Download as pdf or txt
You might also like
- 3 - Interpretation of Coronary AngiogramDocument110 pages3 - Interpretation of Coronary Angiogrammv.sudeepNo ratings yet
- Basic Coronary Angiography - All Slides PDFDocument55 pagesBasic Coronary Angiography - All Slides PDFCarlos Arroyo0% (1)
- ECG .DR Ayalew EthiopiaDocument60 pagesECG .DR Ayalew EthiopiaAyalew Zewdie100% (2)
- Siemens J Press Sidebar Filter Press PDFDocument12 pagesSiemens J Press Sidebar Filter Press PDFTrần Khánh Duy100% (1)
- Aurigemma Chamber Quantitation 2021 SlidesDocument55 pagesAurigemma Chamber Quantitation 2021 SlidesSajjad HussainNo ratings yet
- Freeman Aortic RegurgitationDocument102 pagesFreeman Aortic RegurgitationJose Ignacio Tarton SisimitNo ratings yet
- 4conference mv2 HKR PDFDocument87 pages4conference mv2 HKR PDFekafithraNo ratings yet
- Asessement of RV Function: by Rakshitha NayakDocument41 pagesAsessement of RV Function: by Rakshitha NayakSAI HARSHITHA PulluruNo ratings yet
- Aurigemma Systolic Function, Remodeling 2021 SlidesDocument74 pagesAurigemma Systolic Function, Remodeling 2021 SlidesSajjad HussainNo ratings yet
- Aurigemma Haemodynamics 2021 SlidesDocument67 pagesAurigemma Haemodynamics 2021 SlidesSajjad HussainNo ratings yet
- Carpentier Mitral Valve Regurgitation ClasifDocument45 pagesCarpentier Mitral Valve Regurgitation ClasifKudor Szabadi Zoltán100% (1)
- Basic Coronary Angiography All SlidesDocument55 pagesBasic Coronary Angiography All SlidesSaud ShirwanNo ratings yet
- Basic Coronary Angiography All SlidesDocument55 pagesBasic Coronary Angiography All SlidesSaud ShirwanNo ratings yet
- Basic Coronary Angiography All SlidesDocument55 pagesBasic Coronary Angiography All SlidesSaud ShirwanNo ratings yet
- Cme Ecg InterpretationDocument60 pagesCme Ecg InterpretationAtirah AaNo ratings yet
- Didactics ECGDocument87 pagesDidactics ECGGenesis Poblacion100% (1)
- DCM EchocardiographyDocument100 pagesDCM EchocardiographyJoshwin DemetriusNo ratings yet
- Echo With KosmosDocument57 pagesEcho With Kosmossamirmohamed900No ratings yet
- Journal LADocument38 pagesJournal LANovi RobiyantiNo ratings yet
- PcicardDocument2 pagesPcicardWahdat100% (2)
- 07.01 - 12 Lead ECG Interpretation 2019Document141 pages07.01 - 12 Lead ECG Interpretation 2019Lana LocoNo ratings yet
- TTE Pada Stenosis AortaDocument25 pagesTTE Pada Stenosis AortaFaridaFaradillaPutryCherewetNo ratings yet
- Sat 1315-1415 Cardiac AngiogDocument47 pagesSat 1315-1415 Cardiac AngiogbenypermadiNo ratings yet
- TTE Pada Regurgitasi AortaDocument32 pagesTTE Pada Regurgitasi AortaFaridaFaradillaPutryCherewetNo ratings yet
- Basic EchocardiographyDocument54 pagesBasic Echocardiographyramon100% (23)
- Anatomi Jantung & Konsep Dasar Elektrokardiografi: Dr. Zainal Safri, SPPD, SPJPDocument67 pagesAnatomi Jantung & Konsep Dasar Elektrokardiografi: Dr. Zainal Safri, SPPD, SPJPIndah MaulidawatiNo ratings yet
- ElectrocardiographyDocument101 pagesElectrocardiographyPriya jNo ratings yet
- Echocardiography Evaluation For The Tricuspid ValveDocument48 pagesEchocardiography Evaluation For The Tricuspid ValveSofia KusumadewiNo ratings yet
- Result Analysis Date: November 22, 2017 Conclusion: V. Laboratories and Diagnostic ExamsDocument7 pagesResult Analysis Date: November 22, 2017 Conclusion: V. Laboratories and Diagnostic ExamsEllaine Joy Mesina PadizNo ratings yet
