Download as pdf or txt
You might also like
- AutoantibodiesDocument235 pagesAutoantibodiesMihai M100% (2)
- Torch InfectionDocument45 pagesTorch InfectionDragos100% (2)
- ملف 58 معدلDocument58 pagesملف 58 معدلraghdah alhogailNo ratings yet
- Vet Guide PMDDocument8 pagesVet Guide PMDdanxNo ratings yet
- Pcap - PathophysiologyDocument4 pagesPcap - PathophysiologyAyla Mar100% (1)
- Kitten ContractDocument4 pagesKitten Contractapi-318766222No ratings yet
- Muhammad Usman Akram: (DVM Student at Rcvets Lahore)Document29 pagesMuhammad Usman Akram: (DVM Student at Rcvets Lahore)Usman Akram100% (1)
- FCVDocument23 pagesFCVTrailor BladeNo ratings yet
- Canine Ehrlichiosis - Dr. Jibachha Sah, M.V.SC, LecturerDocument34 pagesCanine Ehrlichiosis - Dr. Jibachha Sah, M.V.SC, LecturerJibachha SahNo ratings yet
- VirologyDocument200 pagesVirologyVishal Singh GaharwarNo ratings yet
- Veterinary Forensic ToxicologyDocument11 pagesVeterinary Forensic ToxicologyCarlos Alberto Chaves VelasquezNo ratings yet
- Exhibit List Veterinary Malpractice CaseDocument1 pageExhibit List Veterinary Malpractice CaseOsiris-Khentamentiu100% (1)
- Liver Focus 20Document7 pagesLiver Focus 20Sanja CirkovicNo ratings yet
- FIP: Diagnostic Approach I: Signalment & HistoryDocument4 pagesFIP: Diagnostic Approach I: Signalment & HistoryPetrisor GheorghiuNo ratings yet
- Infectious Diseases of The Dog and Cat, 3rd Edition: CHAPTER 14 Feline Immunodeficiency Virus InfectionDocument24 pagesInfectious Diseases of The Dog and Cat, 3rd Edition: CHAPTER 14 Feline Immunodeficiency Virus InfectionsoledadDC329No ratings yet
- Vaginal Discharge in DogsDocument5 pagesVaginal Discharge in DogsDarmawan Prastyo100% (1)
- Canine PyometraDocument3 pagesCanine PyometraThu Y 2007No ratings yet
- More Accurate Than Ever: Vcheck Product Catalog - 5.1Document36 pagesMore Accurate Than Ever: Vcheck Product Catalog - 5.1dmantsioNo ratings yet
- Techniques For Parasite Assays and Identification in Faecal SamplesDocument15 pagesTechniques For Parasite Assays and Identification in Faecal SamplesSuresh Kumar Ramanathan50% (2)
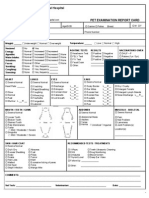
- Vet Examination FormDocument2 pagesVet Examination Formzpallen0003No ratings yet
- (Self-Assessment Color Review) Joyce E. Obradovich - Small Animal Clinical Oncology - Self-Assessment Color review-CRC Press (2017)Document329 pages(Self-Assessment Color Review) Joyce E. Obradovich - Small Animal Clinical Oncology - Self-Assessment Color review-CRC Press (2017)dpcamposhNo ratings yet
- Building Up Competitiveness and The G7's Infrastructure AmbitionsDocument69 pagesBuilding Up Competitiveness and The G7's Infrastructure AmbitionsThe Wilson CenterNo ratings yet
- Chapter 46 - Feline Lower Urinary Tract DiseaseDocument52 pagesChapter 46 - Feline Lower Urinary Tract DiseaseLuis Antonio Buitron Ramirez100% (1)
- Cytologic Patterns - Eclinpath PDFDocument5 pagesCytologic Patterns - Eclinpath PDFJD46No ratings yet
- Veterinary Medicines: A Compact Collection of Information On Veterinary Drugs/medicines in PracticeDocument47 pagesVeterinary Medicines: A Compact Collection of Information On Veterinary Drugs/medicines in PracticeBINAY KUMAR YADAV100% (1)
- King John Necropsy Book 10mar16Document259 pagesKing John Necropsy Book 10mar16Wahid Danang PranathaNo ratings yet
- ACKD in DogsDocument9 pagesACKD in DogsGreomary Cristina MalaverNo ratings yet
- FIP SummaryDocument12 pagesFIP Summarynatalia melladoNo ratings yet
- Veterinary Gynaecology ObstetricsDocument8 pagesVeterinary Gynaecology ObstetricsSuryakantaRoulTuntunNo ratings yet
