Chapter 2Nitya KrishnaNo ratings yet
- ABCs of FluoridationDocument9 pagesABCs of FluoridationgreenbeeNo ratings yet
- Floride HypothroidismDocument8 pagesFloride HypothroidismwealthandbeyondNo ratings yet
- Fluorides: General DescriptionDocument9 pagesFluorides: General DescriptionRamona MateiNo ratings yet
- Fluoride in DentistryDocument42 pagesFluoride in DentistryAbhishek SoniNo ratings yet
- Flourides and FluoridationDocument38 pagesFlourides and FluoridationmisdduaaNo ratings yet
- Systemic Water Fluoridation IncludeDocument6 pagesSystemic Water Fluoridation IncludeFlorida ManNo ratings yet
- Fluoride and Public Health: The Irish Expert Body On Fluorides and HealthDocument6 pagesFluoride and Public Health: The Irish Expert Body On Fluorides and HealthRizka aulianaNo ratings yet
- Lec 9 PDFDocument7 pagesLec 9 PDFFlorida ManNo ratings yet
- Fluoride Water in New ZealandDocument7 pagesFluoride Water in New ZealandMisbah Sajid ChaudhryNo ratings yet
- FluoridesDocument52 pagesFluoridesRahel CharikarNo ratings yet
- Opp All ChaptersDocument31 pagesOpp All ChaptersAnah Maureen AquinoNo ratings yet
- Systemic FluoridesDocument58 pagesSystemic FluoridesShalakha BhardwajNo ratings yet
- Dental FluorosisDocument70 pagesDental Fluorosiskaran89No ratings yet
- Fluoride Book Chapter PDFDocument28 pagesFluoride Book Chapter PDFBrentt Louis DavidNo ratings yet
- Consumer Health Articles - Fluoride, The Silent KillerDocument4 pagesConsumer Health Articles - Fluoride, The Silent KillershakeymacNo ratings yet
- Defluorination of Drinking WaterDocument6 pagesDefluorination of Drinking WaterEditor IJTSRDNo ratings yet
- FluoridesDocument54 pagesFluoridesNAUMAN SHAHNo ratings yet
- Hidden Dangers in ToothpasteDocument14 pagesHidden Dangers in Toothpastexup88No ratings yet
- 1 ADA Fluoride - UseDocument5 pages1 ADA Fluoride - UseTalat SultanaNo ratings yet
- ARTICULO AMERICAN ACADEMY OF PEDIATRIC Fluoride TherapyDocument7 pagesARTICULO AMERICAN ACADEMY OF PEDIATRIC Fluoride TherapykbladimirzmNo ratings yet
- Who Ced PheDocument8 pagesWho Ced PheMuhammad RizwanNo ratings yet
- IAOMT Comprehensive Review On Fluoride in Drugs SupplementsDocument29 pagesIAOMT Comprehensive Review On Fluoride in Drugs SupplementsFelipe LazzarottoNo ratings yet
- Fluoride: To Achieve Credit, You MUST TAKE THIS TEST ONLINE ATDocument5 pagesFluoride: To Achieve Credit, You MUST TAKE THIS TEST ONLINE ATDavidNo ratings yet
- Flouride Map PDFDocument1 pageFlouride Map PDFTesfa AkliluNo ratings yet
- Journal of Dental Research: Topical Fluoride Therapy: Discussion of Some Aspects of Toxicology, Safety, and EfficacyDocument4 pagesJournal of Dental Research: Topical Fluoride Therapy: Discussion of Some Aspects of Toxicology, Safety, and EfficacyBob BobersonNo ratings yet
- Fluoride ReviewDocument5 pagesFluoride ReviewAbelia ABNo ratings yet
- Community Water Fluoridation MythbustersDocument36 pagesCommunity Water Fluoridation MythbustersDavid BriggsNo ratings yet
- BP FluorideTherapyDocument4 pagesBP FluorideTherapyKavana SrinivasNo ratings yet
- Fluoride Therapy: Latest RevisionDocument4 pagesFluoride Therapy: Latest RevisionLaura ZahariaNo ratings yet
- Fluoride in Groundwater: Causes, Implications and Mitigation MeasuresDocument28 pagesFluoride in Groundwater: Causes, Implications and Mitigation MeasuresThao LyNo ratings yet
- Fluoride RemovalDocument16 pagesFluoride RemovalSandeep_AjmireNo ratings yet