- Angiographic Views and Nomencluture PDFDocument36 pagesAngiographic Views and Nomencluture PDFZahidNo ratings yet
- 10 Pulm HTN Florida - 2017Document81 pages10 Pulm HTN Florida - 2017MNo ratings yet
- Steps EchoDocument2 pagesSteps EchoBagus Andi PramonoNo ratings yet
- Pelatihan Ekg Dokter Puskesmas 30 Okt 2009Document75 pagesPelatihan Ekg Dokter Puskesmas 30 Okt 2009fathaNo ratings yet
- 103 Radionuclide Imaging TechniquesDocument30 pages103 Radionuclide Imaging TechniquesrevanthNo ratings yet
- Ladder Filters, Butterworth & Chebyshev Filters, Filter Tables & Freq/Imp ScalingDocument16 pagesLadder Filters, Butterworth & Chebyshev Filters, Filter Tables & Freq/Imp ScalingShobhit GuptaNo ratings yet
- Dasar Dasar Ekg PDFDocument52 pagesDasar Dasar Ekg PDFBobyNo ratings yet
- Assignment 2Document2 pagesAssignment 2api-306696718No ratings yet
- 01 RV Guidelines Florida - 2017Document37 pages01 RV Guidelines Florida - 2017Harry AndromedaNo ratings yet
- Lecture 6 - TransducersDocument58 pagesLecture 6 - TransducersKOFI BROWNNo ratings yet
- Echocardiography General Principles and ExamplesDocument135 pagesEchocardiography General Principles and Examplesroseneels9100% (1)
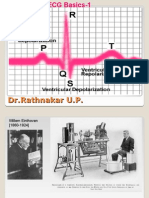
- ECG Basics 1Document24 pagesECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Flow in PipesDocument120 pagesFlow in PipesAnonymous gFAWtLLtNo ratings yet
- Modul EKGDocument101 pagesModul EKGAjeng Dwik01No ratings yet
- 0727 Little - TV TR Severity 1-31 - CCF Miami Feb 2023Document31 pages0727 Little - TV TR Severity 1-31 - CCF Miami Feb 2023hbasrawala110No ratings yet
- ECG Normal - ErwanDocument49 pagesECG Normal - ErwanEvelyne NatalieNo ratings yet
- 04-Role of Echo in Pulm Hypertion N EmbolismDocument57 pages04-Role of Echo in Pulm Hypertion N EmbolismSiska Istanah Wong SintingNo ratings yet
- Umyu Ecg WorkshopDocument55 pagesUmyu Ecg WorkshopzainabhassansadaNo ratings yet
- Systematic Approach To ECGDocument12 pagesSystematic Approach To ECGAmr El TaherNo ratings yet
- ECG - Systematic-ApproachDocument12 pagesECG - Systematic-ApproachMicael MendesNo ratings yet
- ECG InterpretationDocument83 pagesECG InterpretationJuana Maria Garcia Espinoza100% (2)
- ECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial CentreDocument90 pagesECG Interpretation: DR S J Bhosale DM, FPCC (Canada) Associate Professor Tata Memorial Centrevaishali TayadeNo ratings yet
- RV Dysfunction - Assessment by EchocardiographyDocument52 pagesRV Dysfunction - Assessment by EchocardiographyNag Mallesh RaoNo ratings yet
- WFTF Chamber Quantification Summary Doc Final July 18Document18 pagesWFTF Chamber Quantification Summary Doc Final July 18Saloum Muhammed IslamNo ratings yet
- Basics of ElectrocardiographyDocument227 pagesBasics of ElectrocardiographyVlad CarabinNo ratings yet
- Tapas Bag Carotid 22.11.018Document1 pageTapas Bag Carotid 22.11.018dilip kumar bhattacharyaNo ratings yet
- Readecg2010 PDFDocument63 pagesReadecg2010 PDFShiju P SNo ratings yet
- RHC in PH FinalDocument36 pagesRHC in PH FinalKirti KadianNo ratings yet
- Exam 1reference SheetDocument2 pagesExam 1reference SheetAndrea Norton100% (1)