- NAVLE Competencies FINALDocument19 pagesNAVLE Competencies FINALShubham HarishNo ratings yet
- Manual of Standards For Diagnostic Tests and Vaccines PDFDocument831 pagesManual of Standards For Diagnostic Tests and Vaccines PDFerzebeth bathoryNo ratings yet
- Veterinary ParasitologyDocument12 pagesVeterinary ParasitologyDEV3LLSNo ratings yet
- Extra Information For NavleDocument7 pagesExtra Information For NavleYousef MansourNo ratings yet
- Corona Virus VaccineDocument19 pagesCorona Virus VaccinekanazNo ratings yet
- Disaster-Management 8763694 PowerpointDocument39 pagesDisaster-Management 8763694 PowerpointRoshin VargheseNo ratings yet
- Forensic Pathology of CompanionDocument14 pagesForensic Pathology of CompanionCamila100% (1)
- Veterinary Critical CareDocument15 pagesVeterinary Critical Caresudanfx100% (1)
- Anemia and Pyometra in DogsDocument20 pagesAnemia and Pyometra in DogsVer FajaNo ratings yet
- FelinecalicivirusDocument10 pagesFelinecalicivirusadinda larasNo ratings yet
- Radford 2009Document9 pagesRadford 2009JuniClaudia13No ratings yet
- Feline Herpes VirusDocument10 pagesFeline Herpes Viruskadek ayu ichaNo ratings yet
- Feline Viral Upper Respiratory DiseaseDocument14 pagesFeline Viral Upper Respiratory DiseaseTatiana GrichkovNo ratings yet
- Martell A 2008Document11 pagesMartell A 2008sebastian Jimenez PNo ratings yet
- Feline Infectious Peritonitis ABCD Guidelines On PDocument12 pagesFeline Infectious Peritonitis ABCD Guidelines On Pxn5q8nckvkNo ratings yet
- newbury2021Document18 pagesnewbury2021Karen RodríguezNo ratings yet
- Asvs 05 0724Document4 pagesAsvs 05 0724Vet Muhammad MohsinNo ratings yet
- Varicella Zoster Virus Infection: July 2015Document19 pagesVaricella Zoster Virus Infection: July 2015nickNo ratings yet
- Viro Final 6Document10 pagesViro Final 6Muhammad Arslan UsmanNo ratings yet
- Fowl PoxDocument3 pagesFowl PoxakhmadfuadiNo ratings yet
- Management and Treatment of Herpes Simplex Keratitis: June 2016Document8 pagesManagement and Treatment of Herpes Simplex Keratitis: June 2016debbyNo ratings yet
- Canine ParvovirusDocument13 pagesCanine Parvovirusabhi.tangolliNo ratings yet
- Viro Final 2Document10 pagesViro Final 2Muhammad Arslan UsmanNo ratings yet
- Birnaviridae - Infectious Bursal DiseaseDocument9 pagesBirnaviridae - Infectious Bursal DiseaseELIJAH EUMIR CUNANANNo ratings yet
- 2018 Varicella-Zoster Virus InfectionDocument11 pages2018 Varicella-Zoster Virus Infectioneva yustianaNo ratings yet
- Feline Calicivirus Upper Respiratory Disease DiagnosisDocument2 pagesFeline Calicivirus Upper Respiratory Disease DiagnosisPetrisor GheorghiuNo ratings yet
- Infectious Bronchitis Virus Classical and VariantDocument4 pagesInfectious Bronchitis Virus Classical and VariantŠhâh NawazNo ratings yet
- Canine DistemperDocument18 pagesCanine DistemperJ Elver SilvaNo ratings yet
- Feline Calicivirus: Alan D. R, Karen P. C, Susan D, Carol J. P, Rosalind M. GDocument17 pagesFeline Calicivirus: Alan D. R, Karen P. C, Susan D, Carol J. P, Rosalind M. GCahyadi PutraNo ratings yet
- Overview of Infectious Laryngotracheitis in Poultry: Veterinary ManualDocument2 pagesOverview of Infectious Laryngotracheitis in Poultry: Veterinary ManualSamapanNo ratings yet
- Chapter 65 (Introduction To Viruses)Document16 pagesChapter 65 (Introduction To Viruses)leoNo ratings yet
- Prichard 2021Document12 pagesPrichard 2021Ana Clara PessôaNo ratings yet
- Jurnal UveitisDocument26 pagesJurnal Uveitistitin setya ningsihNo ratings yet
- Topic: "Picoronoviruses. Coxsackie. ECHO. Laboratory Diagnostics"Document26 pagesTopic: "Picoronoviruses. Coxsackie. ECHO. Laboratory Diagnostics"deekshit dcNo ratings yet
