
Head To Toe Write Up
Head To Toe Write Up
You might also like
- Soap Note 4Document8 pagesSoap Note 4api-282129457100% (8)
- Sample SoapDocument9 pagesSample SoapDouglas Greg Cook90% (20)
- Sample SOAP NoteDocument6 pagesSample SOAP NoteLorrie83% (6)
- Final Assessment Soap NoteDocument13 pagesFinal Assessment Soap Noteapi-494643478100% (3)
- Healthcare Issues and Trends Issue PaperDocument10 pagesHealthcare Issues and Trends Issue Paperapi-554096544No ratings yet
- 4 - Msds - Repcon FC MsdsDocument3 pages4 - Msds - Repcon FC MsdsProject m707100% (3)
- Medical Surgical Nursing ExamsDocument37 pagesMedical Surgical Nursing ExamsJheanAlphonsineT.Means100% (9)
- PEDIA Case 4.1. Dengue FeverDocument10 pagesPEDIA Case 4.1. Dengue Feverotartil_nimanNo ratings yet
- 1000 Prometric GP MCQ ExpDocument207 pages1000 Prometric GP MCQ ExpNadia Salwani67% (3)
- (Lorne Ladner, Lama ThubtenDocument158 pages(Lorne Ladner, Lama ThubtenMatheus Pereira CostaNo ratings yet
- USMLE World: Revision QuestionsDocument65 pagesUSMLE World: Revision QuestionsDustin91% (23)
- NCPDocument3 pagesNCPGimcy Dela Fuente100% (6)
- Ward Paper LegitDocument13 pagesWard Paper LegitLuigi FranciscoNo ratings yet
- FNP 3 - JiaDocument16 pagesFNP 3 - Jiaapi-551073862100% (1)
- Low Back PainDocument9 pagesLow Back PainDoc AchondoNo ratings yet
- Form Health History Documentation: Biographical DataDocument7 pagesForm Health History Documentation: Biographical DataSandra SanonNo ratings yet
- FocusedDocument4 pagesFocusedlizdp21No ratings yet
- Validation #3 Graded Documentation SheetsDocument4 pagesValidation #3 Graded Documentation SheetsGelsey Gelsinator JianNo ratings yet
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocument15 pagesCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNo ratings yet
- Geri SOAPsampleDocument8 pagesGeri SOAPsampleJacquelineNo ratings yet
- Comprehensive H and P ExampleDocument5 pagesComprehensive H and P ExampleMallory ZaborNo ratings yet
- History 1Document11 pagesHistory 1KaleabNo ratings yet
- Template Gyn Lo Abd PainDocument18 pagesTemplate Gyn Lo Abd PainHassan HarirNo ratings yet
- SOAP NoteDocument8 pagesSOAP NoteAnonymous p0y5mmLQNo ratings yet
- Family Case AnalysisDocument27 pagesFamily Case AnalysisEzekiel ArtetaNo ratings yet
- Junsay, Twinkle Mae D. Section A - Group 10 History #1Document15 pagesJunsay, Twinkle Mae D. Section A - Group 10 History #1Twinkle Mae JunsayNo ratings yet
- Soap Note CoughDocument19 pagesSoap Note CoughlameckwesiNo ratings yet
- 6904 Module 1 HistoryDocument3 pages6904 Module 1 Historyapi-618492022No ratings yet
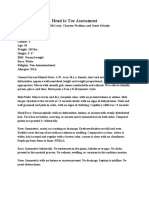
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDocument10 pagesConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoNo ratings yet
- Chief ComplaintDocument7 pagesChief ComplaintyohannesNo ratings yet
- Case Report V Internal MedicineDocument14 pagesCase Report V Internal MedicineGidu SaidNo ratings yet
- CASE STUDY Lung Ca With Pleural EffDocument8 pagesCASE STUDY Lung Ca With Pleural EffL4 CLERK - UY, Rhea Andrea F.No ratings yet