- Cardiovascular Diagnostic Tests and ProceduresDocument48 pagesCardiovascular Diagnostic Tests and ProceduresDr. Rabail MalikNo ratings yet
- Cardiology A Practical Handbook-41-61 Edit 12Document21 pagesCardiology A Practical Handbook-41-61 Edit 12Mahir FikaNo ratings yet
- Hydroxy ZineDocument2 pagesHydroxy ZineSharmaine Grace FlorigNo ratings yet
- Cisco ExámenDocument9 pagesCisco ExámenandreaNo ratings yet
- Discharge Summary: General FormatDocument6 pagesDischarge Summary: General Formatf archiveNo ratings yet
- ARA DraftProgWEBSITE1MayDocument13 pagesARA DraftProgWEBSITE1MayHNNo ratings yet
- Micro paraDocument7 pagesMicro paraAj MillanNo ratings yet
- Boroneant - and - Bonsall Sahranjivanje U Mezolitu DjerdapaDocument14 pagesBoroneant - and - Bonsall Sahranjivanje U Mezolitu DjerdapaMorriganNo ratings yet
- Acknowledgement (Draft 2) : IntroductionDocument3 pagesAcknowledgement (Draft 2) : IntroductionSHAIK AASHIQUE RASOOL ARCH-UG- 2018 BATCHNo ratings yet
- Al Selden Leif - Pagan - Divination - Dice DivinationDocument27 pagesAl Selden Leif - Pagan - Divination - Dice DivinationLuschersUnderworldNo ratings yet
- Pulsar 125Document48 pagesPulsar 125Aayush MahajanNo ratings yet
- TAX 2: Digest - Winebrenner & Iñigo Insurance Brokers, Inc. v. CIRDocument2 pagesTAX 2: Digest - Winebrenner & Iñigo Insurance Brokers, Inc. v. CIRFaith Marie Borden100% (2)
- E Waste RecyclingDocument49 pagesE Waste RecyclingaskmeeNo ratings yet
- Recipe Slow Cooker Chicken TacosDocument10 pagesRecipe Slow Cooker Chicken TacosVincent ReyesNo ratings yet
- West Facing Floor PlansDocument18 pagesWest Facing Floor Plansgurudev001No ratings yet
- B-64120en 02 070508Document462 pagesB-64120en 02 070508Reiko SakurakoNo ratings yet
- 186 ObjectionDocument3 pages186 ObjectionMarsha MainesNo ratings yet
- Evaluating Conflicting Evidence Lesson Summary - History DetectivesDocument5 pagesEvaluating Conflicting Evidence Lesson Summary - History Detectivescorbinmoore1No ratings yet
- English 7 &9Document17 pagesEnglish 7 &9Salve PetilunaNo ratings yet
- DLP Eugelle12Document9 pagesDLP Eugelle12Kim RusteNo ratings yet
- Butterfly CircusDocument2 pagesButterfly CircusSalma BenjellounNo ratings yet
- 'NEXtCARE Corporate Profile 5Document1 page'NEXtCARE Corporate Profile 5Rajesh PotluriNo ratings yet
- Range Guard A Plus Control BoxDocument4 pagesRange Guard A Plus Control Boxyusirwan iwanNo ratings yet
- 1700 Kva Rab Panel SinkronDocument2 pages1700 Kva Rab Panel SinkronIqbal KomengNo ratings yet
- Datasheet (Signal Booster)Document4 pagesDatasheet (Signal Booster)Shrisha BhatNo ratings yet
- WPH03 01 Que 20180113 2Document16 pagesWPH03 01 Que 20180113 2Cka DohaNo ratings yet
- Green Bedding Separator FAN - Parts List - 2017Document9 pagesGreen Bedding Separator FAN - Parts List - 2017Centrifugal SeparatorNo ratings yet
- The Computer Contradictionary - Stan Kelly-BootieDocument249 pagesThe Computer Contradictionary - Stan Kelly-BootiedanielghroNo ratings yet
- Criteria For Laboratory Accreditation in The Field of Volume MetrologyDocument11 pagesCriteria For Laboratory Accreditation in The Field of Volume MetrologyHi Tech Calibration ServicesNo ratings yet
- InDesign ToolsDocument3 pagesInDesign ToolsolywaltNo ratings yet
- Evolution-of-Management-Theory 02 PDFDocument42 pagesEvolution-of-Management-Theory 02 PDFsafiqulislamNo ratings yet