- Systemic FluoridesDocument49 pagesSystemic Fluoridesdrdeepikajoash16No ratings yet
- Municipal Water FluoridationDocument4 pagesMunicipal Water Fluoridationdevon0911No ratings yet
- Fluoride TherapyDocument4 pagesFluoride TherapyمعتزباللهNo ratings yet
- Fluoride: Drinking Ourselves to Death?: The Scientific Argument Against Water FluoridationFrom EverandFluoride: Drinking Ourselves to Death?: The Scientific Argument Against Water FluoridationNo ratings yet
- Harrison Chapter 1Document34 pagesHarrison Chapter 1Neha Sohani100% (2)
- Chemical HazardsDocument17 pagesChemical HazardsLloydy HemsworthNo ratings yet
- 9 PowerPoint 2013Document23 pages9 PowerPoint 2013Justz CollectsNo ratings yet
- Synthesis and Characterization of Cadmium Sulphide NanoparticlesDocument17 pagesSynthesis and Characterization of Cadmium Sulphide NanoparticlesHoneylyn IgnacioNo ratings yet
- Trade Marketing and Its EffectsDocument32 pagesTrade Marketing and Its EffectsTrân Trần Ngọc BảoNo ratings yet
- A Seminar On: Sensotronic Brake ControlDocument23 pagesA Seminar On: Sensotronic Brake ControlVed PrakashNo ratings yet
- Catadromoua and Anadromous FishesDocument20 pagesCatadromoua and Anadromous FishesVijay KarotiaNo ratings yet
- SSESP Sample Test PaperDocument4 pagesSSESP Sample Test PaperMuhammad YounisNo ratings yet
- Garia - Wikipedia, The Free EncyclopediaDocument9 pagesGaria - Wikipedia, The Free EncyclopediaPradip DattaNo ratings yet
- NH Màn Hình 2023-05-07 Lúc 09.44.12Document7 pagesNH Màn Hình 2023-05-07 Lúc 09.44.12lechidung072022No ratings yet
- Reading and Writing TOS With ExamDocument2 pagesReading and Writing TOS With Examjoy grace jaraNo ratings yet
- Salaries & Wages - Regular Payroll PERA . Due To BIRDocument7 pagesSalaries & Wages - Regular Payroll PERA . Due To BIRAyie RomeroNo ratings yet
- PeddimunnaDocument1 pagePeddimunnaShaik MunnaNo ratings yet
- Interim Report - SampleDocument34 pagesInterim Report - SampleRISHAV DUTTANo ratings yet
- PCG 30 September 2023 Quarterly Bursa AnnouncementDocument24 pagesPCG 30 September 2023 Quarterly Bursa AnnouncementoodidayooNo ratings yet
- Lab2 - Stereotaxic SurgeryDocument4 pagesLab2 - Stereotaxic SurgeryMichael Anthony BritoNo ratings yet
- Dav Gandhinagar Holiday HomeworkDocument8 pagesDav Gandhinagar Holiday Homeworkafodfexskdfrxb100% (1)
- HLGuide22 23Document38 pagesHLGuide22 23Luis Gerardo Aguilar CruzNo ratings yet
- Hit and Miss Brickwork: BDA Design Note 02Document2 pagesHit and Miss Brickwork: BDA Design Note 02SamNo ratings yet
- RuRecr05112008 PDFDocument14 pagesRuRecr05112008 PDFPrasad DeshpandeNo ratings yet
- 4Training-Material CATIA V5 Assembly Design Ch11 PDFDocument57 pages4Training-Material CATIA V5 Assembly Design Ch11 PDFMohammad Rizal RamlyNo ratings yet
- VX150 VX2 FMB T: 3: Troubleshooting ManualDocument105 pagesVX150 VX2 FMB T: 3: Troubleshooting ManualragiNo ratings yet
- GEZE - Installation Instructions - EN - 1105614Document20 pagesGEZE - Installation Instructions - EN - 1105614eng.rami.ghassanNo ratings yet
- Release NoteDocument10 pagesRelease NoteyusufNo ratings yet
- Mankind and Mother Earth - A Narrative History of The World (PDFDrive)Document680 pagesMankind and Mother Earth - A Narrative History of The World (PDFDrive)Naveen RNo ratings yet
- Uruguay The Owners Manual 5th EdDocument240 pagesUruguay The Owners Manual 5th EdlinkgineerNo ratings yet