- Ent Case Report Acute Otitis Media Stage IIIDocument12 pagesEnt Case Report Acute Otitis Media Stage IIIRem Alfelor100% (1)
- SOAP Note 1 - Breast CADocument4 pagesSOAP Note 1 - Breast CAacvalvarioNo ratings yet
- Surgery: ENT: Case PresentationDocument67 pagesSurgery: ENT: Case Presentation15Ma. Shaira O PerigoNo ratings yet
- Cwe Nephrotic SnydromeDocument15 pagesCwe Nephrotic SnydromeFariezuan Hamid100% (1)
- Acute PancreatitisDocument7 pagesAcute PancreatitisPatrick DycocoNo ratings yet
- Oniphas Homewoek 2Document14 pagesOniphas Homewoek 2Blake KamminNo ratings yet
- Final Practicum - Soap Note 1Document16 pagesFinal Practicum - Soap Note 1api-49464347867% (3)
- Addis Ababa University Faculty of MedicineDocument12 pagesAddis Ababa University Faculty of MedicinedenekeNo ratings yet
- Tehnik Penyusunan StatusDocument7 pagesTehnik Penyusunan StatusShelly Stephanie BintoroNo ratings yet
- Carbuncle, Incision, Drainage, DebridementDocument11 pagesCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinNo ratings yet
- 3rd Year Precept Pedia Case 4 HydroceleDocument4 pages3rd Year Precept Pedia Case 4 Hydrocelekristel_nicole18yaho100% (1)
- Genome PaperDocument7 pagesGenome Paperapi-444163791100% (1)
- Im - TBDocument11 pagesIm - TBTrisNo ratings yet
- Case Report II Internal MedicineDocument11 pagesCase Report II Internal MedicineGidu SaidNo ratings yet
- BPH Sample To Case ReportDocument12 pagesBPH Sample To Case ReportBirhanu ShiferawNo ratings yet
- Soap Note 5 Acute - Alyssa MatulichDocument7 pagesSoap Note 5 Acute - Alyssa Matulichapi-456313554No ratings yet
- History: O Identifying DataDocument10 pagesHistory: O Identifying DataJofen Ann Hisoler TangpuzNo ratings yet
- Final HX and Physical Dec 2022Document5 pagesFinal HX and Physical Dec 2022Mallory ZaborNo ratings yet
- Fall Out Boy 2Document10 pagesFall Out Boy 2xeileen08No ratings yet
- HISTORY # 1 - PCGH, EchavezDocument11 pagesHISTORY # 1 - PCGH, EchavezHynne Jhea EchavezNo ratings yet
- Case ReportDocument17 pagesCase ReportdenekeNo ratings yet
- IM Gastro FinalDocument10 pagesIM Gastro FinalIzzyMaxinoNo ratings yet
- Bedside Rounds ZCMC Ward 8: History Taking and Physical ExaminationDocument28 pagesBedside Rounds ZCMC Ward 8: History Taking and Physical ExaminationneilaldentanNo ratings yet
- General PE Case Write-Up - Doctoring IIIDocument5 pagesGeneral PE Case Write-Up - Doctoring IIIchristietwongNo ratings yet
- Weebly Head To Toe AssessmentDocument3 pagesWeebly Head To Toe Assessmentapi-608265381No ratings yet
- Soap 2Document5 pagesSoap 2api-456313554No ratings yet
- Pedia - History Taking and Physical Exam - PGI Leira BarbosaDocument6 pagesPedia - History Taking and Physical Exam - PGI Leira BarbosaLeira BarbosaNo ratings yet
- Nursing Care in Tuberculosis PatientsDocument17 pagesNursing Care in Tuberculosis PatientsElisabet SianturiNo ratings yet
- 2 - Carcinoma of TongueDocument14 pages2 - Carcinoma of TonguevaniNo ratings yet
- History and Physical Examination 2014 11 13 00 25 21 UtcDocument7 pagesHistory and Physical Examination 2014 11 13 00 25 21 Utcapi-310557802No ratings yet