- Corona Virus: Q1: Coronavirus Life CycleDocument6 pagesCorona Virus: Q1: Coronavirus Life CycleTufail KhanNo ratings yet
- Circular No. 3 1Document5 pagesCircular No. 3 1spawnn NVX7No ratings yet
- Hubungan Pengetahuan Sikap Penderita Penyakit Malaria FalciparumDocument63 pagesHubungan Pengetahuan Sikap Penderita Penyakit Malaria FalciparumEsty GulsanNo ratings yet
- Chapter 10 - Precipitation and Agglutination - Review QuestionsDocument3 pagesChapter 10 - Precipitation and Agglutination - Review QuestionsTreyton Sekani LopezNo ratings yet
- Polio Eradication: Global Update & ExperienceDocument32 pagesPolio Eradication: Global Update & ExperiencePankaj AgrawalNo ratings yet
- Copar EpiDocument4 pagesCopar EpiCallada NolascoNo ratings yet
- Chapter 14: Principles of Disease and EpidemiologyDocument53 pagesChapter 14: Principles of Disease and EpidemiologyAbhishek Isaac MathewNo ratings yet
- Speech English ItiDocument3 pagesSpeech English ItiBudi AtmikaNo ratings yet
- NIH Public Access: Author ManuscriptDocument33 pagesNIH Public Access: Author ManuscriptIndah Indryani UNo ratings yet
- 1) The Amount of Plasma Proteins ( P.P.) Is Near ToDocument35 pages1) The Amount of Plasma Proteins ( P.P.) Is Near TobmhshNo ratings yet
- Tugas Uas Writing For General Comunication Kelas BDocument9 pagesTugas Uas Writing For General Comunication Kelas Bhadijah offical43119No ratings yet
- Rheum A To Logy QuestionsDocument8 pagesRheum A To Logy QuestionsMark Philip Alfonse0% (1)
- Immuno-Serology & Blood Banking Case Study: Systemic Lupus ErythematosusDocument6 pagesImmuno-Serology & Blood Banking Case Study: Systemic Lupus ErythematosusRomie SolacitoNo ratings yet
- Influenza VirusDocument28 pagesInfluenza VirusDave Despabiladeras100% (2)
- Review Flash Card by Dr. Mitch Roy MaristelaDocument205 pagesReview Flash Card by Dr. Mitch Roy MaristelaMark Justin OcampoNo ratings yet
- Hematology ReviewerDocument10 pagesHematology ReviewerAldren BeliberNo ratings yet
- Malarial Pathogenesis: By: Kareem Waleed Hamimy 6 Year Medical Student Kasr Al Ainy - Cairo UniversityDocument20 pagesMalarial Pathogenesis: By: Kareem Waleed Hamimy 6 Year Medical Student Kasr Al Ainy - Cairo UniversityKareem Waleed Ibrahim HamimyNo ratings yet
- 2chemical MediatorDocument1 page2chemical MediatorUu UuNo ratings yet
- (Methods in Molecular Biology 1139) Michael J.P. Lawman, Patricia D. Lawman (Eds.) - Cancer Vaccines - Methods and Protocols-Humana Press (2014)Document589 pages(Methods in Molecular Biology 1139) Michael J.P. Lawman, Patricia D. Lawman (Eds.) - Cancer Vaccines - Methods and Protocols-Humana Press (2014)mariaNo ratings yet
- Mksap 16Document3 pagesMksap 16Wade BullockNo ratings yet
- TuberculosisDocument16 pagesTuberculosisAhmed Rami100% (1)
- CURS - ENGLEZA - Boli Infectioase PDFDocument246 pagesCURS - ENGLEZA - Boli Infectioase PDFLesan IulianaNo ratings yet
- Eczema Patient LeafletDocument4 pagesEczema Patient LeafletAbdul KareemNo ratings yet
- Nutri TherapyDocument2 pagesNutri TherapySamuel DiazNo ratings yet
- The Diagnosis and Management of Tinea CapitisDocument4 pagesThe Diagnosis and Management of Tinea CapitisKeyla Kehara PutriNo ratings yet
- Inoculations - The True WeaponsDocument1 pageInoculations - The True WeaponsvicaltanNo ratings yet
- Non-Plaque Induced Gingival Diseases: Palle Holmstrup - Jacqueline Plemons - Joerg MeyleDocument16 pagesNon-Plaque Induced Gingival Diseases: Palle Holmstrup - Jacqueline Plemons - Joerg MeyleAnniJassoNo ratings yet