- Enterobiasis CaseDocument4 pagesEnterobiasis CaseKimm Delos ReyesNo ratings yet
- Case 2Document12 pagesCase 2atdumagNo ratings yet
- Health AssessmentDocument26 pagesHealth AssessmentBlake Kammin100% (1)
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- NP ResumeDocument3 pagesNP Resumeapi-554096544No ratings yet
- FNP 2 ObesityDocument24 pagesFNP 2 Obesityapi-554096544No ratings yet
- Heart Disease Teaching PlanDocument16 pagesHeart Disease Teaching Planapi-554096544No ratings yet
- NCP-Drug Study 2Document4 pagesNCP-Drug Study 2hsiriaNo ratings yet
- PoultryDocument15 pagesPoultryMekbib MulugetaNo ratings yet
- Guidelines For SCC (R)Document86 pagesGuidelines For SCC (R)lionmusikaNo ratings yet
- Mehlmanmedical Hy Heme/OncDocument46 pagesMehlmanmedical Hy Heme/Oncnav_malhiNo ratings yet
- Colored Concept MapDocument2 pagesColored Concept Mapapi-544878035No ratings yet
- Mefenamic Acid Drug StudyDocument2 pagesMefenamic Acid Drug StudyJude LabajoNo ratings yet
- (ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Document12 pages(ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Karen EstavilloNo ratings yet
- Readers Digest (Can) 1404Document146 pagesReaders Digest (Can) 1404ChristianBailes89% (9)
- Memory Dysfunction.9Document14 pagesMemory Dysfunction.9Luis Antonio Cespedes HernandezNo ratings yet
- DRUG-STUDY OmeprazoleIV AngelicaRonquilloDocument4 pagesDRUG-STUDY OmeprazoleIV AngelicaRonquillokarl eiron delos santosNo ratings yet
- Elderly Care 101-NGT and PEGDocument92 pagesElderly Care 101-NGT and PEGBecky GalanoNo ratings yet
- Acute Suppurative Otitis MediaDocument87 pagesAcute Suppurative Otitis MediaHermawan Surya Dharma100% (1)
- THT Jurnal ReadingDocument22 pagesTHT Jurnal ReadingNidyasari Ucrit Citraningrum SatyariniNo ratings yet
- Zotrim Efficacy of Zotrim A Herbal Weight Loss PreparationDocument4 pagesZotrim Efficacy of Zotrim A Herbal Weight Loss PreparationbscmsNo ratings yet
- Durio. in Southeast Asia, People Used To Call "King of Fruits" or "Raja Buah" As It NicknameDocument13 pagesDurio. in Southeast Asia, People Used To Call "King of Fruits" or "Raja Buah" As It NicknamefakhrulNo ratings yet
- NP2Document20 pagesNP2Anonymous hDcvpptNo ratings yet
- Vaccination WorkshopDocument76 pagesVaccination WorkshopLaney Sweet100% (2)
- Materi Nursing Care PlanDocument1 pageMateri Nursing Care PlanSiti nur Kholifatus samsiyahNo ratings yet
- Noor2016 PDFDocument13 pagesNoor2016 PDFBilel DhaouadiNo ratings yet
- Soal Pas Genap Bahasa Inggris Kelas XiDocument2 pagesSoal Pas Genap Bahasa Inggris Kelas XilikhinNo ratings yet
- NEET PG MOCK TEST MergedDocument103 pagesNEET PG MOCK TEST MergedShaik AmjadNo ratings yet
- GROUP 2-Health-Care-Development-SystemDocument76 pagesGROUP 2-Health-Care-Development-SystemEzra MaeNo ratings yet
- Ibong Adarna Summary in EnglishDocument2 pagesIbong Adarna Summary in EnglishTaihei SanNo ratings yet
- Case Study (Medical Ward)Document5 pagesCase Study (Medical Ward)George Mikhail Labuguen100% (1)




























































































Download as docx, pdf, or txt
You might also like
- Soap Note 4Document8 pagesSoap Note 4api-282129457100% (8)
- Sample SoapDocument9 pagesSample SoapDouglas Greg Cook90% (20)
- Sample SOAP NoteDocument6 pagesSample SOAP NoteLorrie83% (6)
- Final Assessment Soap NoteDocument13 pagesFinal Assessment Soap Noteapi-494643478100% (3)
- Healthcare Issues and Trends Issue PaperDocument10 pagesHealthcare Issues and Trends Issue Paperapi-554096544No ratings yet
- 4 - Msds - Repcon FC MsdsDocument3 pages4 - Msds - Repcon FC MsdsProject m707100% (3)
- Medical Surgical Nursing ExamsDocument37 pagesMedical Surgical Nursing ExamsJheanAlphonsineT.Means100% (9)
- PEDIA Case 4.1. Dengue FeverDocument10 pagesPEDIA Case 4.1. Dengue Feverotartil_nimanNo ratings yet
- 1000 Prometric GP MCQ ExpDocument207 pages1000 Prometric GP MCQ ExpNadia Salwani67% (3)
- (Lorne Ladner, Lama ThubtenDocument158 pages(Lorne Ladner, Lama ThubtenMatheus Pereira CostaNo ratings yet
- USMLE World: Revision QuestionsDocument65 pagesUSMLE World: Revision QuestionsDustin91% (23)
- NCPDocument3 pagesNCPGimcy Dela Fuente100% (6)
- Ward Paper LegitDocument13 pagesWard Paper LegitLuigi FranciscoNo ratings yet
- FNP 3 - JiaDocument16 pagesFNP 3 - Jiaapi-551073862100% (1)
- Low Back PainDocument9 pagesLow Back PainDoc AchondoNo ratings yet
- Form Health History Documentation: Biographical DataDocument7 pagesForm Health History Documentation: Biographical DataSandra SanonNo ratings yet
- FocusedDocument4 pagesFocusedlizdp21No ratings yet
- Validation #3 Graded Documentation SheetsDocument4 pagesValidation #3 Graded Documentation SheetsGelsey Gelsinator JianNo ratings yet
- CASE 3 MEDICINE JULY 10 2019 AcutePyeloDocument15 pagesCASE 3 MEDICINE JULY 10 2019 AcutePyeloTrisNo ratings yet
- Geri SOAPsampleDocument8 pagesGeri SOAPsampleJacquelineNo ratings yet
- Comprehensive H and P ExampleDocument5 pagesComprehensive H and P ExampleMallory ZaborNo ratings yet
- History 1Document11 pagesHistory 1KaleabNo ratings yet
- Template Gyn Lo Abd PainDocument18 pagesTemplate Gyn Lo Abd PainHassan HarirNo ratings yet
- SOAP NoteDocument8 pagesSOAP NoteAnonymous p0y5mmLQNo ratings yet
- Family Case AnalysisDocument27 pagesFamily Case AnalysisEzekiel ArtetaNo ratings yet
- Junsay, Twinkle Mae D. Section A - Group 10 History #1Document15 pagesJunsay, Twinkle Mae D. Section A - Group 10 History #1Twinkle Mae JunsayNo ratings yet
- Soap Note CoughDocument19 pagesSoap Note CoughlameckwesiNo ratings yet
- 6904 Module 1 HistoryDocument3 pages6904 Module 1 Historyapi-618492022No ratings yet
- Constitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofDocument10 pagesConstitutional: General Appearance: Healthy-Appearing, Well-Nourished, and Well-Developed. Level ofRichard ObinwankwoNo ratings yet
- Chief ComplaintDocument7 pagesChief ComplaintyohannesNo ratings yet
- Case Report V Internal MedicineDocument14 pagesCase Report V Internal MedicineGidu SaidNo ratings yet
- CASE STUDY Lung Ca With Pleural EffDocument8 pagesCASE STUDY Lung Ca With Pleural EffL4 CLERK - UY, Rhea Andrea F.No ratings yet
- Ent Case Report Acute Otitis Media Stage IIIDocument12 pagesEnt Case Report Acute Otitis Media Stage IIIRem Alfelor100% (1)
- SOAP Note 1 - Breast CADocument4 pagesSOAP Note 1 - Breast CAacvalvarioNo ratings yet
- Surgery: ENT: Case PresentationDocument67 pagesSurgery: ENT: Case Presentation15Ma. Shaira O PerigoNo ratings yet
- Cwe Nephrotic SnydromeDocument15 pagesCwe Nephrotic SnydromeFariezuan Hamid100% (1)
- Acute PancreatitisDocument7 pagesAcute PancreatitisPatrick DycocoNo ratings yet
- Oniphas Homewoek 2Document14 pagesOniphas Homewoek 2Blake KamminNo ratings yet
- Final Practicum - Soap Note 1Document16 pagesFinal Practicum - Soap Note 1api-49464347867% (3)
- Addis Ababa University Faculty of MedicineDocument12 pagesAddis Ababa University Faculty of MedicinedenekeNo ratings yet
- Tehnik Penyusunan StatusDocument7 pagesTehnik Penyusunan StatusShelly Stephanie BintoroNo ratings yet
- Carbuncle, Incision, Drainage, DebridementDocument11 pagesCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinNo ratings yet
- 3rd Year Precept Pedia Case 4 HydroceleDocument4 pages3rd Year Precept Pedia Case 4 Hydrocelekristel_nicole18yaho100% (1)
- Genome PaperDocument7 pagesGenome Paperapi-444163791100% (1)
- Im - TBDocument11 pagesIm - TBTrisNo ratings yet
- Case Report II Internal MedicineDocument11 pagesCase Report II Internal MedicineGidu SaidNo ratings yet
- BPH Sample To Case ReportDocument12 pagesBPH Sample To Case ReportBirhanu ShiferawNo ratings yet
- Soap Note 5 Acute - Alyssa MatulichDocument7 pagesSoap Note 5 Acute - Alyssa Matulichapi-456313554No ratings yet
- History: O Identifying DataDocument10 pagesHistory: O Identifying DataJofen Ann Hisoler TangpuzNo ratings yet
- Final HX and Physical Dec 2022Document5 pagesFinal HX and Physical Dec 2022Mallory ZaborNo ratings yet
- Fall Out Boy 2Document10 pagesFall Out Boy 2xeileen08No ratings yet
- HISTORY # 1 - PCGH, EchavezDocument11 pagesHISTORY # 1 - PCGH, EchavezHynne Jhea EchavezNo ratings yet
- Case ReportDocument17 pagesCase ReportdenekeNo ratings yet
- IM Gastro FinalDocument10 pagesIM Gastro FinalIzzyMaxinoNo ratings yet
- Bedside Rounds ZCMC Ward 8: History Taking and Physical ExaminationDocument28 pagesBedside Rounds ZCMC Ward 8: History Taking and Physical ExaminationneilaldentanNo ratings yet
- General PE Case Write-Up - Doctoring IIIDocument5 pagesGeneral PE Case Write-Up - Doctoring IIIchristietwongNo ratings yet
- Weebly Head To Toe AssessmentDocument3 pagesWeebly Head To Toe Assessmentapi-608265381No ratings yet
- Soap 2Document5 pagesSoap 2api-456313554No ratings yet
- Pedia - History Taking and Physical Exam - PGI Leira BarbosaDocument6 pagesPedia - History Taking and Physical Exam - PGI Leira BarbosaLeira BarbosaNo ratings yet
- Nursing Care in Tuberculosis PatientsDocument17 pagesNursing Care in Tuberculosis PatientsElisabet SianturiNo ratings yet
- 2 - Carcinoma of TongueDocument14 pages2 - Carcinoma of TonguevaniNo ratings yet
- History and Physical Examination 2014 11 13 00 25 21 UtcDocument7 pagesHistory and Physical Examination 2014 11 13 00 25 21 Utcapi-310557802No ratings yet
- Enterobiasis CaseDocument4 pagesEnterobiasis CaseKimm Delos ReyesNo ratings yet
- Case 2Document12 pagesCase 2atdumagNo ratings yet
- Health AssessmentDocument26 pagesHealth AssessmentBlake Kammin100% (1)
- Chronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicFrom EverandChronic Diseases - Lymes, Hpv, Hsv Mis-Diagnosis and Mistreatment: A New Approach to the EpidemicRating: 5 out of 5 stars5/5 (1)
- NP ResumeDocument3 pagesNP Resumeapi-554096544No ratings yet
- FNP 2 ObesityDocument24 pagesFNP 2 Obesityapi-554096544No ratings yet
- Heart Disease Teaching PlanDocument16 pagesHeart Disease Teaching Planapi-554096544No ratings yet
- NCP-Drug Study 2Document4 pagesNCP-Drug Study 2hsiriaNo ratings yet
- PoultryDocument15 pagesPoultryMekbib MulugetaNo ratings yet
- Guidelines For SCC (R)Document86 pagesGuidelines For SCC (R)lionmusikaNo ratings yet
- Mehlmanmedical Hy Heme/OncDocument46 pagesMehlmanmedical Hy Heme/Oncnav_malhiNo ratings yet
- Colored Concept MapDocument2 pagesColored Concept Mapapi-544878035No ratings yet
- Mefenamic Acid Drug StudyDocument2 pagesMefenamic Acid Drug StudyJude LabajoNo ratings yet
- (ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Document12 pages(ObstetricsA) Prenatal Care - Dr. San Jose (Lea Pacis)Karen EstavilloNo ratings yet
- Readers Digest (Can) 1404Document146 pagesReaders Digest (Can) 1404ChristianBailes89% (9)
- Memory Dysfunction.9Document14 pagesMemory Dysfunction.9Luis Antonio Cespedes HernandezNo ratings yet
- DRUG-STUDY OmeprazoleIV AngelicaRonquilloDocument4 pagesDRUG-STUDY OmeprazoleIV AngelicaRonquillokarl eiron delos santosNo ratings yet
- Elderly Care 101-NGT and PEGDocument92 pagesElderly Care 101-NGT and PEGBecky GalanoNo ratings yet
- Acute Suppurative Otitis MediaDocument87 pagesAcute Suppurative Otitis MediaHermawan Surya Dharma100% (1)
- THT Jurnal ReadingDocument22 pagesTHT Jurnal ReadingNidyasari Ucrit Citraningrum SatyariniNo ratings yet
- Zotrim Efficacy of Zotrim A Herbal Weight Loss PreparationDocument4 pagesZotrim Efficacy of Zotrim A Herbal Weight Loss PreparationbscmsNo ratings yet
- Durio. in Southeast Asia, People Used To Call "King of Fruits" or "Raja Buah" As It NicknameDocument13 pagesDurio. in Southeast Asia, People Used To Call "King of Fruits" or "Raja Buah" As It NicknamefakhrulNo ratings yet
- NP2Document20 pagesNP2Anonymous hDcvpptNo ratings yet
- Vaccination WorkshopDocument76 pagesVaccination WorkshopLaney Sweet100% (2)
- Materi Nursing Care PlanDocument1 pageMateri Nursing Care PlanSiti nur Kholifatus samsiyahNo ratings yet
- Noor2016 PDFDocument13 pagesNoor2016 PDFBilel DhaouadiNo ratings yet
- Soal Pas Genap Bahasa Inggris Kelas XiDocument2 pagesSoal Pas Genap Bahasa Inggris Kelas XilikhinNo ratings yet
- NEET PG MOCK TEST MergedDocument103 pagesNEET PG MOCK TEST MergedShaik AmjadNo ratings yet
- GROUP 2-Health-Care-Development-SystemDocument76 pagesGROUP 2-Health-Care-Development-SystemEzra MaeNo ratings yet
- Ibong Adarna Summary in EnglishDocument2 pagesIbong Adarna Summary in EnglishTaihei SanNo ratings yet
- Case Study (Medical Ward)Document5 pagesCase Study (Medical Ward)George Mikhail Labuguen100% (1)